Page 17 of 31
PE22.6 | Pediatric Hypertension — SDL Guide
Learning Objectives
- Define hypertension in children using age, sex, and height-based percentile criteria and distinguish elevated BP from Stage 1 and Stage 2 hypertension
- Classify the aetiology of paediatric hypertension and explain why secondary causes predominate in younger children
- Describe the appropriate technique for blood pressure measurement and the correct cuff size selection in children
- Outline a systematic investigation approach for paediatric hypertension, including when to suspect secondary aetiology
- Formulate a management plan covering lifestyle modification, pharmacotherapy, and emergency management of hypertensive crisis in children
INSTRUCTIONS
Hypertension in children is vastly underdiagnosed because clinicians rarely measure BP in paediatric consultations and, when they do, often apply adult reference values incorrectly. A 10-year-old with BP 130/85 mmHg may be hypertensive by percentile criteria yet go undetected. Uncontrolled childhood hypertension drives premature cardiovascular and renal damage, and secondary causes — particularly renal disease — are correctable if found early. This module gives you the definitional framework, aetiological thinking, and management algorithm needed to detect and act on hypertension at every paediatric encounter.
References
- Ghai Essential Pediatrics, 9th ed., Ch 14 (Cardiovascular System) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 472 (Systemic Hypertension) (textbook)
- IAP Guidelines on Childhood Hypertension, 2013 (guideline)
- AAP Clinical Practice Guideline on High Blood Pressure in Children and Adolescents, 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old boy is brought to the outpatient clinic with a two-week history of recurrent morning headaches and one episode of blurred vision. His mother attributes it to 'too much screen time.' On examination he looks well, weight 42 kg, BMI 24.5 kg/m². When you measure his blood pressure at 138/90 mmHg you initially wonder if you have used the wrong cuff. You repeat it twice over the next 15 minutes with the correct paediatric cuff — both readings are similar. You look up the normative tables and find his reading is well above the 99th percentile for his age, sex, and height. His urine dipstick shows 2+ proteinuria. What is happening, and what do you do next?
WHY THIS MATTERS
Paediatric hypertension is a clinically important and frequently missed diagnosis. Unlike adult hypertension, it is often secondary to a treatable underlying cause — especially in younger children — meaning that detection directly enables cure. Even primary hypertension in adolescents has been shown to lead to early left-ventricular hypertrophy, increased arterial stiffness, and retinal vessel changes that presage adult cardiovascular disease. In India, rising childhood obesity rates are increasing the burden of primary hypertension among adolescents, while infections such as post-streptococcal glomerulonephritis remain a significant secondary cause. Final-year students must be able to recognise, classify, investigate, and initiate management — a complete clinical skill required from the first day of practice.
RECALL
Before proceeding, recall the following from your earlier years: (1) The renin-angiotensin-aldosterone system (RAAS) from physiology — renin, released by juxtaglomerular cells in response to reduced renal perfusion or sodium depletion, drives angiotensin II production, vasoconstriction, and aldosterone release. (2) Renal anatomy — the cortex contains glomeruli and proximal tubules; diseases affecting glomeruli (nephritic, nephrotic) impair filtration and sodium handling, raising BP. (3) The adrenal medulla secretes catecholamines (epinephrine, norepinephrine) — a tumour of these cells (phaeochromocytoma) causes episodic or sustained hypertension. (4) Coarctation of aorta — a narrowing of the aortic arch (most commonly just distal to the left subclavian artery) that causes upper-limb hypertension and lower-limb hypotension with radio-femoral delay. Activate these pathways as you read the aetiological section.
Clinical Presentation and Initial Recognition
Paediatric hypertension is predominantly asymptomatic and detected incidentally during routine or opportunistic blood pressure screening. The majority of children with elevated BP or even Stage 1 hypertension have no symptoms, and this is precisely why systematic measurement at every well-child visit is the only reliable detection strategy. The absence of symptoms must never be used to exclude hypertension. When symptoms do appear, they are usually non-specific: headache (particularly occipital, on waking), visual disturbances (blurring, diplopia, visual field loss), irritability, or fatigue. In severe or acute-onset hypertension — for example, during a hypertensive emergency — children may present with hypertensive encephalopathy, characterised by severe headache, altered consciousness, seizures, or papilloedema. Nausea and vomiting are common accompaniments. In neonates and young infants, hypertension may be entirely silent or manifest as irritability, poor feeding, tachypnoea, or cardiac failure.
On physical examination, key findings that should prompt suspicion of hypertension or a secondary cause include:
• Elevated BP on repeated measurement (see grading section for thresholds)
• Fundoscopic changes — arteriovenous nicking, cotton-wool spots, haemorrhages, papilloedema
• Signs of left-ventricular hypertrophy — displaced apex beat, prominent left ventricular impulse, S4 gallop
• Features suggesting secondary cause: radio-femoral pulse delay (coarctation), abdominal bruit (renovascular), cushingoid features (Cushing's syndrome), café-au-lait spots (neurofibromatosis with renal artery stenosis), palpable kidneys (polycystic kidney disease)
IMPORTANT: Always measure BP in all four limbs when coarctation is suspected — upper limb BP will be higher than lower limb BP.
Secondary Causes of Hypertension in Children
Pathophysiology and Aetiology
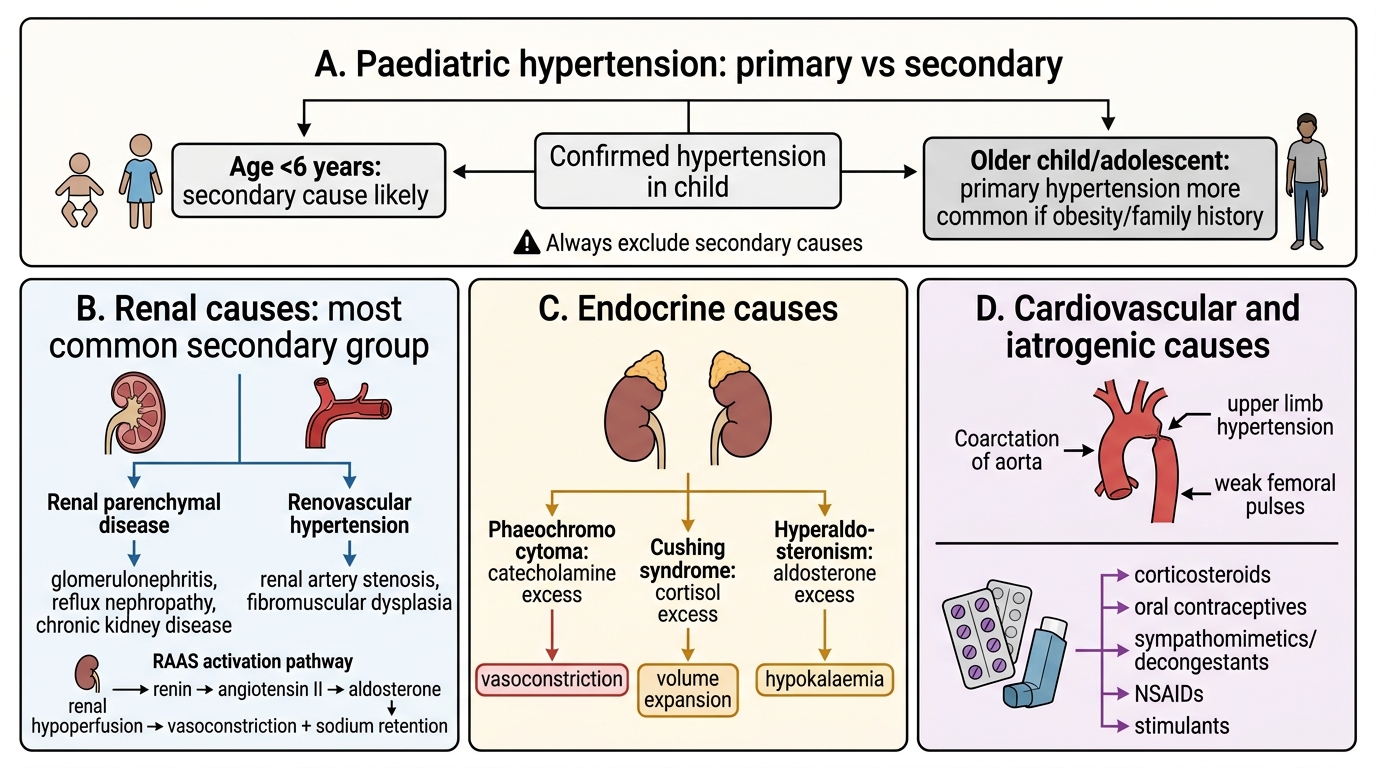
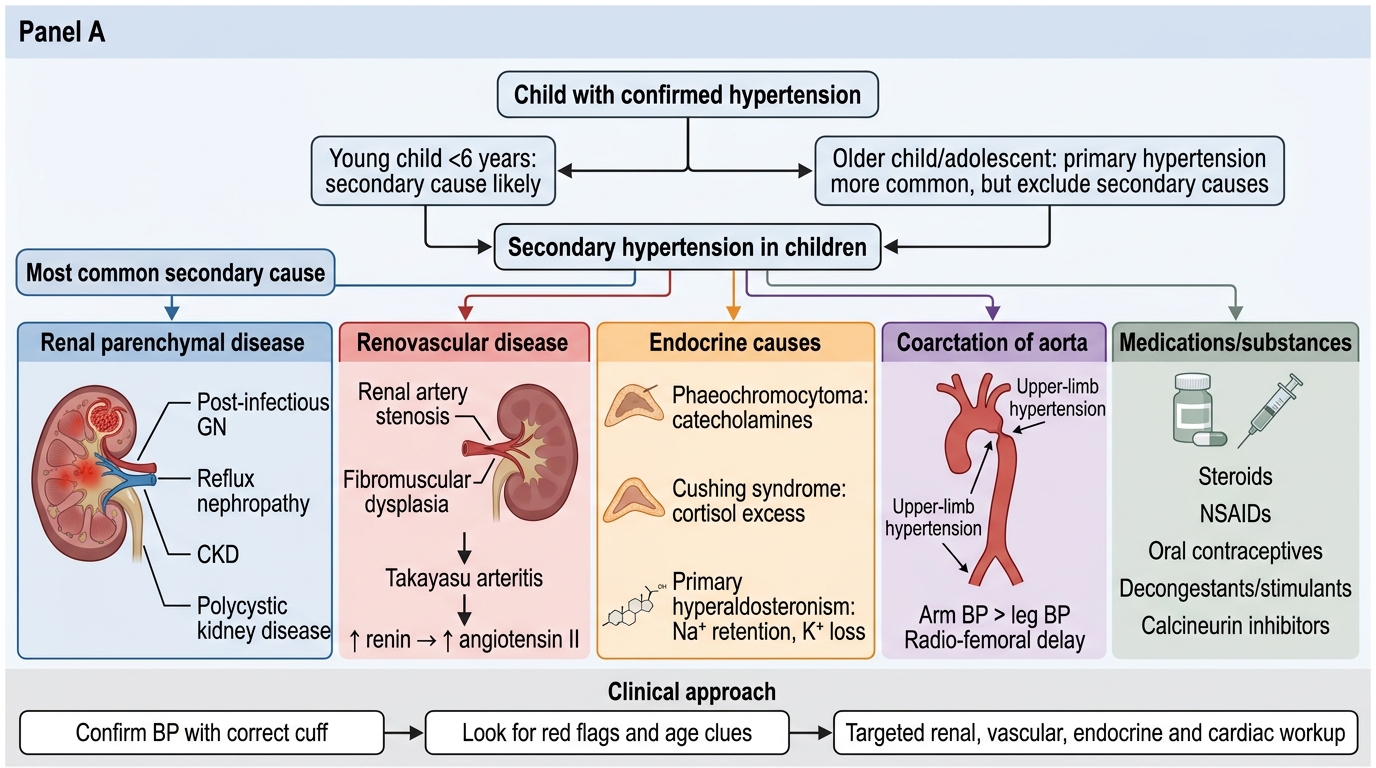
Understanding why hypertension occurs in a child requires a distinction between primary (essential) hypertension and secondary hypertension, and this distinction is critically age-dependent. In young children (under 6 years), secondary hypertension is overwhelmingly more likely — almost every young child with confirmed hypertension has an identifiable underlying cause, most commonly renal. In older children and adolescents, particularly those who are overweight or obese, primary hypertension becomes progressively more common and may represent up to 50% of hypertension in this age group.
Primary (essential) hypertension arises from a polygenic predisposition interacting with environmental drivers — obesity, dietary salt excess, sedentary lifestyle, and stress. Obesity-related hypertension involves hyperinsulinaemia activating the sympathetic nervous system and RAAS, causing sodium retention and increased cardiac output. These children typically have a positive family history, elevated BMI, and no identifiable organic cause after workup.
Secondary hypertension — the most important category in paediatric practice — demands a systematic aetiological framework:
- Renal parenchymal disease (most common secondary cause overall): post-infectious glomerulonephritis, chronic kidney disease from reflux nephropathy, congenital anomalies of the kidney and urinary tract (CAKUT), nephrotic syndrome, polycystic kidney disease, and haemolytic-uraemic syndrome. These conditions impair glomerular filtration and tubular sodium handling, expand extracellular volume, and activate the RAAS.
- Renovascular disease: renal artery stenosis (due to fibromuscular dysplasia, Takayasu's arteritis, or neurofibromatosis type 1) reduces renal perfusion, triggering hyperreninaemia and angiotensin-II-mediated vasoconstriction — a classic mechanism for severe, often drug-resistant hypertension in children.
- Endocrine causes: phaeochromocytoma (catecholamine excess — episodic or sustained hypertension with sweating, palpitations, pallor); Cushing's syndrome (cortisol excess — truncal obesity, striae, glucose intolerance, hypertension); primary hyperaldosteronism (aldosterone excess — hypokalaemia, sodium retention, suppressed renin); congenital adrenal hyperplasia (11β-hydroxylase deficiency causes mineralocorticoid excess and virilisation); hyperthyroidism (increased cardiac output and systolic hypertension).
- Cardiovascular: coarctation of the aorta — mechanical obstruction causes upper-body hypertension with lower-body hypotension; correctable surgically or by balloon dilation.
- Medications and toxins: oral contraceptive pills, systemic steroids, stimulant medications (methylphenidate, amphetamines), non-steroidal anti-inflammatory drugs (NSAIDs), liquorice, and cocaine.
| Age group | Most common causes |
|---|---|
| Neonates | Renal artery thrombosis (umbilical catheter), coarctation, renal parenchymal |
| Infants/toddlers | Coarctation, renal parenchymal disease, renovascular |
| School-age children | Renal parenchymal, renovascular, endocrine |
| Adolescents | Primary (essential), renal parenchymal, endocrine, medications |
Secondary Causes of Hypertension in Children
SELF-CHECK
A 5-year-old child is found to have persistently elevated blood pressure. Which of the following is the most likely aetiology?
A. Primary (essential) hypertension due to obesity
B. Secondary hypertension due to renal parenchymal disease
C. White-coat hypertension with no underlying cause
D. Medication-induced hypertension from antihistamines
Reveal Answer
Answer: B. Secondary hypertension due to renal parenchymal disease
In young children under 6 years, secondary hypertension is overwhelmingly more common than primary hypertension. Renal parenchymal disease is the most frequent secondary cause across all paediatric age groups. Primary (essential) hypertension becomes more common in older children and adolescents, particularly those with obesity and a positive family history. At age 5, a thorough workup for an identifiable secondary cause is always mandated.
Definition and Grading of Hypertension in Children
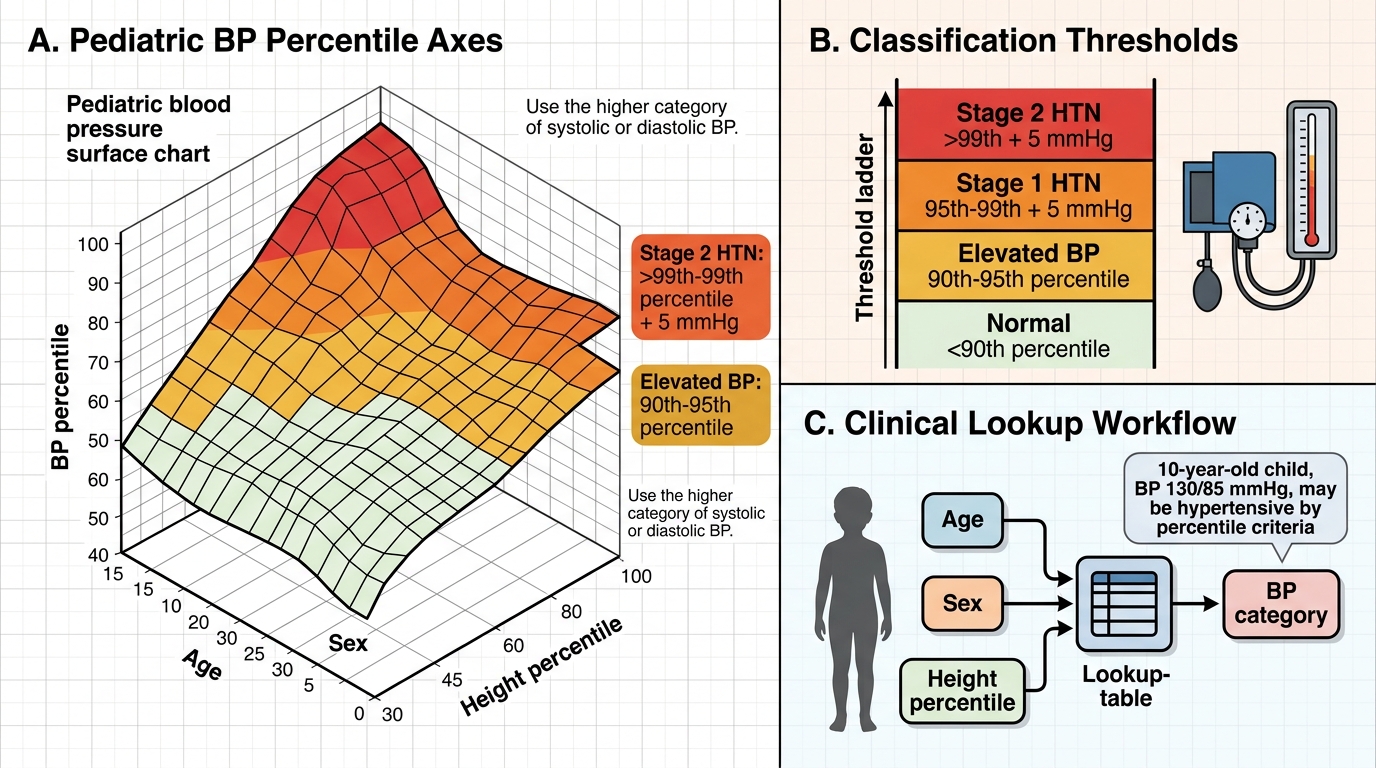
Defining hypertension in children is more complex than in adults because normal blood pressure varies substantially with age, sex, and height. A BP of 120/80 mmHg is entirely normal in an adult but may represent hypertension in a 6-year-old. The gold standard definition is therefore percentile-based, referenced against normative tables that account for all three variables simultaneously.
Definition (IAP / AAP 2017): Hypertension in children aged ≥1 year is defined as an average systolic or diastolic BP ≥95th percentile for age, sex, and height, measured on three separate occasions. The three-occasion rule is critical — a single elevated reading may reflect acute anxiety, pain, discomfort (the 'white-coat effect'), or a measurement error. A single elevated reading in a well child warrants repeat; true hypertension requires confirmation across visits.
BP classification in children (≥1 year):
- Normal BP: <90th percentile
- Elevated BP (previously called 'pre-hypertension'): 90th–<95th percentile OR ≥120/80 mmHg (whichever is lower in older children and adolescents)
- Stage 1 Hypertension: 95th–99th percentile + 5 mmHg
- Stage 2 Hypertension: >99th percentile + 5 mmHg
- Hypertensive urgency: Stage 2 HTN without acute end-organ damage
- Hypertensive emergency: Severe HTN with acute end-organ damage (encephalopathy, acute LVF, acute renal failure, retinopathy)
Pediatric Blood Pressure Classification by Percentiles
Blood pressure measurement technique — mandatory precision: Correct technique is essential because errors in measurement are a major source of both over- and under-diagnosis. The child should be seated quietly for 5 minutes in a calm environment. The arm should be supported at heart level. The standard auscultatory method using a properly calibrated mercury or aneroid sphygmomanometer (or a validated oscillometric device) should be used. The right arm is preferred to allow comparison with published normative tables and to avoid missing coarctation (right arm BP may be higher if the coarctation is between the right and left subclavian origins).
Correct cuff size is perhaps the single most important technical requirement:
- The inflatable bladder width should be at least 40% of the arm circumference (mid-point between olecranon and acromion)
- The bladder length should cover 80–100% of the arm circumference
- An undersized cuff falsely elevates the reading; an oversized cuff may falsely lower it
- In practice: use neonatal, infant, child, and adult small/standard/large cuffs as appropriate; never use an adult cuff on a young child
Korotkoff phase I (first sound) = systolic BP; Korotkoff phase V (disappearance of sounds) = diastolic BP. In young children, sounds may persist to zero — in such cases, use phase IV (muffling) as diastolic.