Page 11 of 42
PE23.{4,6-8} | Acute Gastroenteritis — SDL Guide (Part 2)
Investigations: Stool Examination and Laboratory Tests
Most children with uncomplicated acute watery diarrhoea do not require any investigation — the diagnosis is clinical, and management with ORS and zinc is initiated immediately. Investigations are reserved for dysentery (to identify the pathogen), prolonged or persistent diarrhoea, and when complications (AKI, electrolyte disturbance) are suspected. Over-investigation in straightforward AGE wastes resources, delays treatment, and falsely reassures when a result is negative. The skill the clinician must develop is knowing precisely which children need which investigation — and why that investigation will change management. The two key investigations in paediatric AGE are the stool examination (especially the Hanging Drop Preparation for motility) and the serum electrolytes and renal function tests for complications. Both are described in detail below.
Stool Examination — the core skill (PE23.8):
Macroscopic: Colour (pale/yellow/green); consistency (watery, soft, formed); blood (bright red = lower, dark = upper); mucus; undigested food; offensive odour (rotavirus), watery and pale (cholera).
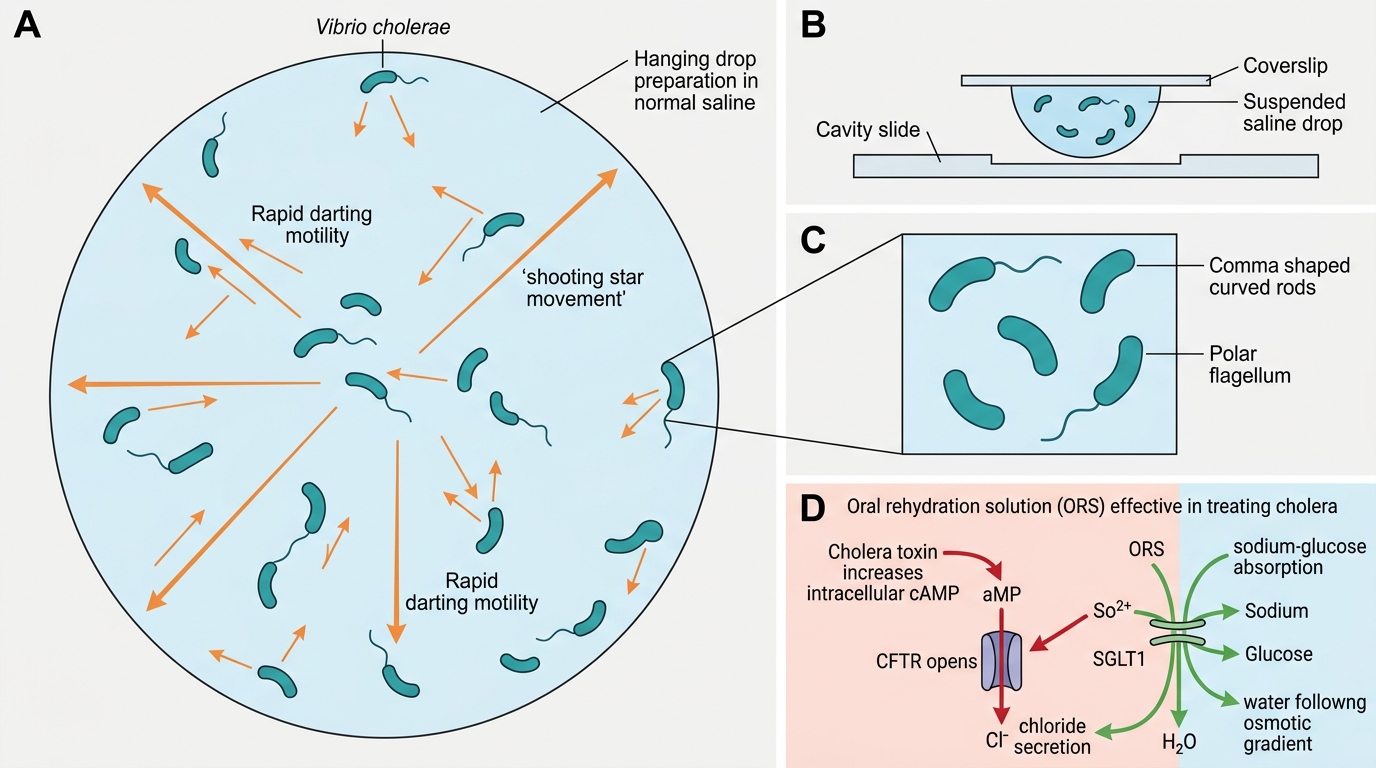
Hanging Drop Preparation (for motility):
This is the most specific rapid bedside test for Vibrio cholerae and Giardia.
1. Place one small drop of freshly passed liquid stool on a glass slide
2. Add a drop of normal saline (0.9%)
3. Cover with a coverslip — do NOT press down
4. Examine under low-power then high-power microscopy immediately (within 10–15 minutes of stool passage — motility diminishes rapidly)
5. Interpretation:
- Vibrio cholerae: Rapid darting motility — the classic description is 'shooting star' or 'shooting comet' — rapid, to-and-fro motion across the field. The comma-shaped curved rods are visible at 40× and are actively motile.
- Giardia: Pear-shaped or piriform trophozoites with characteristic 'falling leaf' or 'tumbling' motility; two nuclei visible in trophozoites on stained preparations
- Adding a drop of anti-O1 antiserum to the preparation and observing cessation of motility confirms V. cholerae serotype O1 (Pfeiffer phenomenon)
- Important: Sample must be fresh. Refrigeration and delay abolish motility. A negative Hanging Drop does NOT exclude V. cholerae — culture is the gold standard.
Microscopy (wet mount/concentration technique):
- Pus cells (polymorphonuclear leucocytes): ≥5 per high-power field suggests invasive diarrhoea (Shigella, EIEC, Campylobacter, Entamoeba)
- Red blood cells: Invasive pathogen
- Trophozoites of Entamoeba histolytica: Active, pseudopod-extending trophozoites containing ingested red blood cells (erythrophagocytosis) — PATHOGNOMONIC for amoebic dysentery
- Cysts: Entamoeba cysts (4 nuclei), Giardia cysts (4 nuclei, oval), Cryptosporidium oocysts (modified Ziehl-Neelsen stain)
- Ova and larvae: Hookworm, Ascaris, Strongyloides
Culture and sensitivity: Required for persistent diarrhoea, outbreak investigation, or dysentery unresponsive to empirical therapy.
Renal function tests (RFT) and electrolytes in the context of diarrhoea:
- Prerenal AKI pattern: Elevated serum urea and creatinine in proportion to dehydration; urea:creatinine ratio >20:1 (renal retention of urea); urine sodium <20 mEq/L; fractional excretion of sodium (FeNa) <1%; urine osmolality >500 mOsm/kg; urine specific gravity >1.025. This pattern reverses with rehydration — if it does not, intrinsic renal injury (HUS) must be considered.
- Hyponatraemia (Na <135 mEq/L): Common in diarrhoea; causes — sodium loss in stool exceeding water loss, or excessive intake of hypotonic fluids (diluted ORS, plain water). Clinical: lethargy, weakness, seizures if Na <125. Correction must be gradual (≤0.5 mEq/L/hour) to avoid cerebral oedema or demyelination.
- Hypokalaemia (K <3.5 mEq/L): Potassium is lost in profuse diarrhoea and in aldosterone-mediated renal potassium excretion; ORS contains 20 mEq/L of potassium which partially replaces losses; IV fluids in Plan C include potassium once urine output is confirmed.
- Metabolic acidosis: Low bicarbonate, low pH — from bicarbonate-rich stool losses plus lactic acidosis in shock. Ringer's Lactate (the preferred Plan C fluid) provides lactate which is converted hepatically to bicarbonate.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Vibrio cholerae Hanging Drop Motility and ORS Mechanism
CLINICAL PEARL
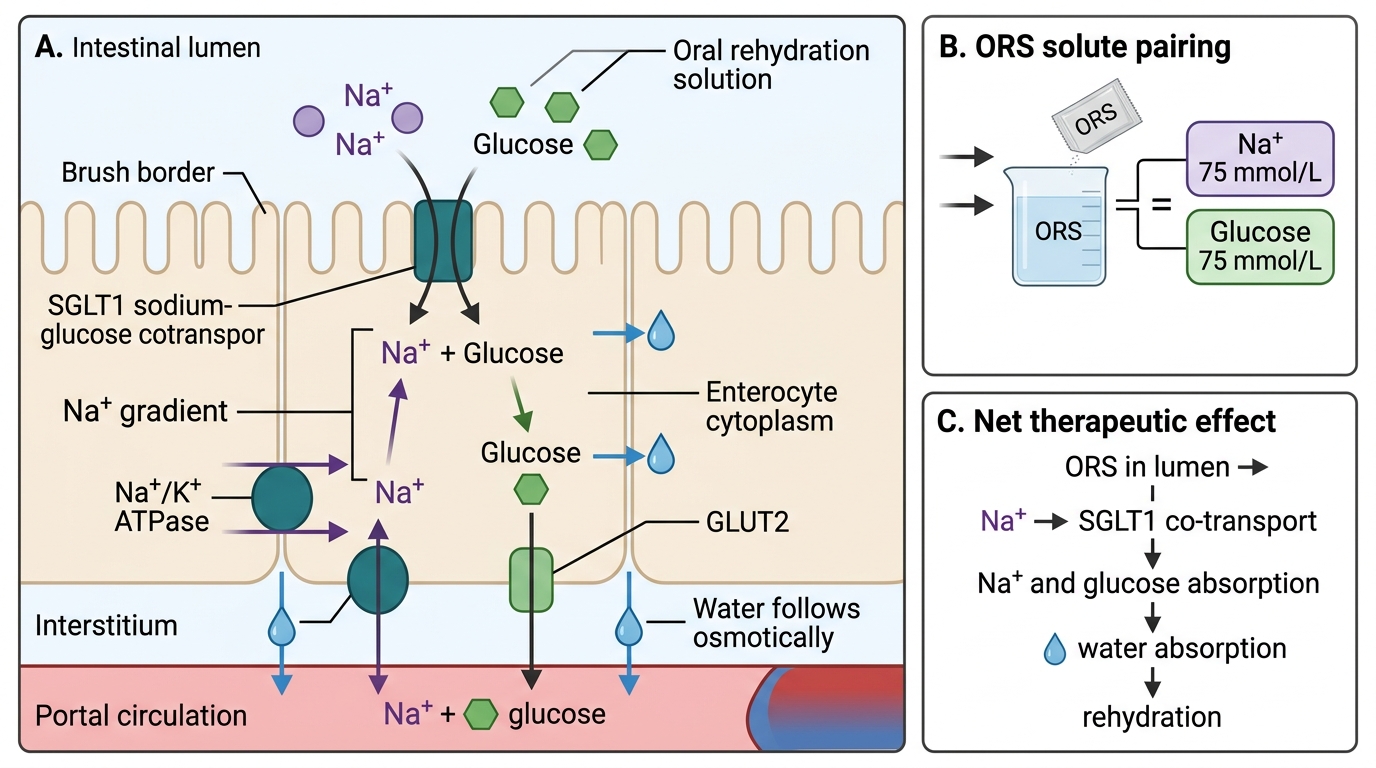
ORS works because cholera toxin cannot turn off glucose-coupled sodium absorption. The cholera toxin activates adenylate cyclase, raises cAMP, and locks the chloride channel (CFTR) open — the gut secretes litres of fluid. But the sodium-glucose cotransporter (SGLT1) uses a different, cAMP-independent mechanism. When glucose is present in the lumen (as in ORS), SGLT1 actively co-transports sodium and glucose into the enterocyte, dragging water with it by osmosis. This is why ORS can treat cholera even in the middle of maximal cholera toxin activity. The WHO's formulation of reduced-osmolarity ORS (245 mOsm/L: Na 75, K 20, glucose 75, citrate 10 mmol/L) exploits this mechanism optimally — lower osmolarity reduces the osmotic load in the lumen and results in less vomiting and less stool output than the older standard ORS.
ORT: Physiological Basis, ORS Types, and Fluid Management
Oral rehydration therapy (ORT) is one of the greatest public health innovations of the 20th century, estimated to have saved more than 50 million children's lives since its introduction. Its physiological basis — the preserved glucose-sodium cotransport in secretory diarrhoea — has been described above. The clinical application hinges on choosing the right ORS plan, administering it correctly, and continuing feeding. A common clinical error is to reserve ORS only for mild cases and move immediately to IV fluids for any child who vomits or appears unwell. This is wrong in two ways: ORS is effective even in the presence of vomiting (small sips at 5 mL/minute overcome most vomiting), and IV fluids carry their own risks (electrolyte imbalance, infection, fluid overload). The WHO ORS Plans A, B, and C provide a graduated, evidence-based framework that matches the intervention to the severity of dehydration — and the clinician's role is to prescribe the correct plan based on the IMNCI assessment.
ORS composition and types:
The WHO/UNICEF reduced-osmolarity ORS (245 mOsm/L) is the current standard:
- Sodium: 75 mmol/L
- Potassium: 20 mmol/L
- Glucose: 75 mmol/L
- Citrate: 10 mmol/L
- Chloride: 65 mmol/L
- Total osmolarity: 245 mOsm/L
This replaced the older standard ORS (311 mOsm/L) because the reduced-osmolarity formulation results in significantly less vomiting and reduced stool output, reducing the need for IV fluids by 33%. It is the formulation used in all government ORS packets in India (ORS packets at PHCs, CHCs, and hospitals contain this formulation).
Home fluids (Plan A): Acceptable alternatives at home include rice water (kanji), lassi, salted lemon water, coconut water, or daal water — any age-appropriate oral fluid that can be given in adequate volumes. However, plain water alone without electrolytes is insufficient and can cause hyponatraemia.
WHO ORS Plans:
Plan A — Home-based (NO dehydration):
- Give extra fluid at home: for children <2 years = 50-100 mL after each loose stool; for children 2-10 years = 100-200 mL; for children >10 years = as much as desired
- Continue breastfeeding
- Continue feeding — do NOT fast the child
- Return signs: child cannot drink, worsens, blood in stool, high fever
Plan B — Supervised facility-based (SOME dehydration):
- Administer 75 mL/kg of ORS over 4 hours in a health facility under supervision
- Give frequently in small sips (by spoon in infants); if vomiting, wait 10 minutes then restart at slower pace (5 mL/minute)
- Reassess dehydration after 4 hours — if improved to 'no dehydration' → transition to Plan A; if still 'some dehydration' → repeat Plan B; if 'severe' → Plan C
- Do NOT use sugary drinks (sodas, fruit juice) — their high osmolarity worsens diarrhoea
Plan C — Rapid IV rehydration (SEVERE dehydration):
- Use Ringer's Lactate (preferred) or normal saline
- Children <12 months: 30 mL/kg IV in 1 hour, then 70 mL/kg in 5 hours (total 100 mL/kg in 6 hours)
- Children ≥12 months: 30 mL/kg IV in 30 minutes, then 70 mL/kg in 2.5 hours (total 100 mL/kg in 3 hours)
- Reassess every 15-30 minutes; if radial pulse not detectable, give more rapidly
- As soon as the child can drink, start ORS alongside IV fluids (5 mL/kg/hour)
- After completion of Plan C, reassess and decide on Plan B or A
Continuing feeding during diarrhoea:
Feeding must NOT be stopped during diarrhoea. Continued breastfeeding reduces diarrhoea duration, maintains intestinal villi, and provides immunological protection. For non-breastfed children, age-appropriate foods should continue. Lactose-free formula is not routinely required unless clinical lactose intolerance is evident (perianal excoriation, acidic stool, positive clinitest).
SGLT1-Mediated Glucose-Sodium Cotransport in ORS Therapy
Drug Therapy in Acute Gastroenteritis
Pharmacological therapy in acute gastroenteritis is highly targeted — most drugs that appear on the surface to be reasonable treatments for diarrhoea are either ineffective or harmful in children. The evidence-based pharmacological interventions are zinc supplementation (universal for all children with diarrhoea) and antibiotics (only for specific indications — dysentery and cholera). All other drugs commonly prescribed for diarrhoea in clinical practice — antidiarrhoeals, antispasmodics, antisecretory agents — have either no evidence of benefit or are actively harmful in children and should not be prescribed.
Zinc supplementation — WHO/UNICEF 2004 recommendation:
Zinc is an essential micronutrient required for intestinal epithelial repair, immune function, and maintenance of gut integrity. Children in low- and middle-income countries are frequently zinc-deficient. Zinc supplementation during AGE has been shown in randomised controlled trials to reduce the duration and severity of diarrhoeal episodes by approximately 25% and reduce the probability of the episode persisting beyond 7 days by 24%. WHO/UNICEF recommend zinc for all children with diarrhoea:
- Children >6 months: 20 mg elemental zinc per day for 14 days (even after diarrhoea resolves — to replenish body stores and reduce the risk of future episodes)
- Children <6 months: 10 mg per day for 14 days
- Formulation: Zinc sulphate dispersible tablet (dissolved in ORS or breast milk); zinc acetate syrup
- Note: 14 days is the full course — stopping at resolution of diarrhoea is a common error
Antibiotics — indicated ONLY for:
- Dysentery (bloody diarrhoea): Empirical treatment targeting Shigella — azithromycin (first-line for children: 10 mg/kg once daily × 3 days) or ciprofloxacin (as per local resistance patterns). Do NOT use ampicillin or co-trimoxazole (widespread Shigella resistance in India).
- Confirmed/suspected cholera: Single-dose antibiotic — azithromycin 20 mg/kg (max 1 g) as a single dose for children; reduces duration and carriage. Alternative: doxycycline (>8 years, 300 mg single dose).
- Giardiasis: Metronidazole 15 mg/kg/day in 3 divided doses × 5-7 days
- Amoebic dysentery: Metronidazole (tissue amoebicide) followed by diloxanide furoate (luminal amoebicide)
- Salmonella: Antibiotics only for systemic disease, children <3 months, immunocompromised, haemoglobinopathy
Drugs NOT recommended in routine AGE:
- Antidiarrhoeals (loperamide): CONTRAINDICATED in children under 2 years; associated with paralytic ileus, toxic megacolon, and deaths in young children; not recommended in any age group in developing countries
- Antispasmodics (atropine derivatives, dicyclomine): No evidence of benefit; cause sedation, hyperthermia, and ileus in infants; CONTRAINDICATED in children under 6 months
- Antisecretory agents (bismuth, racecadotril): Racecadotril (enkephalinase inhibitor) has modest evidence in reducing stool output in some settings but is not part of standard WHO/IAP protocols; bismuth not recommended
- Routine antiemetics: Ondansetron has evidence for reducing vomiting and improving ORS tolerance (single oral dose 0.15 mg/kg); use selectively where vomiting prevents ORS administration — not as routine
- Probiotics: Lactobacillus rhamnosus GG and L. reuteri have modest evidence for reducing AGE duration by approximately 1 day; not part of standard WHO/IAP protocol; may be considered as an adjunct
| Drug/Category | Recommendation | Dose | Evidence |
|---|---|---|---|
| Zinc (>6 months) | Recommended universally | 20 mg/day × 14 days | Strong (WHO/UNICEF) |
| Zinc (<6 months) | Recommended | 10 mg/day × 14 days | Strong |
| Antibiotics | Dysentery/cholera ONLY | Azithromycin (per protocol) | Targeted |
| Loperamide | CONTRAINDICATED <2 years | — | Harmful in children |
| Antispasmodics | NOT recommended | — | No benefit, harmful |
| Racecadotril | Not standard protocol | — | Limited |
| Probiotics | Adjunct only | — | Modest |
SELF-CHECK
A 2-year-old child has had watery diarrhoea for 3 days. On IMNCI assessment: awake but irritable, eyes moderately sunken, drinking eagerly, skin pinch returns slowly (2 seconds). Weight is 12 kg. What is the CORRECT management plan?
A. Oral Rehydration Plan A: give extra fluids at home and return if worse
B. Oral Rehydration Plan B: 75 mL/kg ORS over 4 hours = 900 mL ORS in facility
C. Intravenous Ringer's Lactate 30 mL/kg in 30 minutes then 70 mL/kg in 2.5 hours
D. Nil by mouth and immediate IV access due to irritability
Reveal Answer
Answer: B. Oral Rehydration Plan B: 75 mL/kg ORS over 4 hours = 900 mL ORS in facility
This child has SOME dehydration (two or more of: irritable/restless, sunken eyes, drinks eagerly/thirsty, skin pinch slow 1-2 seconds). SOME dehydration requires ORS Plan B: 75 mL/kg over 4 hours in a health facility. For a 12 kg child: 75 × 12 = 900 mL of reduced-osmolarity ORS given by mouth over 4 hours, with supervision. Reassess at 4 hours. Plan A is for no dehydration; Plan C (IV Ringer's Lactate) is for SEVERE dehydration (lethargic/unconscious + cannot drink + skin pinch very slow >2 seconds). The child's irritability here reflects dehydration, not altered consciousness — IV fluids are not yet indicated.