Page 23 of 42
PE23.13 | Acute Hepatitis — SDL Guide
Learning Objectives
- Describe the clinical stages of acute viral hepatitis and recognise the signs and symptoms that distinguish uncomplicated hepatitis from acute liver failure
- Identify the major viral and non-viral causes of acute hepatitis in Indian children and explain their transmission routes
- Interpret standard hepatitis serology (IgM anti-HAV, HBsAg, IgM anti-HBc, IgM anti-HEV) and liver function tests to diagnose the aetiology of acute hepatitis
- Outline the management of uncomplicated acute viral hepatitis and the emergency management of acute liver failure
- Recognise the special risk of Hepatitis E in pregnancy and describe the prevention of Hepatitis A through vaccination and hygiene
INSTRUCTIONS
Acute hepatitis is one of the commonest causes of jaundice in Indian children. Hepatitis A virus accounts for the majority of acute viral hepatitis in children in India — a country where faeco-oral transmission flourishes in settings with limited access to clean water and sanitation. While most cases are self-limiting, the clinical imperative is to identify the minority who are developing acute liver failure — a rapidly lethal condition that requires urgent recognition, supportive management, and timely referral to a liver transplant centre. Hepatitis E has a special danger in pregnant women that the clinician must communicate clearly.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 13 (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Ch 385–386 (textbook)
- IAP Guidelines on Viral Hepatitis in Children (guideline)
- APASL Guidelines on Acute Liver Failure in Children, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 8-year-old boy is brought to the paediatric OPD with 5 days of fever, nausea, vomiting, and poor appetite. His mother noticed 2 days ago that his eyes had turned yellow and his urine was dark. He attends a school with a communal water supply that was recently reported to have contamination. On examination, he is mildly icteric, his liver is enlarged and tender (4 cm below the right costal margin), and his spleen is just palpable. You order a bilirubin (total 7.2 mg/dL, direct 5.1 mg/dL) and liver enzymes (ALT 820 U/L, AST 740 U/L). He is alert and fully oriented. His prothrombin time is 14 seconds (control 13 seconds). What is the most likely cause, what single test confirms the acute infection, and what two features, if they appeared, would tell you this child is developing acute liver failure?
WHY THIS MATTERS
Hepatitis A virus is the commonest cause of acute viral hepatitis in children in India and is a vaccine-preventable disease. Despite being generally self-limiting, it is a major source of school absenteeism, family disruption, and hospital admissions. The real clinical danger is not the typical case but the 1–2% who develop acute liver failure — a condition where the window between recognition and death can be measured in hours to days. Hepatitis E, though less common, carries a disproportionate mortality risk in pregnant women (case-fatality rate up to 20–25% in the third trimester in endemic settings) — a fact you must communicate to mothers and pregnant women in communities with contaminated water supplies. Hepatitis B, transmitted via blood and mother-to-child routes, causes both acute and chronic liver disease and is preventable by universal newborn vaccination. Understanding the aetiology-specific serology allows you to give a family an accurate diagnosis, prognosis, and infection-control advice.
RECALL
Before engaging with this module, consolidate your knowledge of hepatic physiology. The liver serves five critical functions that become clinically apparent when they fail: (1) protein synthesis — albumin (oncotic pressure) and clotting factors (PT/INR measures this; Vitamin K-dependent factors II, VII, IX, X); (2) bilirubin metabolism — conjugation of indirect bilirubin to direct, excretion via bile; (3) detoxification — ammonia cleared to urea; in hepatic failure, ammonia accumulates causing encephalopathy; (4) carbohydrate metabolism — gluconeogenesis maintains blood glucose; hypoglycaemia is a complication of ALF; (5) drug metabolism — Phase I and II reactions. Recall the jaundice classification: pre-hepatic (elevated indirect/unconjugated bilirubin from haemolysis), hepatic (elevated both; hepatocellular injury), post-hepatic (elevated direct/conjugated; obstruction). Recall that ALT (alanine aminotransferase) is the most liver-specific enzyme and is elevated in hepatocellular damage; ALP (alkaline phosphatase) rises more in cholestatic/obstructive conditions. PT/INR reflects synthetic function of the liver — prolongation indicates severe dysfunction.
Clinical Presentation of Acute Hepatitis
Acute viral hepatitis in children follows a characteristic clinical course divided into three phases, though the presentation can range from subclinical (the majority of HAV infections in young children) to fulminant liver failure. Recognising each phase and knowing when to escalate management is the key clinical skill.
Prodromal phase (1–2 weeks before jaundice): This is the pre-icteric phase, dominated by constitutional and gastrointestinal symptoms. The child presents with fever (typically 38–39°C), malaise, anorexia, nausea, vomiting, and abdominal discomfort — particularly in the right upper quadrant. These symptoms are frequently attributed to a 'stomach virus' or 'fever' by parents and even clinicians, delaying recognition. Arthralgia, urticaria, and a serum-sickness-like picture can occur with Hepatitis B during this phase (due to immune complex deposition).
Icteric phase (jaundice phase): As hepatocellular damage progresses, conjugated bilirubin accumulates and the child develops jaundice — yellowing of the sclera (earliest sign) and skin. Dark urine (bilirubinuria — direct bilirubin is water-soluble and excreted in urine) and pale/acholic stools (reduced stercobilinogen from impaired bile excretion) appear at the onset of jaundice. Paradoxically, constitutional symptoms may improve when jaundice appears. The liver is enlarged and tender. Splenomegaly occurs in ~20% of cases. Pruritus (from bile salt deposition in skin) can occur. The icteric phase lasts 2–6 weeks in HAV.
Convalescence phase: Jaundice fades, appetite returns, and liver size normalises over weeks to months. HAV causes complete resolution — it does NOT cause chronic hepatitis. HBV causes chronic hepatitis in a small proportion of adults but in a significantly higher proportion of perinatally-infected children (~90%) and young children (~30%) — this age-dependent risk of chronicity is a critical teaching point.
Acute liver failure (ALF): The most feared complication of acute hepatitis. ALF is defined as hepatic encephalopathy + coagulopathy (INR >1.5) within 8 weeks of onset in a child without prior known liver disease. Key warning signs:
- Deepening jaundice with liver shrinkage (not enlargement — progressive hepatocyte necrosis).
- Encephalopathy: earliest stage = reversal of sleep rhythm, irritability, confusion; advanced = drowsiness, stupor, coma.
- Coagulopathy: bleeding gums, petechiae, prolonged PT/INR (synthetic failure).
- Hypoglycaemia: gluconeogenesis fails; check blood glucose frequently in suspected ALF.
- Ascites and oedema.
- Fetor hepaticus: sweet-musty breath from exhaled mercaptans.
ALF is a medical emergency requiring immediate transfer to a specialised paediatric liver centre.
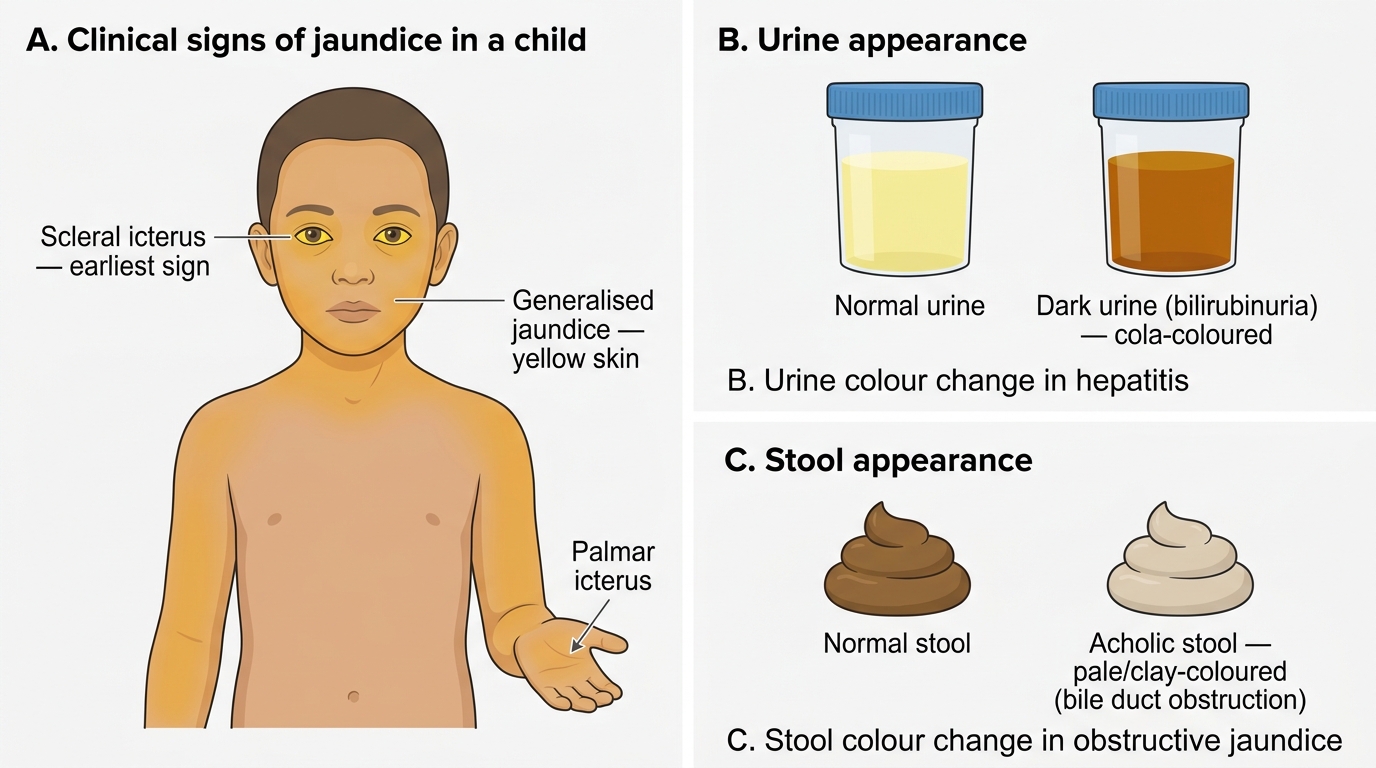
Clinical Signs of Jaundice in a Child: Scleral Icterus, Skin Discolouration, and Urine/Stool Changes
Pathogenesis and Aetiology
Understanding the pathogenic mechanism of hepatic injury in each viral and non-viral cause explains both the natural history and the rationale for management decisions — particularly why antiviral therapy is applicable in some cases and not others.
Hepatitis A virus (HAV): An RNA virus transmitted via the faeco-oral route — contaminated water, food (especially raw shellfish, unwashed produce), and person-to-person contact. HAV is the commonest cause of acute hepatitis in Indian children, reflecting the prevalence of poor sanitation and contaminated water in many communities. After ingestion, HAV replicates in the liver and is shed in faeces for 1–2 weeks BEFORE jaundice appears (the peak infectious period is in the prodromal phase — when the child is at school, unaware they are contagious). HAV causes hepatocyte injury primarily through CD8+ cytotoxic T-lymphocyte-mediated immune attack, not direct cytopathic effect. Importantly, HAV never causes chronic hepatitis and has no carrier state.
Hepatitis E virus (HEV): Another RNA virus transmitted faeco-orally, important in India, particularly in water-borne outbreaks. The natural history in children is similar to HAV — self-limiting in most. The critical special danger is in pregnancy: HEV infection in the third trimester causes fulminant hepatic failure in up to 20–25% of cases, with high maternal and fetal mortality. The mechanism is not fully understood but appears to involve immune dysregulation in pregnancy combined with direct viral cytopathic effects.
Hepatitis B virus (HBV): A DNA virus transmitted via blood (transfusion, needles, sexual contact) and vertically (mother-to-child) at birth — the dominant route in India. The risk of developing chronic HBV is inversely related to age at infection: perinatally infected neonates have ~90% risk of chronicity, children infected at age 1–5 years ~30%, adults ~5%. Acute HBV hepatitis in children is therefore less common because most perinatal acquisitions establish chronic infection from the start. HBV hepatocellular injury is primarily immune-mediated (CD8+ T cells) rather than direct viral cytopathic.
Drug-induced hepatitis: Paracetamol (acetaminophen) overdose is the most important cause of drug-induced ALF in children — toxic metabolite NAPQI overwhelms glutathione stores and causes massive hepatocyte necrosis. Other hepatotoxic drugs include INH (isoniazid), valproate (especially in children with metabolic disorders), tetracycline, and antifungals. Always take a drug history in any child with acute hepatitis.
Wilson's disease: Autosomal recessive copper overload (ATP7B gene); can present in children/adolescents as acute hepatitis with haemolytic anaemia. Slit-lamp examination for Kayser-Fleischer rings and serum caeruloplasmin are key tests. Wilson's presenting as ALF has a very high mortality without liver transplantation.
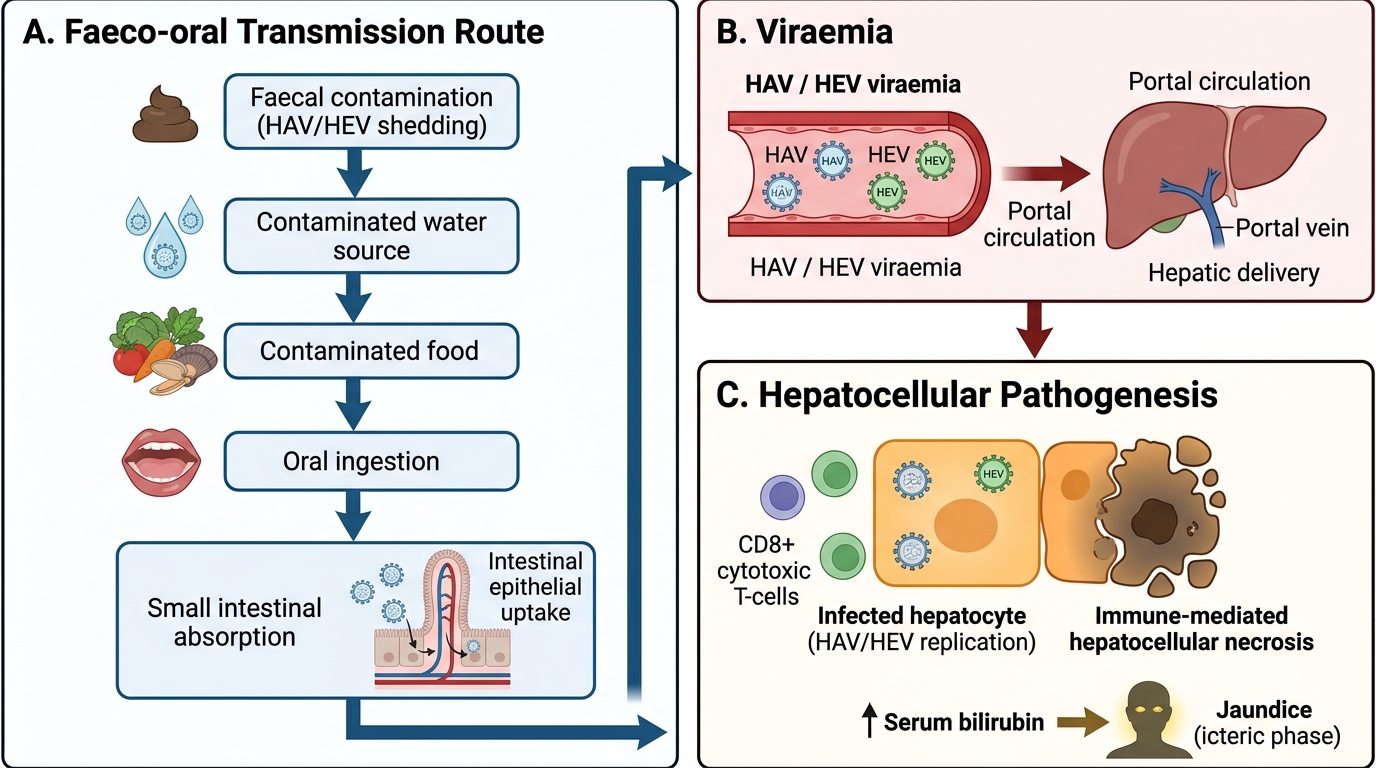
Hepatitis A and E: Faeco-oral Transmission and Immune-Mediated Pathogenesis
SELF-CHECK
A 9-year-old girl has acute hepatitis with jaundice. Her serology shows: IgM anti-HAV positive, HBsAg negative, IgM anti-HBc negative. What is the diagnosis and what is the expected natural history?
A. Acute Hepatitis B — may progress to chronic hepatitis in 5–10% of cases
B. Acute Hepatitis A — complete recovery expected with no chronic infection
C. Acute Hepatitis B — high risk of chronic infection in children
D. Hepatitis E — high risk of fulminant hepatic failure
Reveal Answer
Answer: B. Acute Hepatitis A — complete recovery expected with no chronic infection
IgM anti-HAV positive = acute Hepatitis A infection. HAV does not cause chronic hepatitis — recovery is complete. The icteric phase resolves over 2–6 weeks, with no carrier state and no chronic sequelae. Hepatitis B would show HBsAg and/or IgM anti-HBc positivity. Hepatitis E would show IgM anti-HEV positivity. While HAV rarely causes ALF in immunocompetent children, the expected outcome for typical acute HAV in a school-age child is complete recovery.
Diagnosis and Investigation
The diagnostic workup for acute hepatitis is structured around three simultaneous clinical goals that must be pursued in parallel, not sequentially: confirming hepatocellular injury, identifying the causative agent, and assessing the severity of liver dysfunction to detect early acute liver failure before it becomes irreversible. In practice, a standard panel of LFTs, viral serology, and INR can answer all three questions from a single blood draw, making the investigation both efficient and informative. The specific serology ordered depends on the clinical context — in India, most acute hepatitis in children is HAV, making IgM anti-HAV the first test; however, HBsAg and IgM anti-HBc should be added in any child with risk factors for HBV exposure (unvaccinated, blood transfusion history, mother HBsAg-positive). HEV serology (IgM anti-HEV) is important in outbreak settings and in any pregnant woman with acute hepatitis.
Liver function tests (LFTs) — assess severity and pattern:
- ALT and AST: elevated in hepatocellular injury. In acute viral hepatitis, ALT/AST typically rises 10–100 times above normal (>10× ULN = hepatocellular pattern). ALT is more liver-specific than AST.
- Bilirubin (total and direct): predominantly conjugated (direct) hyperbilirubinaemia in hepatocellular disease. Bilirubin >3 mg/dL produces clinical jaundice.
- PT/INR: most critical test for assessing hepatic synthetic function. A prolonged PT (INR >1.5) indicates significant liver dysfunction and is a component of the ALF definition.
- Serum albumin: low albumin suggests chronicity or severe acute disease — albumin has a half-life of 20 days, so acute illness may not reduce it initially.
- Blood glucose: check in any child with acute hepatitis and altered mental status — hypoglycaemia is a complication of ALF.
- Ammonia: elevated in hepatic failure; correlates with degree of encephalopathy.
Viral serology — identify the cause:
The correct serology markers are high-yield and frequently tested:
- Hepatitis A: IgM anti-HAV = acute infection (detectable from symptom onset, persists 3–6 months); IgG anti-HAV = past infection or vaccination (protective).
- Hepatitis B: HBsAg = current HBV infection (acute or chronic); IgM anti-HBc = acute HBV infection; HBeAg = high replication and infectivity; anti-HBs = protective antibody (past infection or vaccination).
- Hepatitis E: IgM anti-HEV = acute HEV infection.
- EBV: Paul-Bunnell test (heterophile antibody) or EBV-specific antibodies (IgM anti-VCA) for infectious mononucleosis hepatitis.
- CMV: CMV-IgM for cytomegalovirus hepatitis.
Additional investigations:
- Ultrasound abdomen: confirms hepatomegaly, assesses liver echogenicity, excludes biliary obstruction or cholelithiasis.
- Complete blood count: leucopaenia or leucocytosis (atypical lymphocytes in EBV), anaemia (haemolytic in Wilson's disease).
- Urine dipstick: bilirubinuria (direct bilirubin in urine, 'cola-coloured urine').
- Serum caeruloplasmin and 24-hour urine copper: if Wilson's disease is suspected (teenage, haemolysis + hepatitis).
- Drug history and drug levels: if drug-induced hepatitis is possible (paracetamol levels).
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
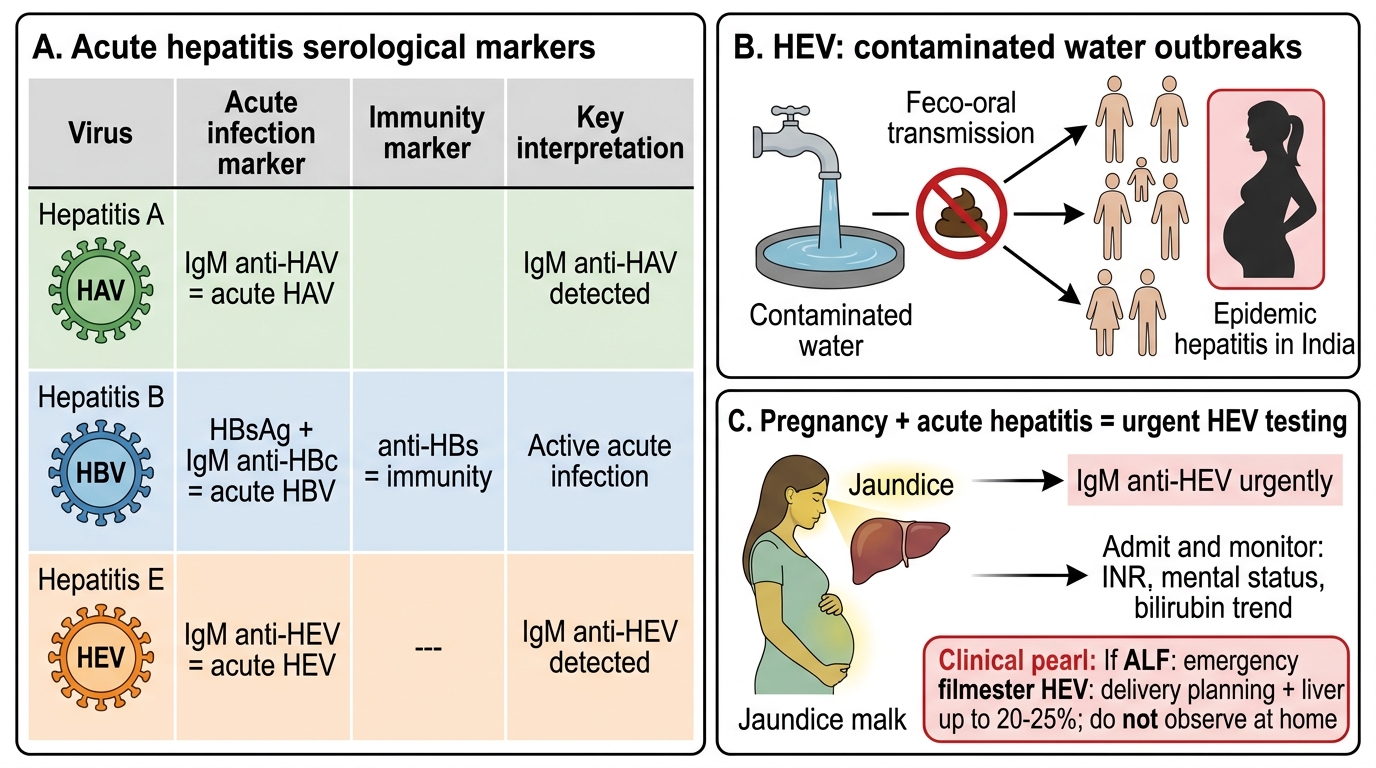
Acute Hepatitis Serology and HEV Pregnancy Warning
CLINICAL PEARL
Hepatitis E in pregnancy carries special danger — and you must warn the family. While Hepatitis E is self-limiting in most children and non-pregnant adults, it causes fulminant hepatic failure in up to 20–25% of pregnant women in the third trimester — this is among the highest case-fatality rates of any common viral infection. In India, HEV is transmitted by contaminated water and is responsible for epidemic hepatitis outbreaks. If you encounter a pregnant woman — or a woman of childbearing age in an outbreak setting — with acute hepatitis, HEV testing (IgM anti-HEV) is urgent, and if positive, she requires immediate hospitalisation, close monitoring for early signs of ALF (INR, mental status, bilirubin trajectory), and planning for possible emergency delivery and liver transplant evaluation if ALF develops. This is one of the few infectious hepatitis scenarios where 'observe at home' is genuinely dangerous.