Page 14 of 42
PE23.5 | Dysentery — SDL Guide
Learning Objectives
- Distinguish dysentery from watery diarrhoea using clinical features
- Identify the commonest causes of dysentery in Indian children including Shigella, Entamoeba histolytica, and EHEC
- Plan appropriate investigations for a child presenting with bloody mucoid diarrhoea
- Prescribe correct antibiotic therapy for bacillary and amoebic dysentery and recognise when antibiotics are contraindicated
- Recognise haemolytic uraemic syndrome (HUS) as a complication of EHEC infection and manage appropriately
INSTRUCTIONS
Dysentery is one of the most common infectious causes of childhood morbidity in India, accounting for significant paediatric admissions and diarrhoeal deaths. Unlike watery diarrhoea, dysentery involves mucosal invasion and carries a risk of systemic complications. The ability to distinguish bacterial from amoebic dysentery and to make the critical EHEC/HUS decision — where antibiotics must be withheld — is a core clinical competency for every paediatric practitioner.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 13 (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Ch 366–368 (textbook)
- WHO Guidelines for the Treatment of Dysentery in Children, 2005 (guideline)
- IAP Guidelines on Management of Acute Diarrhoeal Disease (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is brought to the paediatric OPD with 3 days of diarrhoea that started as watery stools but became frequent, small-volume, and blood-streaked with mucus from day 2. He now passes 10–12 such stools a day with painful straining. He is febrile at 38.8°C, irritable, and has mild periumbilical cramps. His mother reports he attended a birthday party 4 days ago where food was served outdoors. On examination, he is alert, has mildly sunken eyes, and his abdominal exam shows mild diffuse tenderness. You notice he is straining to defaecate even though his rectum is empty. What is driving this clinical picture and what is the most dangerous management mistake you could make in EHEC-associated disease?
WHY THIS MATTERS
Dysentery remains a leading cause of preventable childhood mortality in India, particularly in children under 5 years of age. India contributes disproportionately to the global burden of diarrhoeal disease, and bloody diarrhoea signals mucosal invasion — a qualitatively different and more dangerous process than secretory diarrhoea. Among the bacterial causes, Shigella dysenteriae is the most common pathogen of bloody diarrhoea in Indian children. The condition demands precise clinical reasoning: choosing the wrong antibiotic or — critically — prescribing any antibiotic for EHEC-associated dysentery can precipitate haemolytic uraemic syndrome (HUS), a triad of haemolytic anaemia, thrombocytopaenia, and acute kidney injury that carries significant mortality. Getting this decision right is one of the highest-stakes antibiotic-management choices you will make in paediatric practice.
RECALL
Before proceeding, consolidate your foundation knowledge. Recall the difference between secretory diarrhoea (large-volume, watery, osmotic gradient from enterotoxins, no mucosal damage — as in cholera) and invasive/inflammatory diarrhoea (small-volume, frequent, blood and mucus, mucosal disruption, fever — as in dysentery). Recall the IMNCI diarrhoea classification: no dehydration, some dehydration (sunken eyes, reduced skin turgor, restless/irritable — Plan B ORS), and severe dehydration (lethargic, deeply sunken eyes, no skin turgor, drinking poorly — Plan C IV fluids). Recall that reduced-osmolarity ORS (245 mOsm/L) is the current WHO standard, replacing the older 311 mOsm/L formulation, and zinc supplementation (10 mg/day under 6 months; 20 mg/day for 6 months–5 years for 10–14 days) is recommended for all acute diarrhoea episodes. Recall that Entamoeba histolytica trophozoites are the invasive form and that metronidazole is the principal amoebicidal agent.
Clinical Presentation of Dysentery
Dysentery is defined as diarrhoea in which the stools contain visible blood and mucus, accompanied by painful straining. This pattern reflects mucosal damage and inflammation in the large intestine rather than the osmotic or secretory mechanisms of watery diarrhoea. The clinical picture is characteristically distinct and allows bedside diagnosis even before laboratory investigations return.
Provided image
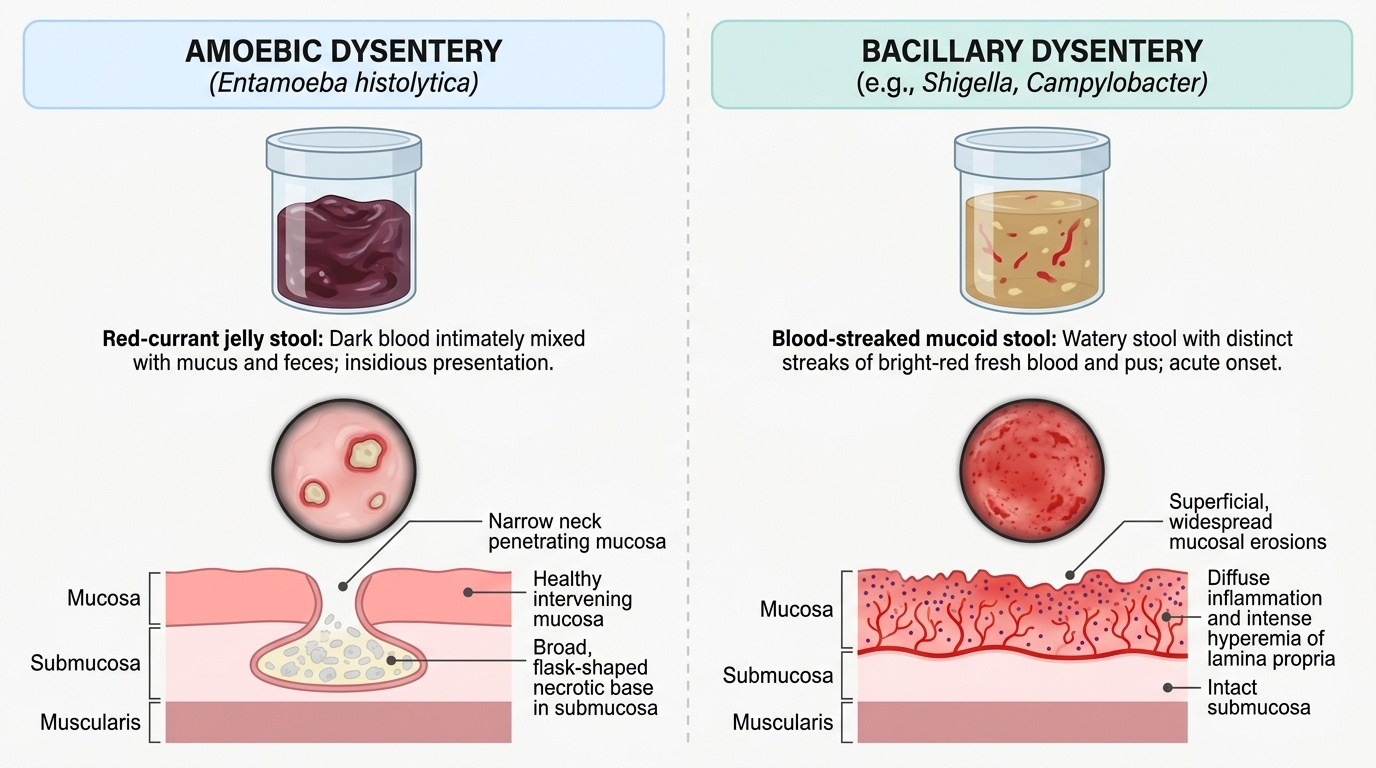
The cardinal features are frequent, small-volume stools containing blood mixed with mucus — classically described as 'red-currant jelly' stools in amoebic disease or as frankly blood-streaked mucoid stools in bacillary disease. Tenesmus — a persistent, painful urge to defaecate despite an empty rectum — is a hallmark and results from rectal mucosal inflammation. Fever is almost invariably present in bacterial dysentery because of mucosal invasion and systemic bacteraemia; it may be absent or low-grade in uncomplicated amoebic dysentery. Children are typically irritable and anorexic; abdominal cramps and diffuse tenderness on palpation are common.
Assess dehydration status carefully using IMNCI criteria: sunken eyes, reduced skin turgor, dry mucous membranes, and altered consciousness are the key signs. In dysentery, dehydration is less severe than in secretory diarrhoea because stool volumes are small, but systemic toxicity and refusal of oral intake can compound the deficit. Check for danger signs of systemic spread: high sustained fever, convulsions, altered sensorium, pallor suggesting haemolysis (suspicious for HUS in epidemic settings), and oliguria or haematuria.
Amoebic dysentery (Entamoeba histolytica) tends to have a more insidious onset, less fever, and characteristic 'flask-shaped' ulcers on proctoscopy. Bacillary dysentery (Shigella, Campylobacter) presents more acutely with higher fever and greater systemic toxicity. EHEC (E. coli O157:H7) classically begins as bloody diarrhoea without fever, followed several days later by pallor, decreased urine output, and petechiae — signalling the onset of HUS.
Pathophysiology and Aetiology
Understanding the mechanism of mucosal invasion explains both the clinical features of dysentery and the rational basis for treatment decisions, including the contraindication of antibiotics in EHEC infection.
Bacillary dysentery is caused primarily by Shigella species, most commonly Shigella dysenteriae in India. Other bacterial causes include enterotoxigenic and enteroinvasive E. coli (ETEC/EIEC), Campylobacter jejuni, and non-typhoidal Salmonella. Enterohaemorrhagic E. coli (EHEC), particularly serotype O157:H7, occupies a special pathophysiological category. The mechanism of mucosal damage differs critically between ordinary invasive bacteria and EHEC.
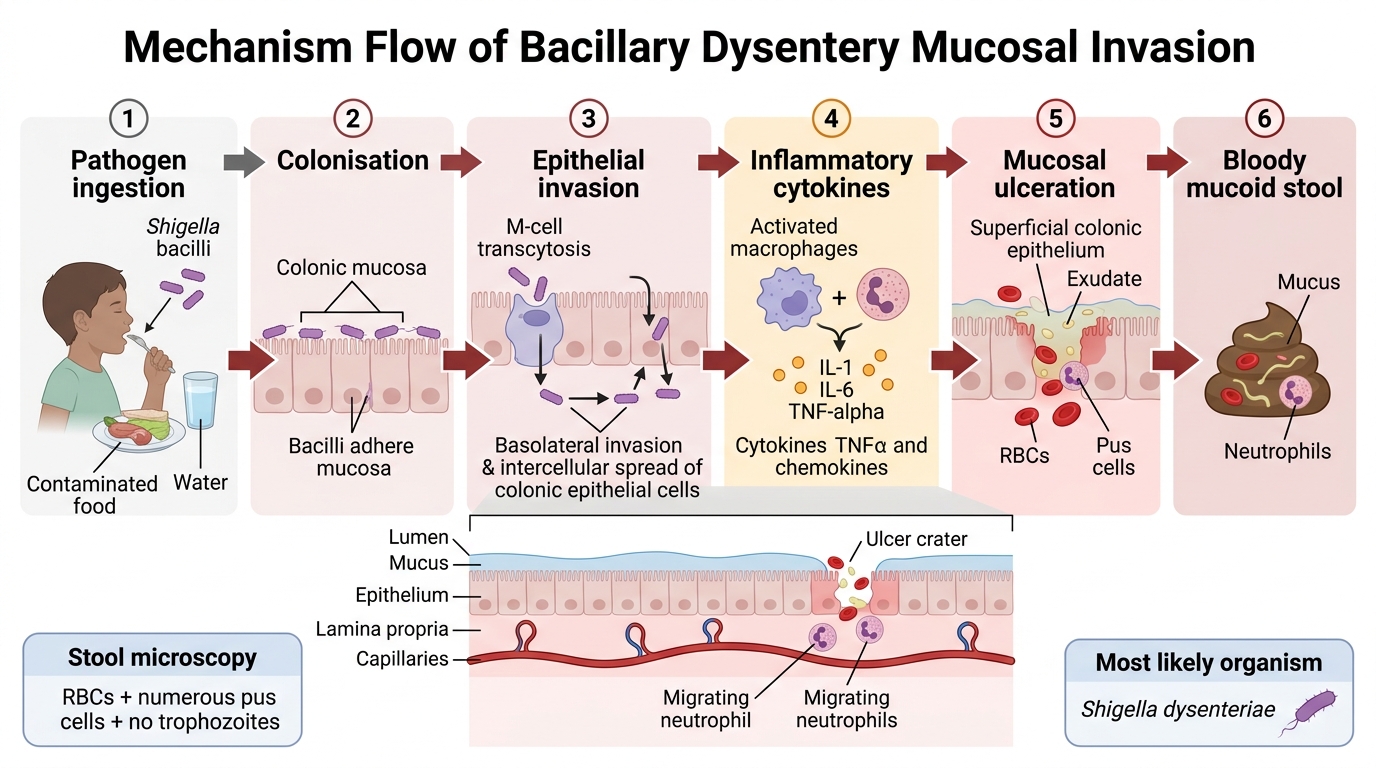
In Shigella infection, organisms are ingested via the faeco-oral route, pass through the small intestine, and penetrate the colonic mucosal epithelium. Inside epithelial cells and macrophages, Shigella multiplies, triggers apoptosis and inflammatory cytokine release (IL-1, IL-6, TNF-α), and spreads cell-to-cell via actin tails. The result is mucosal ulceration, bloody mucoid diarrhoea, and a marked polymorphonuclear infiltrate in the lamina propria. Bacteraemia is less common than the intense local inflammation suggests, but can occur in malnourished or immunocompromised children. The infective dose is very low (as few as 10–200 organisms) — hence easy person-to-person spread.
EHEC (O157:H7) does NOT invade the mucosa. Instead, it adheres to colonic epithelium and releases Shiga toxin (verotoxin), which binds to Gb3 receptors on intestinal and renal glomerular endothelial cells, inhibits protein synthesis, causes endothelial death, and triggers a thrombotic microangiopathy. The kidney's glomerular endothelium is uniquely vulnerable. This Shiga toxin mechanism is why antibiotics are CONTRAINDICATED in suspected EHEC dysentery: bacteriolytic antibiotics (and certain antibiotics like fluoroquinolones) cause a massive release of preformed Shiga toxin from lysed bacteria, dramatically increasing the risk of HUS.
Entamoeba histolytica infects via cyst ingestion; trophozoites excyst in the colon and invade the mucosal epithelium, forming characteristic flask-shaped ulcers that undermine the submucosa. Contact-dependent cytolysis via amoebapore proteins and proteolytic enzymes leads to the necrotic colitis picture.
The epidemiology is shaped by sanitation: Shigella thrives in contaminated water and food in low-resource settings; E. histolytica is endemic in areas without adequate sanitation; EHEC is classically food-borne (undercooked beef, unpasteurised milk, but also raw produce) and may occur in small outbreaks.
Mucosal Invasion Pathway in Bacillary Dysentery
SELF-CHECK
A 3-year-old presents with 2 days of bloody diarrhoea and fever of 39°C. The stool microscopy shows red blood cells, numerous pus cells, and no trophozoites. Which organism is the most likely cause of dysentery in an Indian child?
A. Entamoeba histolytica
B. Shigella dysenteriae
C. Enterohaemorrhagic E. coli O157:H7
D. Vibrio cholerae
Reveal Answer
Answer: B. Shigella dysenteriae
Shigella dysenteriae is the most common cause of bacterial (bacillary) dysentery in India. Shigellosis characteristically shows numerous pus cells (polymorphonuclear leucocytes) and red blood cells on stool microscopy due to mucosal invasion. Entamoeba histolytica is amoebic dysentery with trophozoites and RBCs but few pus cells. EHEC occurs but is far less common in India. Vibrio cholerae causes watery diarrhoea, not dysentery.
Diagnosis and Investigation
The diagnosis of dysentery is primarily clinical — the combination of bloody mucoid stools, fever, tenesmus, and abdominal cramps establishes the diagnosis at the bedside. However, investigations are critical to identify the causative organism, detect complications (especially early HUS in EHEC), and guide antibiotic choice in settings where drug resistance is prevalent. A systematic investigative approach, beginning with stool examination and escalating to systemic markers when complications are suspected, should be applied in every child with bloody diarrhoea. The choice of which investigations to prioritise depends on the clinical context: in a child with typical Shigella presentation (fever, pus cells), stool microscopy and culture suffice; in a child who is afebrile with bloody diarrhoea and then develops pallor, a full blood count with peripheral smear and renal function tests become urgent priorities.
Stool examination is the cornerstone. Fresh stool (collected within 30 minutes) should be examined microscopically for:
- Pus cells (polymorphonuclear leucocytes) — numerous in bacillary dysentery, few or absent in amoebic.
- Red blood cells — present in both.
- Amoebic trophozoites — seen in fresh warm stool in amoebic dysentery; look for trophozoites with ingested red blood cells (hallmark of invasive amoeba, distinguishing from non-pathogenic E. dispar).
- Cysts — E. histolytica cysts with 1–4 nuclei.
Stool culture and sensitivity (on MacConkey agar and selective media) identifies the bacterial organism and guides antibiotic choice — crucial given widespread Shigella resistance to cotrimoxazole and ampicillin. Campylobacter requires microaerophilic culture. Stool for EHEC testing (verotoxin ELISA or PCR) is performed when HUS is suspected.
Complete blood count: leucocytosis with left shift suggests bacterial infection. Anaemia with thrombocytopaenia in a child with bloody diarrhoea should prompt suspicion for HUS (EHEC). If the CBC shows microangiopathic haemolytic anaemia (fragmented RBCs/schistocytes on peripheral smear), elevated creatinine, and thrombocytopaenia — the triad of HUS is established.
Renal function tests (urea, creatinine, electrolytes) and urinalysis (haematuria, proteinuria) are essential when HUS is suspected. Peripheral smear for schistocytes and platelet count are mandatory in any child with bloody diarrhoea who develops pallor or oliguria.
Assessment of dehydration by clinical examination (IMNCI criteria) is equally important — though stool volumes in dysentery are smaller than in cholera-like illness, systemic toxicity and poor oral intake can cause significant dehydration.
| Stool finding | Bacillary dysentery | Amoebic dysentery |
|---|---|---|
| Consistency | Watery + mucus + blood | Semi-formed or mucoid; 'currant jelly' |
| Pus cells | Many (>50/hpf) | Few or absent |
| Red blood cells | Present | Present (ingested by trophozoites) |
| Organisms | Culture positive (Shigella/Campylobacter) | Trophozoites with RBCs |
| Odour | Offensive | Less offensive |
CLINICAL PEARL
EHEC trap — never prescribe antibiotics for bloody diarrhoea without excluding EHEC. The classic presentation of EHEC (O157:H7) is bloody diarrhoea WITHOUT fever — this is the clinical clue. If a child presents with afebrile bloody diarrhoea and there is any suspicion of EHEC (outbreak setting, undercooked meat exposure, or if the child develops pallor/oliguria within days), withhold all antibiotics. Antibiotic-induced lysis of EHEC releases a surge of Shiga toxin, increasing HUS risk 2–10 fold. Additionally, fluoroquinolones induce the phage-encoded Stx gene, further amplifying toxin production. For uncomplicated Shigella dysentery, ciprofloxacin (15 mg/kg/day in two divided doses for 3 days) is the first-line treatment in India because of widespread cotrimoxazole and ampicillin resistance. Ceftriaxone (50–100 mg/kg/day IV) is used for severe or complicated cases requiring parenteral therapy.