Page 36 of 42
PE23.17-21 | Gastrointestinal Clinical Assessment — SDL Guide (Part 2)
Interpretation of LFTs, Viral Markers, and USG Reports
Interpreting the results of liver investigations requires a pattern-recognition approach that integrates multiple tests simultaneously rather than reading each value in isolation. The single most important first step is to determine whether the pattern of LFT derangement is hepatocellular (predominantly elevated transaminases — ALT and AST — reflecting hepatocyte injury) or cholestatic (predominantly elevated alkaline phosphatase and GGT — reflecting impaired bile flow). This distinction immediately directs the aetiological differential and the next investigation step. Mixed patterns occur in advanced disease where both hepatocyte injury and biliary obstruction coexist. Alongside LFTs, the viral serology markers (particularly the full hepatitis B panel) are commonly misread by students who memorise individual markers without understanding their combinations; this section provides a systematic approach to reading the HBV serology pattern.
Provided image
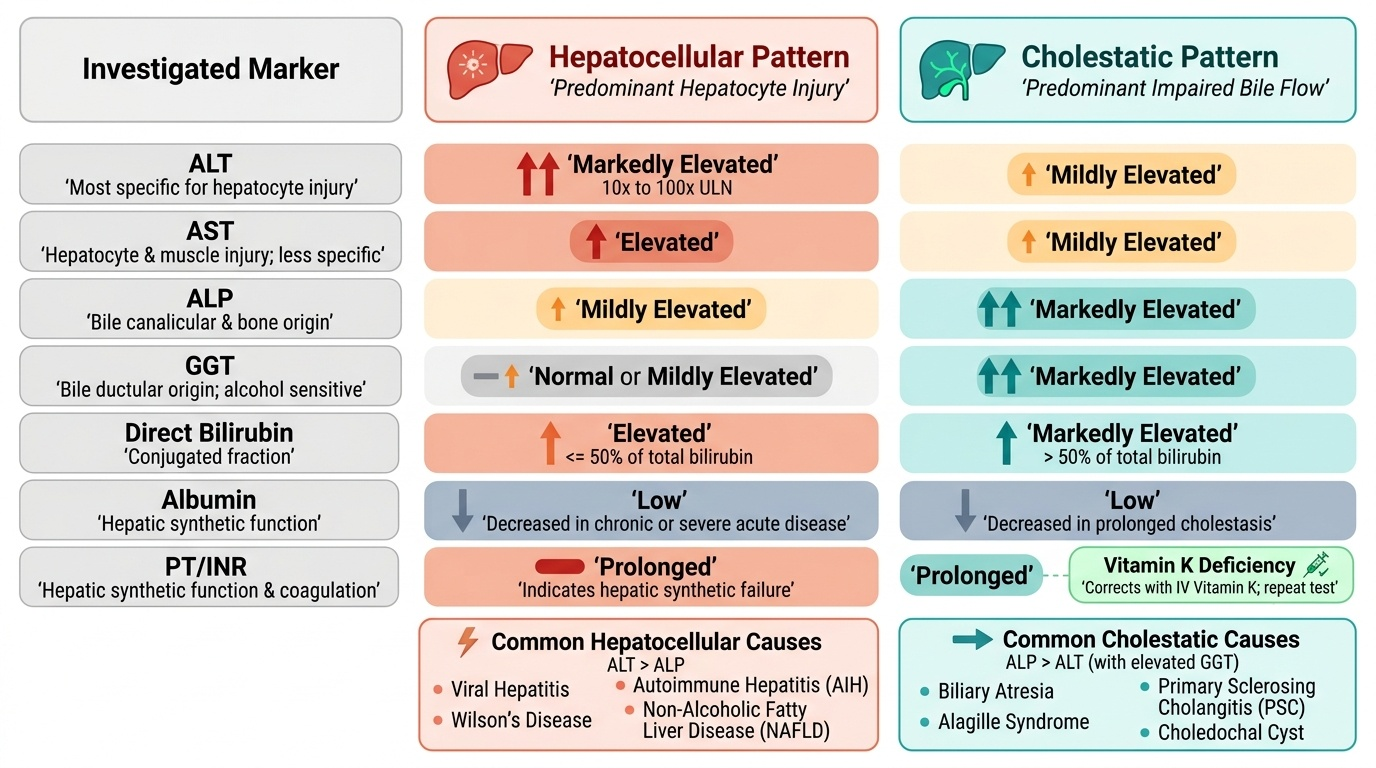
LFT pattern interpretation:
| LFT | What it measures | Hepatocellular pattern | Cholestatic pattern |
|---|---|---|---|
| ALT (alanine aminotransferase) | Hepatocyte injury (most specific) | Markedly elevated (×10–100 ULN) | Mildly elevated |
| AST (aspartate aminotransferase) | Hepatocyte + muscle injury | Elevated (less specific than ALT) | Mildly elevated |
| ALP (alkaline phosphatase) | Bile canalicular/bone | Mildly elevated | Markedly elevated |
| GGT (gamma-glutamyl transferase) | Bile ductular; alcohol | Normal or mildly elevated | Markedly elevated |
| Bilirubin (direct) | Conjugated fraction | Elevated (≤50% in pure hepatocellular) | Markedly elevated (>50%) |
| Albumin | Synthetic function | Low in chronic/severe | Low in prolonged cholestasis |
| PT/INR | Synthetic function | Prolonged | Prolonged (also from Vit K deficiency — correct with Vit K and re-test) |
Key interpretation rules:
1. ALT > ALP = hepatocellular pattern (viral hepatitis, Wilson, AIH, NAFLD)
2. ALP > ALT (especially with elevated GGT) = cholestatic pattern (biliary atresia, PSC, Alagille, choledochal cyst)
3. Low albumin + prolonged INR = hepatic synthetic failure (chronic or severe acute disease)
4. A prolonged INR that corrects with IV Vitamin K suggests Vitamin K deficiency (malabsorption/cholestasis), NOT hepatic synthetic failure; repeat INR after Vitamin K before concluding synthetic failure
Viral markers — interpretation:
Hepatitis B serology panel:
| Clinical state | HBsAg | Anti-HBs | Anti-HBc IgM | Anti-HBc IgG | HBeAg | HBV DNA |
|---|---|---|---|---|---|---|
| Susceptible (unvaccinated) | − | − | − | − | − | − |
| Acute HBV | + | − | + | − | ± | High |
| Past infection (immune) | − | + | − | + | − | − |
| Vaccinated (immune) | − | + | − | − | − | − |
| Chronic HBV (active) | + | − | − | + | + | High |
| Chronic HBV (inactive carrier) | + | − | − | + | − | Low |
Key rules: HBsAg = antigen from the virus surface = infected (acute or chronic); Anti-HBs = antibody to surface antigen = immune (past infection or vaccination); Anti-HBc IgM = acute phase antibody; Anti-HBc IgG = past exposure. Chronic HBV = HBsAg positive for >6 months.
Hepatitis A: Anti-HAV IgM = acute infection; Anti-HAV IgG = past infection or immunity (from vaccine).
Hepatitis E: Anti-HEV IgM = acute infection (confirm with HEV RNA if available).
Abdominal USG interpretation (common GI/hepatobiliary findings):
• Hepatomegaly: Liver measures >13 cm span (age-dependent); echogenicity increased = fatty change (NAFLD, glycogen storage); decreased = acute hepatitis; coarse echotexture = cirrhosis
• Splenomegaly: Spleen >11 cm in school-age; increased in portal hypertension, infection, storage disorders
• Portal vein: Normal diameter <13 mm in children; enlarged = portal hypertension; absent/replaced by collaterals = EHPVO (cavernous transformation)
• Ascites: Anechoic free fluid in peritoneal cavity; most sensitive in Morison's pouch (hepatorenal space)
• Biliary system: Dilated intrahepatic bile ducts (>2 mm) = cholestasis; absent gall bladder + triangular cord sign = biliary atresia
SELF-CHECK
A 9-year-old girl has the following LFT results: ALT 680 U/L (normal <40), AST 520 U/L, ALP 95 U/L (normal 40–130), GGT 42 U/L (normal <35), total bilirubin 6.2 mg/dL (direct 3.8 mg/dL), albumin 3.1 g/dL, INR 1.8. Which pattern does this represent, and what is the most likely class of diagnosis?
A. Cholestatic pattern — most likely biliary atresia or PSC
B. Hepatocellular pattern — most likely viral hepatitis, autoimmune hepatitis, or Wilson disease
C. Mixed pattern suggesting both hepatocellular injury and biliary obstruction equally
D. Normal LFT pattern with incidental hyperbilirubinaemia
Reveal Answer
Answer: B. Hepatocellular pattern — most likely viral hepatitis, autoimmune hepatitis, or Wilson disease
ALT 680 >> ALP 95 = hepatocellular pattern (ALT markedly elevated, ALP barely above normal). The low albumin and elevated INR indicate significant hepatic synthetic compromise. The cholestatic pattern would show ALP and GGT markedly elevated with relatively mild ALT elevation. Hepatocellular causes include acute viral hepatitis (A, B, E), autoimmune hepatitis (check ANA, anti-SMA), and Wilson disease (check ceruloplasmin in this age group). Biliary atresia and PSC cause cholestatic patterns (high ALP/GGT, predominantly direct bilirubinaemia, relatively modest ALT elevation).
Indications for Upper GI Endoscopy
Upper gastrointestinal endoscopy (oesophagogastroduodenoscopy, OGD) is an endoscopic procedure in which a flexible fibreoptic instrument is passed from the mouth through the oesophagus, stomach, and into the duodenum. In children it requires general anaesthesia or deep sedation and is performed by a paediatric gastroenterologist. Understanding the indications — when to request OGD and what clinical question you are asking — is a core competency for the final-year student, who must know not only that endoscopy may be needed, but why (diagnostic versus therapeutic), and what information to provide in the referral to allow the gastroenterologist to prepare appropriately. OGD in children is generally safe, with a low complication rate, but it carries the risks of aspiration, perforation (rare), and sedation-related events — these risks must be balanced against the clinical need. The clinician ordering OGD must ensure that the child is nil by mouth before the procedure (typically 4 hours for clear fluids, 6 hours for solids in scheduled elective OGD).
Diagnostic indications for upper GI endoscopy:
• Haematemesis or malaena — to identify the source of bleeding (oesophageal varices, gastric/duodenal ulcer, Mallory-Weiss tear, haemorrhagic gastritis, Dieulafoy lesion); urgent OGD should be performed within 12–24 hours of haemodynamic stabilisation
• Unexplained iron deficiency anaemia — to look for occult upper GI blood loss (portal hypertensive gastropathy, gastric antral vascular ectasia, ulcers, polyps)
• Dysphagia — oesophageal stricture, eosinophilic oesophagitis, oesophageal web
• Persistent or severe vomiting — upper GI obstruction, pyloric stenosis (in older children / recurrence), superior mesenteric artery syndrome
• Suspected coeliac disease — duodenal biopsy (at least 4 biopsies from different duodenal segments, including the duodenal bulb, to maximise sensitivity for villous atrophy)
• Suspected H. pylori infection — antral biopsy for rapid urease test (CLO test), histology, or culture in complicated peptic ulcer disease
• Suspected portal hypertension — to assess and grade oesophageal varices, detect gastric varices, and assess portal hypertensive gastropathy
• Ingestion of corrosives (acid/alkali) — to assess the extent of oesophageal and gastric mucosal injury (delay 24–48 h from ingestion to allow the acute inflammatory phase to declare itself)
Therapeutic indications for upper GI endoscopy:
• Oesophageal variceal band ligation (EVL) — primary and secondary prophylaxis of variceal haemorrhage; also acute haemostasis during active variceal bleed
• Endoscopic injection sclerotherapy (EIS) — injection of sclerosant into/around oesophageal varices; used when EVL technically difficult
• Foreign body removal — coins, button batteries (urgent — electrolytic tissue injury), food bolus impaction
• Haemostasis — adrenaline injection, electrocautery, or haemostatic clips for bleeding peptic ulcers; adrenaline injection into actively bleeding varices as temporising measure
• Oesophageal dilatation — for strictures (caustic, peptic, post-surgical)
• Placement of enteral feeding tubes — percutaneous endoscopic gastrostomy (PEG) for long-term enteral nutrition
Contraindications to OGD:
• Haemodynamic instability not corrected (relative)
• Suspected perforated viscus
• Uncorrected coagulopathy (INR >2.5 for therapeutic procedures)
• Uncooperative child without adequate sedation/anaesthesia plan
What to include in an OGD referral:
• Age and weight of child (for sedation dosing)
• Indication (diagnostic/therapeutic — be specific)
• Current medications (anticoagulants, proton pump inhibitors)
• Allergy history
• Recent INR (especially for therapeutic procedures)
• Whether an urgent (within 24h) or elective procedure is required
SELF-CHECK
A 10-year-old with known EHPVO develops haematemesis and is resuscitated with IV octreotide and blood transfusion. He is now haemodynamically stable. When should upper GI endoscopy be performed, and what is its therapeutic role in this case?
A. Endoscopy should be performed immediately during active bleeding regardless of haemodynamic status
B. Endoscopy should be performed within 12-24 hours of haemodynamic stabilisation for diagnostic confirmation and therapeutic variceal band ligation
C. Endoscopy is not indicated in EHPVO — management is surgical only
D. Endoscopy should be deferred for 4 weeks until the varices shrink spontaneously
Reveal Answer
Answer: B. Endoscopy should be performed within 12-24 hours of haemodynamic stabilisation for diagnostic confirmation and therapeutic variceal band ligation
In haemodynamically stable variceal haemorrhage, upper GI endoscopy should be performed within 12–24 hours of stabilisation. This timeline balances the risk of re-bleeding (early) against the risk of performing endoscopy in an unstable patient (immediate). The therapeutic role is endoscopic variceal band ligation (EVL) — placing elastic bands at the varix base to strangulate and obliterate it. Endoscopy during active haemorrhage with haemodynamic instability is more hazardous and should wait for stabilisation. Surgical management (Rex shunt) is a planned definitive procedure, not an emergency alternative to endoscopy. Varices do not shrink spontaneously.
Applied Practice: Putting It Together
Translating individual clinical skills into a coherent assessment of a child with GI or liver disease requires a structured presentation and documentation framework. In a clinical examination, a long case on liver disease is typically marked on three dimensions: the quality of the history (did you cover all the aetiological domains?), the accuracy and completeness of the examination (did you correctly detect and characterise organomegaly, ascites, and external markers?), and the quality of your investigation plan and interpretation. In clinical practice, the additional requirement is to communicate your findings clearly to a gastroenterologist or hepatologist — a referral letter that says 'the child has a big liver and yellow eyes' is far less useful than one that specifies the liver edge in centimetres, the character of the organ, the constellation of associated signs, and your preliminary aetiological hypothesis with key positive and negative investigation results.
Structured clinical presentation framework for paediatric GI/liver case:
- Introduce the patient — age, sex, presenting complaint and duration
- History — jaundice (chronology, urine/stool colour, pruritus), GI symptoms (pain, vomiting, bleeding, diarrhoea), growth failure; aetiological clues (perinatal, family, drugs, diet, travel, vaccinations)
- General examination — nutritional status (weight, height, MUAC), pallor, jaundice (degree), external markers (spider angiomata — count, site; palmar erythema; clubbing; caput medusae with flow direction; vitamin deficiency signs)
- Abdominal examination — inspection (shape, scars, veins), percussion (liver span, ascites — shifting dullness result), palpation (liver — size/surface/edge/consistency; spleen — size; ballottement of kidneys)
- Summary and hypothesis — 'This child has features consistent with CLD/portal hypertension/FHF (state which), most likely caused by [aetiology], in the context of [risk factors]'
- Investigation plan — first-tier (LFTs, CBC, coagulation, glucose, USG) + aetiology-specific (ceruloplasmin, autoantibodies, viral markers, A1AT phenotype) + staging (biopsy, elastography)
- Management priorities — immediate (correct hypoglycaemia, treat active bleeding, initiate aetiology-specific therapy) + referral decision (transplant centre if INR >4, Grade III–IV HE, Wilson FHF)
- Endoscopy decision — state the indication (diagnostic/therapeutic), urgency (within 24h/elective), and what you expect to find
Documentation essentials:
• Always state organ size in centimetres below the costal margin, not as 'enlarged' or 'big'
• Always state the percussion result for ascites (shifting dullness positive/negative at which position)
• Always state which specific external markers are present and which are absent (negative findings matter)
• Always include a growth assessment (weight, height, MUAC, WHO chart percentile) in any child with GI/liver disease
Self-Assessment: GI Clinical Assessment
Test your integrated clinical assessment skills with these scenarios.
Scenario 1 (History): Parents of an 8-year-old girl report progressive jaundice, dark urine, pale stools, and severe itching for 3 weeks. The child was born normally; her newborn screening was normal. Her elder sister had 'kidney trouble'. What specific historical features would you probe to distinguish biliary atresia (presenting very late — unlikely), Alagille syndrome, or primary sclerosing cholangitis?
Key answer points: Biliary atresia presents in the neonatal period; presenting at 8 years effectively rules it out. Ask: Eye examination history (posterior embryotoxon = Alagille); cardiac murmurs (peripheral pulmonic stenosis = Alagille); family history of liver disease (Alagille is autosomal dominant); history of inflammatory bowel disease (PSC associated with IBD — check for bloody diarrhoea, urgency, rectal bleeding). Order: MRCP (biliary strictures = PSC), JAG1/NOTCH2 gene testing and eye exam (Alagille), colonoscopy if IBD suspected. Her sister's 'kidney trouble' could be renal cysts associated with Alagille (JAG1 mutation can cause renal structural anomalies).
Scenario 2 (Examination + Investigation): You examine a 15-year-old male. Liver 5 cm below costal margin (firm, nodular edge), spleen 9 cm below left costal margin. Shifting dullness positive. Spider angiomata: 8 on chest. Palmar erythema present. LFTs: ALT 95 U/L, ALP 42 U/L (low!), bilirubin 4.2 mg/dL, INR 2.1, albumin 2.8 g/dL. Interpret the LFT pattern and state the single most important diagnostic test.
Key answer points: Low ALP in the context of active liver disease is the key clue → Wilson disease. ALT > ALP (hepatocellular pattern but ALP paradoxically low from copper inhibition). CLD with portal hypertension (spider angiomata >5, splenomegaly, ascites, firm nodular liver). Most important single test: serum ceruloplasmin + 24-h urinary copper. If Wilson confirmed: penicillamine/trientine + zinc; liver transplant evaluation (cirrhosis likely decompensated).
Scenario 3 (OGD decision): A 12-year-old with cirrhosis secondary to autoimmune hepatitis is found to have Grade III oesophageal varices on elective endoscopy (no history of variceal bleed). His INR is 1.6. Should endoscopic therapy be offered, and if so, what type and urgency?
Key answer points: Yes — Grade III oesophageal varices in a child with cirrhosis warrant primary prophylaxis (before the first bleed). Treatment: endoscopic variceal band ligation (EVL), elective (not urgent), performed in a planned programme of 2–4 weekly sessions until variceal eradication. Propranolol can be added as adjunct. INR 1.6 is acceptable for therapeutic endoscopy (threshold for concern is >2.5). Explain to parents that EVL reduces the risk of a first variceal bleed, which in cirrhotic liver disease is associated with significant mortality.