Page 2 of 42
PE23.1 | Vomiting — SDL Guide (Part 2)
Management of Vomiting in Children
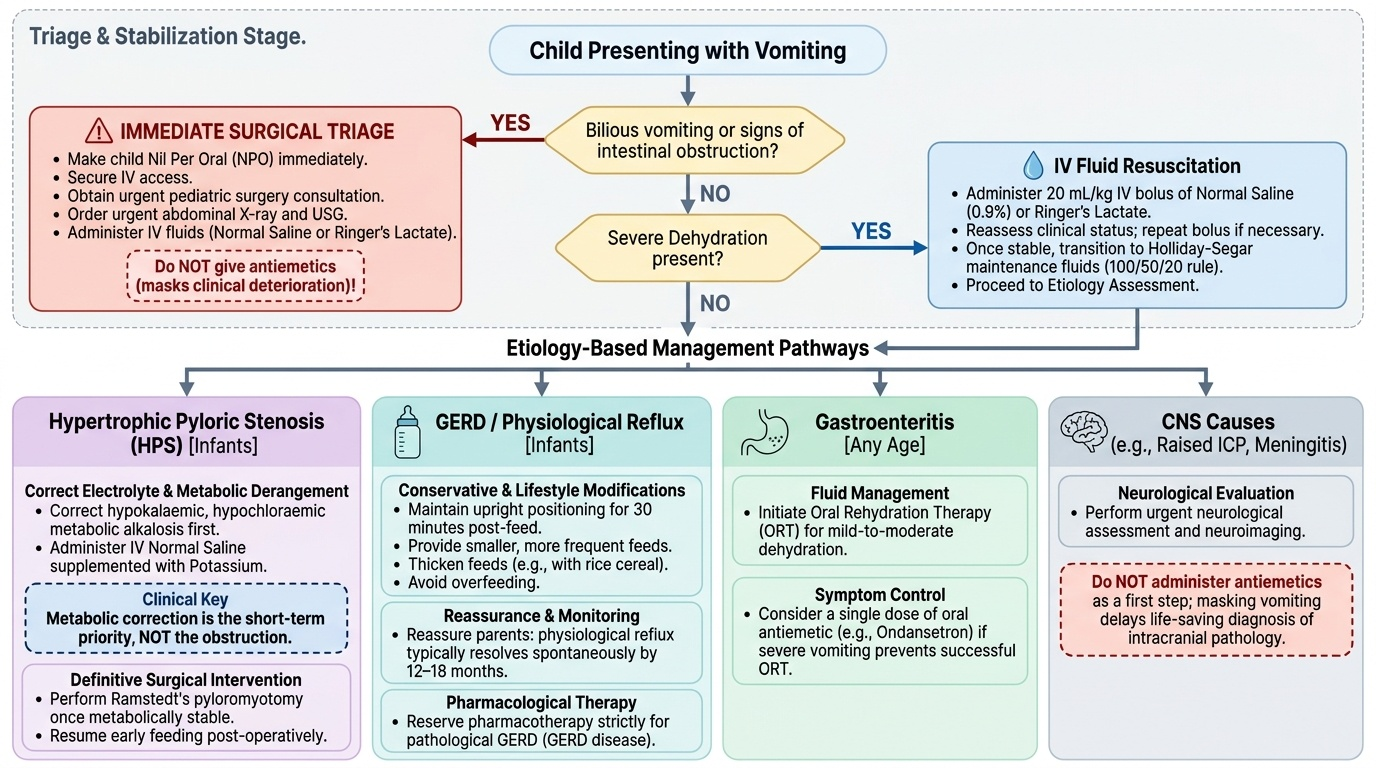
Management of vomiting must be directed at the underlying cause. The immediate priority, however, is to identify and stabilise any child with a surgical emergency or severe dehydration before pursuing definitive treatment. A structured approach is essential: the clinical assessment already performed guides whether the first step is calling the surgeon, resuscitating with IV fluids, or simply beginning oral rehydration therapy. No antiemetic should ever be given as a first step without establishing the diagnosis, because masking vomiting in a child with intestinal obstruction or raised intracranial pressure delays life-saving intervention. The management pathways described below are condition-specific and must be applied only after the cause is identified or at least the surgical emergency is excluded.
Provided image
Immediate approach — triage and stabilise:
1. Bilious vomiting or clinical signs of intestinal obstruction: Make the child nil per oral immediately, secure IV access, obtain urgent surgical consultation, order X-ray and USG. Administer IV fluids (normal saline or Ringer's lactate for dehydration correction). Do NOT give antiemetics as these mask deterioration.
2. Severe dehydration (any cause): IV fluid resuscitation — 20 mL/kg IV bolus of normal saline (0.9%) or Ringer's lactate, reassess, repeat if needed. Transition to Holliday-Segar maintenance fluids once stabilised (100 mL/kg/day for first 10 kg, 50 mL/kg/day for next 10 kg, 20 mL/kg/day for each kg thereafter).
Hypertrophic Pyloric Stenosis (HPS):
- Medical emergency in the SHORT TERM is the metabolic derangement, NOT the obstruction. First correct electrolyte imbalance (hypokalaemic, hypochloraemic metabolic alkalosis) with IV normal saline and potassium supplementation.
- Once metabolically stable, definitive treatment is Ramstedt's pyloromyotomy (surgical division of the hypertrophied pyloric muscle without entering the mucosa). This is curative. Early resumption of feeds post-operatively.
Gastro-oesophageal Reflux (GERD) in infancy:
- Lifestyle modifications first: Upright positioning for 30 minutes post-feed; smaller, more frequent feeds; thickened feeds (rice cereal); avoidance of overfeeding. Reassure parents that most physiological regurgitation resolves spontaneously by 12–18 months.
- Pharmacological: Reserved for GERD disease (pathological — with oesophagitis, poor weight gain, aspiration). H2 blockers (ranitidine) or proton pump inhibitors (omeprazole) as per ESPGHAN guidelines; avoid unnecessary PPI use in uncomplicated regurgitation.
Acute Gastroenteritis with vomiting:
- Oral Rehydration Therapy (ORT) with reduced-osmolarity ORS (osmolarity 245 mOsm/L) is first-line even in the presence of vomiting — give small, frequent sips (5 mL every 1-2 minutes). WHO recommendation.
- Antiemetics: Ondansetron (0.15 mg/kg/dose oral) has a strong evidence base for reducing vomiting and improving oral fluid tolerance in acute gastroenteritis in children ≥6 months. Use a single dose; avoid in prolonged QT. Metoclopramide and promethazine are generally avoided in children due to extrapyramidal side effects.
- NOT indicated: Antiemetics as monotherapy without assessing dehydration; antidiarrhoeals (loperamide is contraindicated in children <2 years).
Increased Intracranial Pressure:
- Head elevation 30°, IV mannitol if herniation threatened, urgent CT head, neurosurgical consultation. Vomiting is a symptom — treating the vomiting alone is dangerous.
Cyclic Vomiting Syndrome:
- Acute phase: IV fluids, antiemetics (ondansetron, lorazepam for intractable episodes), dark quiet room, sumatriptan in migraine-associated CVS
- Prophylaxis: Cyproheptadine (young children), propranolol, amitriptyline, coenzyme Q10 and L-carnitine (metabolic CVS variants)
SELF-CHECK
A 6-week-old male infant with 2-week history of progressively worsening non-bilious projectile vomiting is brought to the casualty. He appears lethargic and dehydrated. Arterial blood gas shows pH 7.55, bicarbonate 34 mEq/L. Serum electrolytes: Na 138, K 2.9, Cl 88 mEq/L. What is the immediate management priority BEFORE surgery?
A. Emergency Ramstedt's pyloromyotomy
B. Insertion of nasogastric tube and gastric lavage
C. Correction of metabolic alkalosis with IV normal saline and potassium supplementation
D. Oral rehydration with reduced-osmolarity ORS
Reveal Answer
Answer: C. Correction of metabolic alkalosis with IV normal saline and potassium supplementation
In hypertrophic pyloric stenosis, the metabolic derangement (hypokalaemic, hypochloraemic metabolic alkalosis from prolonged HCl loss in vomitus) is the immediate life threat, not the pyloric obstruction itself. Surgery (Ramstedt's pyloromyotomy) is curative but must be deferred until the metabolic alkalosis is corrected — anaesthesia with uncorrected alkalosis is dangerous (reduced respiratory drive, arrhythmias). IV normal saline corrects the chloride deficit and fluid loss; potassium supplementation is added once urine output is confirmed. Only after normalisation of serum electrolytes and pH is the child taken for surgery.
Self-Assessment: Clinical Scenarios
The following scenarios test your ability to apply the clinical approach to vomiting in children. Work through each case before reading the discussion.
Scenario 1: A 2-day-old neonate is noted to be vomiting green fluid. He was born at term by normal vaginal delivery. He has not yet passed meconium. Examination reveals mild abdominal distension. A plain X-ray shows a 'double-bubble' sign with no gas distal to the duodenum.
Discussion: Bilious vomiting in a neonate = surgical emergency. The double-bubble sign (distended stomach + distended proximal duodenum with no distal gas) is diagnostic of duodenal atresia — a complete obstruction of the duodenum, commonly associated with Down's syndrome (trisomy 21; 30% of cases). Management: IV access, nil orally, nasogastric decompression, correction of electrolytes, and urgent paediatric surgical repair.
Scenario 2: A 14-month-old male presents with sudden onset of severe, colicky crying episodes, each lasting a few minutes and recurring every 15-20 minutes. Between episodes he appears pale and quiet. One episode of vomiting. Examination reveals a sausage-shaped mass in the right side of the abdomen.
Discussion: Classic intussusception — ileocolic telescoping, peak age 6–18 months. The clinical triad is paroxysmal colicky pain, vomiting, and rectal bleeding (currant-jelly stool appears later). The sausage-shaped mass moves toward the umbilicus. Management: Ultrasound confirms (target sign); pneumatic or hydrostatic air enema reduction under radiological guidance is curative in 75-90% of cases; surgical reduction for failed enema or peritonitis.
Scenario 3: A 10-year-old girl presents with a 3-day history of morning vomiting, diffuse headache, and one episode of blurred vision. Her mother says the vomiting occurs before she gets out of bed. On examination the optic discs appear blurred with loss of the disc margin.
Discussion: Morning vomiting with headache and papilloedema is raised intracranial pressure until proven otherwise. Urgent CT head is indicated. Do NOT give antiemetics without first identifying the cause.
SELF-CHECK
Which statement about vomiting in children is CORRECT?
A. Regurgitation and vomiting are synonymous terms in clinical practice
B. Bilious (green) vomiting in a neonate requires urgent surgical evaluation
C. Ondansetron is contraindicated in children with acute gastroenteritis
D. In hypertrophic pyloric stenosis, bilious vomiting is the characteristic finding
Reveal Answer
Answer: B. Bilious (green) vomiting in a neonate requires urgent surgical evaluation
Bilious vomiting (green or yellow-green) in a neonate or infant requires urgent surgical evaluation as it may indicate intestinal obstruction, malrotation with volvulus, atresia, or Hirschsprung's disease. Option A is incorrect — regurgitation is effortless and passive (typical physiological GERD), while vomiting involves active muscular effort. Option C is incorrect — ondansetron has good evidence for reducing vomiting in acute gastroenteritis and improving oral rehydration success. Option D is incorrect — hypertrophic pyloric stenosis produces NON-bilious projectile vomiting (only gastric contents proximal to the obstruction are expelled; bile enters below the pylorus).