Page 2 of 31
PE24.{1,21} | Cardiorespiratory Arrest — SDL Guide (Part 2)
Advanced Life Support and Rhythm-Directed Therapy
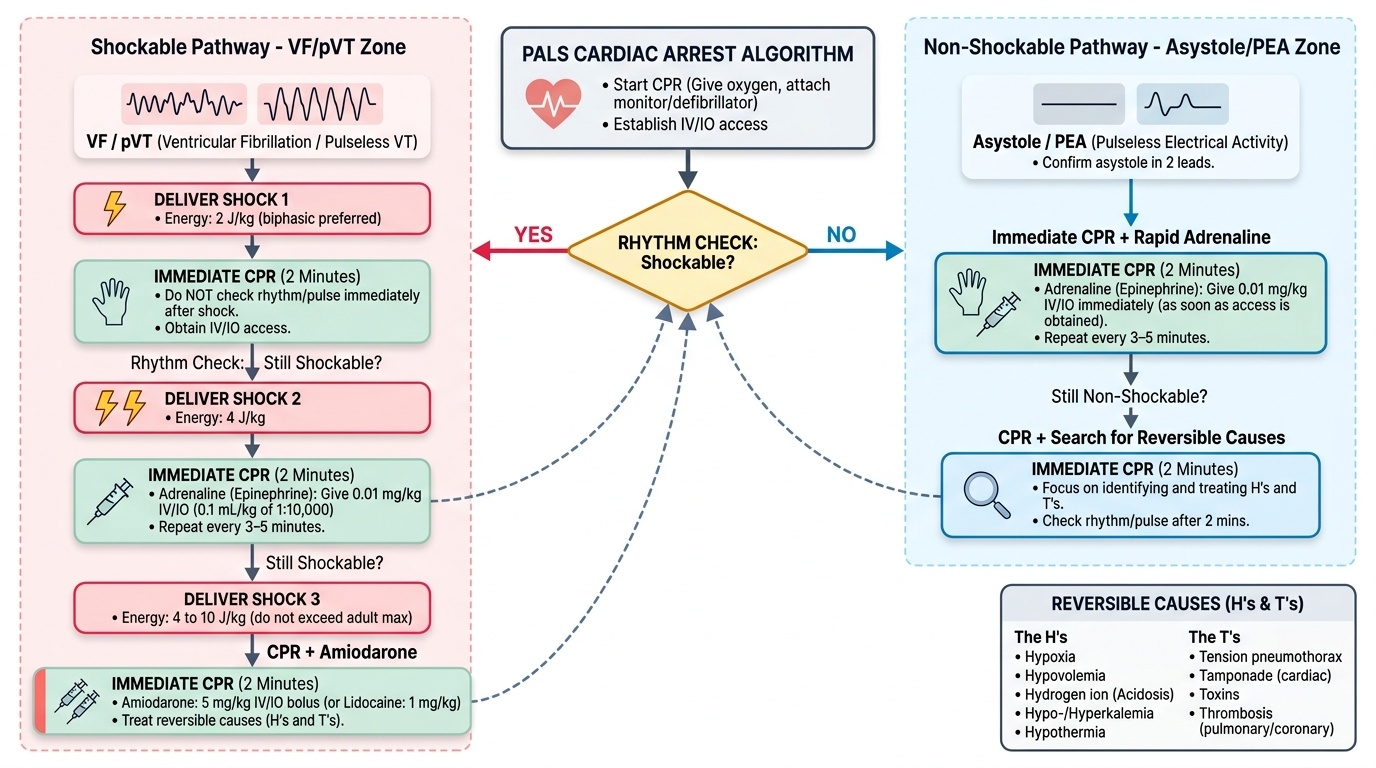
Once BLS is underway, advanced life support (ALS) introduces rhythm analysis, vascular access, and pharmacotherapy. The key decision point is whether the cardiac arrest rhythm is shockable or non-shockable, as this determines whether defibrillation is indicated.
Provided image
Shockable rhythms: Ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT) are the only cardiac arrest rhythms for which defibrillation is indicated. These rhythms are less common in children (occurring in ~10-20% of paediatric arrests) but are more likely in congenital heart disease, electrolyte disturbances, and commotio cordis. On ECG, VF shows chaotic undulations with no discernible P-QRS-T complexes; pVT shows a rapid, wide-complex, monomorphic or polymorphic tachycardia without a palpable pulse.
Non-shockable rhythms: Asystole (flat line on ECG — confirm in two leads, ensure electrode contact before calling asystole) and pulseless electrical activity (PEA) (organised ECG rhythm without a palpable pulse) account for the majority of paediatric arrests. Asystole and PEA are not treatable with defibrillation; management focuses on CPR + adrenaline + identifying reversible causes.
Defibrillation energy dose for VF/pVT:
• Initial shock: 2 J/kg (biphasic preferred; monophasic acceptable)
• Second and subsequent shocks: 4 J/kg (escalate up to a maximum of 10 J/kg or the adult maximum dose)
• After each shock, immediately resume CPR — do NOT pause to check rhythm/pulse after each shock; do so after 2 minutes of CPR
Drug therapy (given IV or IO — intraosseous is equally effective if IV access is unavailable):
• Adrenaline (epinephrine): 0.01 mg/kg IV/IO (= 0.1 mL/kg of 1:10,000 solution); give every 3–5 minutes during CPR; the first dose for non-shockable rhythms is given as soon as IV/IO access is obtained; for VF/pVT give after the second shock
• Amiodarone for shock-refractory VF/pVT: 5 mg/kg IV/IO bolus (can repeat up to two additional doses); alternative: lidocaine 1 mg/kg IV/IO if amiodarone unavailable
• Calcium gluconate: only for hypocalcaemia or hyperkalaemia-related arrest; not routine
• Sodium bicarbonate: only for known metabolic acidosis, hyperkalaemia, tricyclic antidepressant overdose; not routine
The H's and T's — reversible causes to search for during CPR:
| H's | T's |
|---|---|
| Hypoxia | Tension pneumothorax |
| Hypovolaemia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins / drugs |
| Hypo/hyperkalaemia | Thrombosis (pulmonary/coronary) |
| Hypoglycaemia | Trauma |
| Hypothermia |
Vascular access hierarchy: peripheral IV first (antecubital/dorsal foot); if not achieved within 90 seconds or after two attempts → IO access (proximal tibia most common site in children); central venous access is a secondary option.
CLINICAL PEARL
Paediatric arrest is almost always preventable. The child who arrests on the ward nearly always showed premonitory signs hours earlier — tachycardia, tachypnoea, poor perfusion, altered consciousness. Recognising the 'peri-arrest' state and escalating management before arrest occurs is more valuable than any resuscitation skill. Use the 'triangle of assessment' (appearance, work of breathing, circulation to skin) as a 30-second bedside screener on every sick child — it is faster than any vital-sign score.
For manikin practice: the commonest correctable error in student BLS is insufficient compression depth. Medical students compress to ~25-30% of the mannequin's AP diameter instead of one-third. Use the visual landmark of the heel of your hand sinking visibly one-third into the mannequin's chest, and count rhythm aloud ('one-and-two-and-three-and...') to pace 100-120/min.
Post-Resuscitation Care and Prognostication
Return of spontaneous circulation (ROSC) is signalled by a palpable pulse, a rise in end-tidal CO₂ on capnography (usually to >35-40 mmHg), a sudden improvement in pulse oximetry tracing, or the reappearance of a rhythmic waveform on arterial line monitoring. ROSC is the beginning, not the end, of resuscitation. The post-cardiac arrest syndrome is a complex, multi-organ pathophysiological state that follows successful resuscitation and comprises four inter-related components: myocardial stunning and dysfunction, systemic ischaemia-reperfusion injury affecting every organ, hypoxic-ischaemic brain injury, and persistence of the underlying precipitating cause. Failure to address each of these simultaneously is a leading cause of death in the hours to days following ROSC. In children, post-arrest brain injury is the primary determinant of long-term neurological outcome, and every post-resuscitation management decision should be made with neuroprotection as a co-equal goal alongside haemodynamic stabilisation. Children who are conscious and interactive immediately after ROSC have a dramatically better prognosis than those who remain comatose; for comatose children, a structured bundle of post-resuscitation care has been shown to improve survival with favourable neurological outcomes.
Post-ROSC management priorities:
- Airway and ventilation: secure the airway if not already done (endotracheal intubation preferred in post-arrest children). Titrate oxygen to SpO₂ 94–99% — avoid both hyperoxia (which worsens cerebral reperfusion injury) and hypoxia. Target PaCO₂ 35–45 mmHg (avoid hyperventilation — cerebral vasoconstriction worsens outcome).
- Haemodynamic support: target a mean arterial pressure at or above the 5th percentile for age. Correct hypovolaemia with isotonic crystalloid in boluses of 10–20 mL/kg; use vasoactive agents (dopamine, adrenaline, noradrenaline) for cardiogenic or vasodilatory post-arrest haemodynamics. Avoid and treat hypotension aggressively — systolic BP <5th percentile for age is independently associated with poor neurological outcome.
- Targeted temperature management (TTM): for comatose post-arrest children who remain unresponsive after ROSC, TTM at 32–36°C (prevention of fever) for 48–72 hours has been applied per PALS recommendations; avoid active fever (≥38°C). The THAPCA trial in children did not show a difference between 33°C and 36°C, but preventing fever is standard.
- Glucose: treat hypoglycaemia (blood glucose <2.6 mmol/L / <47 mg/dL) promptly with IV glucose; avoid hyperglycaemia (>10 mmol/L) which worsens neurological outcome.
- Neurological monitoring: pupils, GCS/modified GCS, EEG for subclinical seizures, brain MRI (diffusion-weighted) at 24–72 h for prognostication.
- Treat the underlying cause that precipitated the arrest (e.g., antibiotic therapy for septic shock, drainage of tension pneumothorax, antidote for toxin).
Prognostication after paediatric cardiac arrest is complex and should not be made acutely. Favourable factors include witnessed in-hospital arrest, short no-flow time, shockable initial rhythm, and rapid ROSC. Unfavourable factors include out-of-hospital arrest, prolonged downtime (>30 min CPR without ROSC), asphyxial aetiology, absent brainstem reflexes at 24–72 h. Involvement of a paediatric intensivist and neurologist is essential before any decision regarding withdrawal of care.
SELF-CHECK
A child with VF-arrest achieves ROSC after 15 minutes of CPR. SpO₂ is now 100% on FiO₂ 1.0. Blood glucose is 3.1 mmol/L. Which of the following immediate post-ROSC actions is MOST appropriate?
A. Maintain FiO₂ 1.0 to ensure maximum oxygenation
B. Titrate FiO₂ to target SpO₂ 94-99% and monitor blood glucose closely
C. Begin active cooling to 33°C immediately without further assessment
D. Start sodium bicarbonate infusion for presumed metabolic acidosis
Reveal Answer
Answer: B. Titrate FiO₂ to target SpO₂ 94-99% and monitor blood glucose closely
After ROSC, hyperoxia (SpO₂ 100% on FiO₂ 1.0) should be corrected by titrating oxygen to SpO₂ 94–99%; excess oxygen worsens cerebral reperfusion injury. Blood glucose of 3.1 mmol/L is normal (normal post-arrest range 3.9–10 mmol/L) and requires monitoring but not immediate intervention. Routine sodium bicarbonate is not recommended (only for specific indications). TTM at 32–36°C may be indicated in comatose children but is not the first priority over airway/oxygenation management.
Simulation Practice: BLS on a Paediatric Manikin
The transition from knowledge to skill in cardiorespiratory resuscitation cannot occur through reading alone — it requires deliberate practice on a manikin under direct observation and structured feedback. Research in medical education consistently shows that psychomotor skills such as chest compressions deteriorate rapidly without regular practice, and that even a single supervised manikin session significantly improves both compression depth and rate accuracy. The goal of this simulation session is not just to 'go through the motions' but to achieve automaticity: the BLS sequence should become a procedural memory that can be executed under the cognitive and emotional stress of a real arrest. During manikin practice, a deliberate focus on the performance elements that most commonly fail — compression depth, recoil, and the compression-to-ventilation ratio — will have the greatest impact on your readiness for clinical encounters. Ask a peer or facilitator to observe and provide real-time corrective feedback; self-assessment alone is insufficient because compressors systematically overestimate their compression depth when not monitored.
Setup and scenario: Use a paediatric BLS manikin (age-matched if possible — infant or child manikin). A facilitator or peer acts as the second rescuer and monitors your performance against the checklist below.
BLS performance standards (per PALS):
| Element | Acceptable performance |
|---|---|
| Time to first compression | Within 10 seconds of confirming arrest |
| Compression rate | 100–120/min (paced by metronome or count) |
| Compression depth (child manikin) | Visibly ≥one-third AP diameter; ~5 cm |
| Full recoil | Hands fully lift; no leaning on chest |
| Compression interruptions | <10 seconds per interruption |
| Airway opening technique | Head-tilt chin-lift correctly performed |
| Mask seal (BVM) | No visible air leak at mask edges |
| Ventilation volume | Chest visibly rises with each breath |
| C:V ratio (2-rescuer child) | 15 compressions then 2 breaths |
| Team communication | Verbally confirms role swap, counts aloud |
Common errors to self-monitor:
• Stopping compressions to talk or check monitors — maintain uninterrupted CPR
• Inadequate depth — students frequently compress only 2–3 cm; use the one-third visual landmark
• Hyperventilating — two rescue breaths per cycle, 1 second each; excessive ventilation causes gastric inflation and reduces cardiac output by raising intrathoracic pressure
• Poor mask seal — use E-C grip: three fingers (ring, middle, index) lift the jaw (E), thumb and index form a C-clamp over the mask; a leak wastes every breath
• Forgetting to call for help / activate the emergency system — this is the first step, not something done after compressions are already underway
Role rotation: in a two-person team, swap the compressor role every 2 minutes (after each rhythm check) to prevent fatigue-related decline in compression quality.
Debrief after the simulation: reflect on which element was hardest to perform simultaneously — maintaining rate AND depth AND full recoil is cognitively demanding at first; deliberate practice ingrains these as automatic motor programs.
Self-Assessment: Cardiorespiratory Arrest
Self-directed learning in emergency medicine requires not just passive recall but the ability to apply knowledge rapidly under simulated examination conditions. The questions below cover the full scope of this module — recognition criteria, BLS technique, rhythm-directed therapy, drug dosing, and post-ROSC management. Work through each question independently before checking the answers, and if you find yourself uncertain on any item, re-read the relevant section rather than simply memorising the answer. Pay particular attention to numeric precision (compression depth, defibrillation energy dose, adrenaline dose in mg/kg) because these are common MBBS examination and OSCE assessment points where partial knowledge leads to errors. The dose-calculation questions (questions 3 and 5) require you to show your working — practise writing out mg/kg × weight = dose and then convert to volume using the stated concentration. This habit prevents calculation errors in real clinical settings where speed and accuracy are simultaneously demanded.
- A 6-month-old infant is pulseless. You are the only rescuer. Which compression technique do you use and what is the compression-to-ventilation ratio?
- On the cardiac monitor, a child in cardiac arrest shows a chaotic, irregular waveform with no discernible QRS complexes. What rhythm is this? What is the first treatment after identifying it?
- What is the correct adrenaline dose for a 15 kg child in cardiac arrest? What concentration should you use?
- You have been performing CPR for 2 minutes on a child with PEA. The child does not have ROSC. Name three reversible H's and two reversible T's that you should immediately consider.
- After ROSC, the child's SpO₂ is 98% on 2 L/min nasal cannula and blood glucose is 1.8 mmol/L. What is the most urgent intervention?
Answers (for self-check):
1. 2-finger technique (single rescuer); ratio 30:2
2. Ventricular fibrillation (VF); defibrillate at 2 J/kg immediately, then resume CPR
3. 0.01 mg/kg × 15 kg = 0.15 mg; use 1:10,000 solution (0.1 mg/mL), give 1.5 mL IV/IO
4. Any three H's (hypoxia, hypovolaemia, hypoglycaemia, hypothermia, hyperkalaemia, acidosis) and two T's (tension pneumothorax, tamponade, toxins, thrombosis)
5. Treat hypoglycaemia promptly with IV dextrose (blood glucose 1.8 mmol/L is below the 2.6 mmol/L threshold)