Page 21 of 31
PE24.17-20 | Emergency Thermal Care — SDL Guide
Learning Objectives
- Define hypothermia and describe the clinical features, complications, and management of hypothermia in children
- Describe the advantages and correct method of Kangaroo Mother Care (KMC) as a skin-to-skin warming technique
- Describe environmental measures to maintain normal body temperature in neonates and young children
- Assess a child for hypothermia using correct thermometry technique and initiate temperature maintenance
INSTRUCTIONS
Temperature regulation is one of the most basic survival functions, and its failure — particularly hypothermia in neonates — is a leading contributor to neonatal mortality in India. A clinician who recognises hypothermia early, applies the WHO warm chain principles, correctly positions a baby for Kangaroo Mother Care, and controls the thermal environment in the ward is directly preventing a major category of preventable newborn death. This module covers both hypothermia and hyperthermia as clinical emergencies, with emphasis on recognition, prevention, and management using evidence-based techniques.
References
- Ghai Essential Pediatrics, 9th edition, Ch 8 (Care of the Newborn) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 113 (Thermoregulation in the Newborn) (textbook)
- WHO Thermal Protection of the Newborn: A Practical Guide, 1997 (Warm Chain) (guideline)
- IAP Guidelines on Kangaroo Mother Care, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 36-hour-old neonate delivered at a district hospital is brought to you by the nurse: 'The baby is not feeding well and looks blue around the lips.' You check the axillary temperature: 35.4°C. The baby was wrapped in a thin cloth and the delivery room window was open. What is your immediate diagnosis, and what are your first three actions?
WHY THIS MATTERS
Hypothermia is a major contributor to neonatal mortality in India — a country where a significant proportion of deliveries occur in homes or small facilities without radiant warmers. Even hospital-born neonates frequently become hypothermic in the immediate post-delivery period if the warm chain is interrupted: wet skin exposed to a cool room, delayed drying, or early separation from the mother. The WHO estimates that hypothermia contributes to or causes death in a substantial fraction of the approximately 250,000 neonatal deaths occurring annually in India. The warm chain and Kangaroo Mother Care are two evidence-based, low-cost interventions that directly address this burden. On the other end of the temperature spectrum, hyperthermia from fever and heat stroke are both paediatric emergencies that require recognition and rapid cooling to prevent neurological damage. Temperature management — both preventing cold and treating heat excess — is therefore a fundamental bedside skill for every clinician caring for children in India.
RECALL
Recall from your physiology studies:
• Thermoregulatory centre: the hypothalamus integrates afferent temperature signals from skin and core receptors, and coordinates effector responses: peripheral vasoconstriction (conserves heat), shivering thermogenesis (generates heat in older children and adults), and sweating/vasodilation (dissipates heat).
• Brown adipose tissue (BAT): neonates lack the muscle mass to shiver effectively. Their primary heat-generation mechanism is non-shivering thermogenesis via BAT, located in the neck, axillae, mediastinum, and perirenal region. BAT metabolism is stimulated by noradrenaline and generates heat by uncoupling oxidative phosphorylation (via uncoupling protein-1/thermogenin).
• Surface area to mass ratio: neonates and small infants have a much higher surface-area-to-body-mass ratio than older children and adults. This means heat loss per unit mass is proportionally much greater — a fundamental reason for their vulnerability to hypothermia.
• Four mechanisms of heat loss: conduction (to cold surfaces), convection (to moving air), radiation (to cold nearby objects), and evaporation (from wet skin — the dominant route immediately after birth).
Thermal Emergencies: Why Temperature Matters in Paediatric Care
Temperature regulation is not a luxury function — it is a basic metabolic necessity. In neonates, the margin between normal thermoregulation and life-threatening hypothermia is measured in degrees and minutes, not hours. A wet neonate in a 22°C room with a fan nearby can lose enough heat through evaporation and convection in the first 20 minutes of life to drop below the hypothermic threshold — and without a functioning warm chain, that process begins immediately after delivery before any clinician acts. Understanding why temperature regulation matters in paediatric care requires understanding three distinct but related clinical scenarios: neonatal cold stress immediately after delivery, hypothermia in a sick or malnourished child, and hyperthermia from fever or heat illness.
Provided image
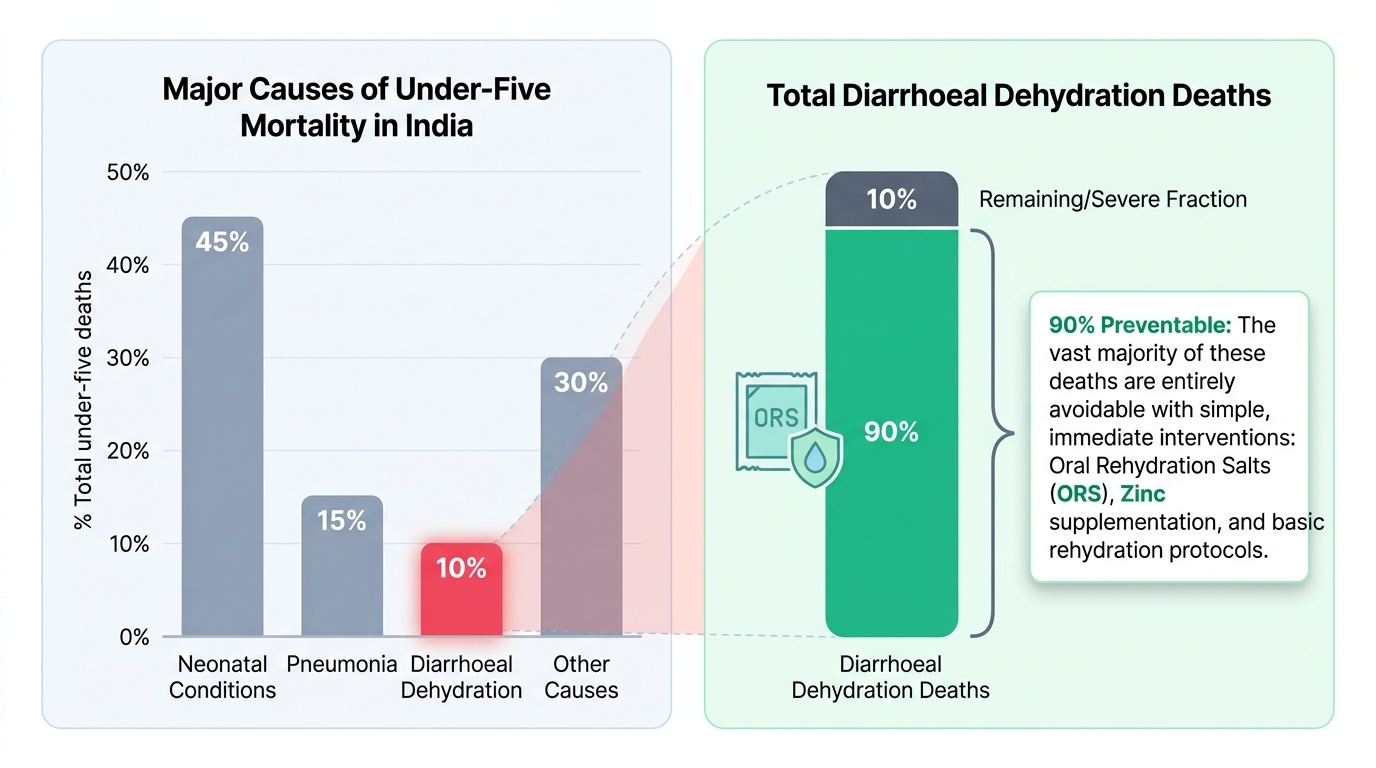
The burden of neonatal hypothermia in India is substantial. Studies in peripheral health facilities show that a significant proportion of neonates admitted to sick newborn care units are hypothermic on arrival, and hypothermia on admission is independently associated with higher mortality. The causal pathway is direct: hypothermia increases metabolic rate (the body attempts to generate heat), depletes glucose stores (hypoglycaemia is a common complication), worsens respiratory function (cold reduces surfactant activity), impairs immune function (increasing infection risk), and — if severe — leads to respiratory failure and cardiovascular collapse.
The WHO warm chain was developed specifically to interrupt this pathway at every step from delivery to discharge — a sequence of 10 interlinked actions ensuring no single point of care inadvertently breaks the thermal protection provided by the others. Kangaroo Mother Care (KMC), the second major intervention, uses the mother's body as a biological incubator — providing skin-to-skin warmth that is equivalent to a radiant warmer for stable low-birthweight infants, at zero cost and with additional benefits including breastfeeding promotion, maternal bonding, and reduced infection rates.
Recognising and managing hyperthermia — fever from infection, and heat stroke from environmental exposure — is an equally important skill because the neurological consequences of untreated heat stroke (hyperthermia >40°C with CNS dysfunction) are severe and rapidly irreversible.
Thermoregulation: Physiology and Vulnerability in Children
The physiological basis of temperature vulnerability in neonates lies in three interacting factors: an immature thermoregulatory response, a large surface area relative to body mass, and dependence on non-shivering thermogenesis (brown adipose tissue, BAT) rather than shivering. Understanding these mechanisms explains why the warm chain works and why environmental controls are not optional but physiologically essential.
In healthy adults and older children, the hypothalamus maintains core temperature within a narrow range (36.5–37.5°C) through a feedback loop: temperature receptors in the skin and hypothalamus send afferent signals; the hypothalamus coordinates effector responses — peripheral vasoconstriction to reduce heat loss, shivering to generate heat, and sweating/vasodilation to dissipate heat. Neonates have the hypothalamic control centre but lack the muscle mass for effective shivering thermogenesis. Their alternative is non-shivering thermogenesis via BAT metabolism: noradrenaline stimulates BAT to oxidise fatty acids with uncoupling protein-1 generating heat instead of ATP. This is effective at modest cold loads, but under severe cold stress or during illness (when BAT metabolism is impaired), it is rapidly overwhelmed.
The surface area to mass ratio of a term neonate is approximately 3× that of an adult, and of a preterm infant even higher. This means that per kilogram of body mass, neonates lose heat at a rate proportionally far exceeding adults. The four heat loss mechanisms are all amplified in neonates:
• Evaporation — the dominant route immediately after delivery: amniotic fluid on wet skin evaporates rapidly, causing rapid cooling. Prevention: dry immediately and thoroughly.
• Conduction — heat transferred to cold surfaces (cold delivery table, cold weighing scale). Prevention: warm all surfaces the baby contacts.
• Convection — heat carried away by air currents (open windows, fans, air-conditioning). Prevention: warm room, no draughts.
• Radiation — heat radiated to cold objects in the environment (cold walls, open windows). Prevention: radiant warmer, keep baby away from cold surfaces.
Preterm and low-birthweight infants have even less subcutaneous fat (a natural insulator), smaller BAT reserves, and greater surface area, making them the most vulnerable group.
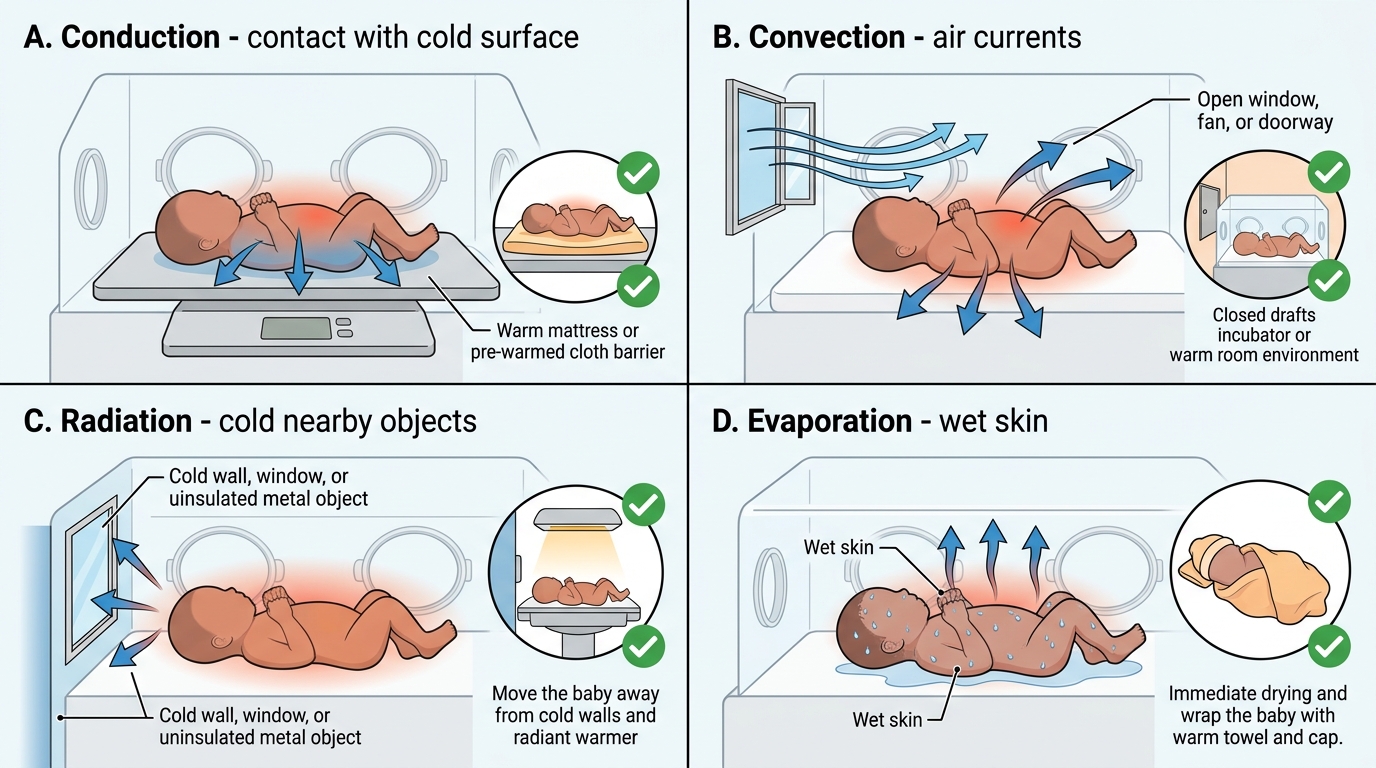
Mechanisms of Heat Loss in Neonates
Assessment Technique: Identifying Hypothermia and Hyperthermia
Temperature assessment in a child requires the correct site, instrument, and interpretation framework. Errors in technique produce misleading values — rectal temperature (the most accurate core temperature) differs from axillary temperature (the practical standard in paediatrics) by approximately 0.5°C, and oral temperature is not used routinely in young children due to the risk of biting the thermometer and lack of cooperation. In clinical paediatric practice in India, axillary temperature is the standard, and all reference values for paediatric temperature abnormalities are based on axillary measurement. The measurement is seemingly simple but is frequently done incorrectly in busy clinical settings: the thermometer placed at the edge of the axilla rather than the centre, the arm not held firmly, or the reading taken too early in a glass thermometer — each of these errors can produce a falsely low or falsely high reading. A falsely low reading may lead to under-recognition of fever; a falsely high reading may lead to unnecessary investigation. Developing the habit of correct technique from the beginning of clinical training prevents these systematic errors from becoming ingrained practice. The axillary route is also safe for neonates — rectal temperature measurement carries a risk of rectal perforation in very small or preterm neonates and is not the routine bedside method.
Provided image
Correct technique for axillary thermometry:
1. Ensure the axilla is dry (pat dry if sweating).
2. Place the thermometer bulb in the centre of the axilla (not at the edge).
3. Hold the arm firmly against the chest wall to ensure skin contact.
4. Leave for the duration specified by the thermometer type (digital: until beep; glass/mercury: 3–5 minutes).
5. Read immediately.
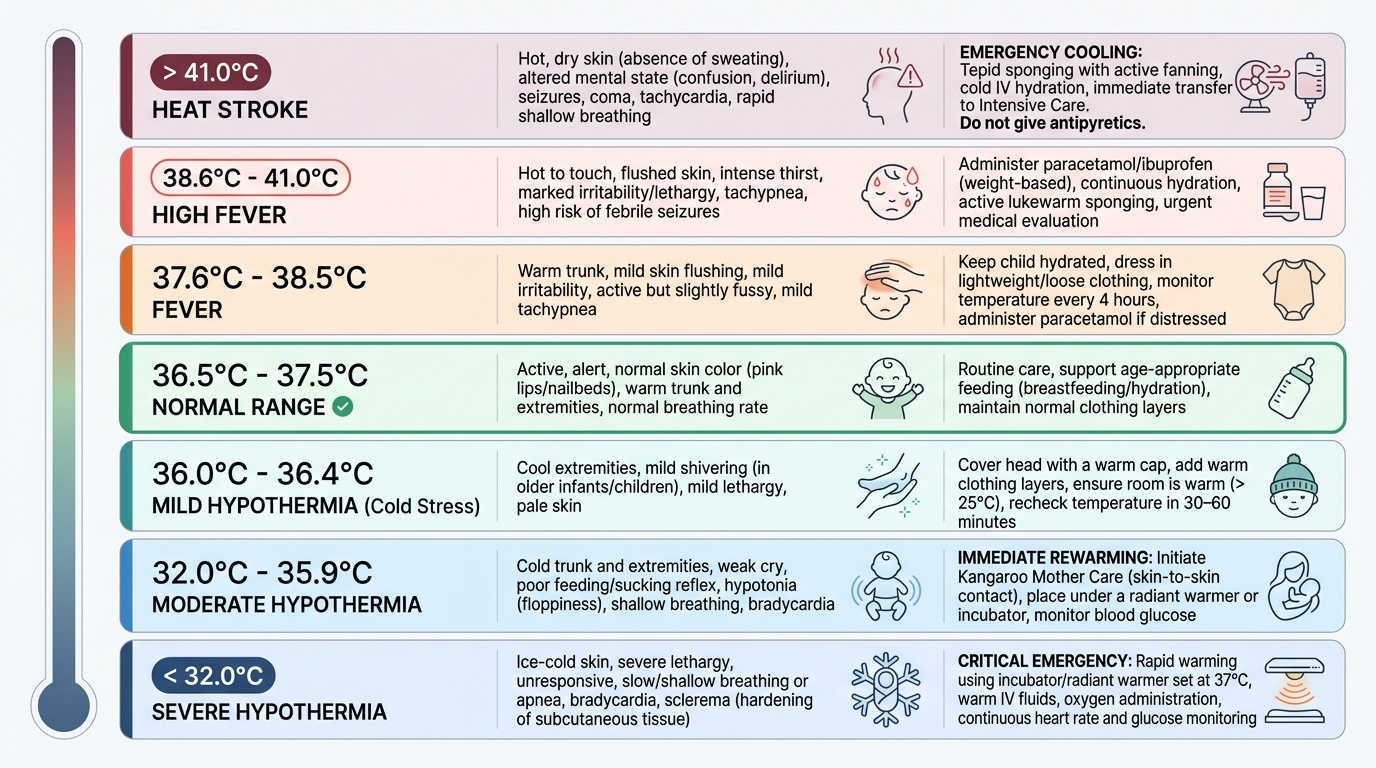
Temperature classification (axillary):
• Normal: 36.5–37.5°C
• Mild hypothermia: 36.0–36.4°C
• Moderate hypothermia: 32.0–35.9°C
• Severe hypothermia: <32°C
• Fever: >37.5°C
• High fever: >39°C
• Hyperpyrexia / heat stroke risk: >40°C
Clinical signs of hypothermia (beyond the thermometer reading):
• Cold to touch — skin feels cold, especially extremities
• Lethargy, poor feeding, weak cry — metabolic depression
• Peripheral cyanosis, pallor
• Bradycardia, bradypnoea in severe hypothermia
• Hypoglycaemia (check BGL in all hypothermic neonates — hypothermia depletes glucose)
• In neonates: reduced spontaneous movements, poor muscle tone
Clinical signs of heat stroke (distinguishing from simple fever):
• Core temperature >40°C
• Absence of sweating (anhidrosis) in classical heat stroke (not seen in exertional)
• CNS dysfunction: confusion, delirium, seizures, loss of consciousness
• Hot, dry skin
• History of exposure to hot environment
SELF-CHECK
A 3-day-old neonate has axillary temperature 35.2°C. He is lethargic and not feeding well. What is the correct classification and the single most important immediate action?
A. Mild hypothermia — wrap in extra blanket and reassess in 2 hours
B. Moderate hypothermia — initiate rewarming (KMC or radiant warmer) and check blood glucose immediately
C. Severe hypothermia — intubate and ventilate first
D. Normal variant — axillary temperature is always lower; no action needed
Reveal Answer
Answer: B. Moderate hypothermia — initiate rewarming (KMC or radiant warmer) and check blood glucose immediately
35.2°C is moderate hypothermia (32–35.9°C range). The immediate actions are: initiate rewarming (KMC skin-to-skin or radiant warmer), check blood glucose (hypothermia depletes glucose — hypoglycaemia is a common complication), feed (if able) or establish IV dextrose. Mild hypothermia is 36.0–36.4°C; severe is <32°C. Extra blanket alone is insufficient for moderate hypothermia without addressing the heat source. Intubation is not indicated unless respiratory failure is present.