Page 15 of 31
PE24.{5,15} | Unconscious Child — SDL Guide
Learning Objectives
- Describe the aetio-pathogenesis, clinical approach, and management of an unconscious child using AEIOU-TIPS mnemonic
- Assess the level of consciousness using AVPU scale and paediatric GCS
- Demonstrate emergency treatment of a child with convulsions or coma: airway positioning, IV/PR diazepam administration, and 10% dextrose for hypoglycaemia
- Position an unconscious child safely, with and without suspected spinal trauma, in a simulated environment
INSTRUCTIONS
An unconscious child is one of the most time-critical presentations in paediatric emergency medicine. Every minute of delay in identifying and treating a reversible cause — hypoglycaemia, seizure, meningitis, or airway obstruction — worsens neurological outcome. This module equips you to rapidly assess the level of consciousness using validated tools, systematically work through differential diagnoses, and execute the first 60 seconds of emergency management correctly. These skills are tested both in IMNCI danger-sign recognition and in supervised clinical practice.
References
- Ghai Essential Pediatrics, 9th edition, Ch 18 (Paediatric Emergencies) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 71 (Neurological Emergencies) (textbook)
- IAP Guidelines on Paediatric Emergency Management, 2022 (guideline)
- WHO IMNCI Chart Booklet — Danger Signs and Referral Criteria (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-year-old boy is brought to the emergency department by his mother at 11 PM. She found him unresponsive in bed an hour ago — he had been febrile for two days and had one witnessed seizure this afternoon. He does not respond to his name. His eyes open only when you pinch his finger firmly. Capillary blood glucose reads 38 mg/dL. You have 60 seconds to act. What do you do first — and in what order?
WHY THIS MATTERS
Impaired consciousness in a child is a medical emergency because the causes are numerous, several are immediately reversible (hypoglycaemia, seizure), and delayed recognition of any of them carries a high risk of permanent neurological damage or death. In IMNCI triage, 'lethargic or unconscious' is one of the five general danger signs that mandates urgent referral regardless of the presenting complaint. In the Indian paediatric emergency setting, hypoglycaemia, CNS infections (bacterial meningitis, cerebral malaria), and status epilepticus are the leading treatable causes — and missing any of them during the first assessment is the single most preventable error. Learning to apply AVPU, paediatric GCS, and the AEIOU-TIPS framework rapidly and correctly is therefore foundational to safe paediatric emergency care.
RECALL
Before proceeding, recall the following from your preclinical studies:
• Reticular activating system (RAS): the ascending reticular activating system in the brainstem and thalamus maintains wakefulness. Bilateral cortical or brainstem dysfunction — from metabolic, infectious, or structural causes — disrupts it and produces coma.
• Glucose homeostasis: the brain is entirely dependent on circulating glucose. A child's glycogen stores are small relative to metabolic demand; stress, fever, or poor oral intake can precipitate hypoglycaemia rapidly.
• Seizures: sustained seizure activity (status epilepticus >5 minutes) leads to progressive neuronal injury through glutamate excitotoxicity and energy failure — time-to-treatment is the critical variable.
You will build on these physiological foundations to understand why your assessment and intervention sequence matters.
Why Consciousness Matters: Indication and Clinical Relevance
Consciousness is the brain's most integrative function — requiring an intact arousal system (reticular activating system, RAS) and intact cortical processing. When a child presents with altered or absent consciousness, the clinician is facing a convergence of potentially lethal pathologies, each of which demands a specific intervention. The urgency is categorical: unlike an adult with diabetes who can signal distress, a young child cannot communicate a worsening state, making external rapid assessment the only reliable guide.
The IMNCI danger signs — unable to drink or breastfeed, vomiting everything, convulsions, lethargic or unconscious — were designed for community-level health workers to triage children under 5 who need immediate referral. 'Lethargic or unconscious' is the neurological danger sign, and any child meeting it bypasses general assessment and proceeds directly to emergency stabilisation. In a hospital setting, the same priority applies: the child who arrives obtunded or comatose is assessed and treated simultaneously, not sequentially.
Epidemiology of paediatric coma in India (referencing IAP data) shows hypoglycaemia, CNS infections (bacterial meningitis, cerebral malaria, viral encephalitis), and status epilepticus as the three most common reversible causes. Each requires a different first-line intervention: dextrose for the first, antibiotics and antivirals for the second, and benzodiazepines for the third. Identifying the primary cause — or covering all three simultaneously when the cause is unclear — is the core skill this module builds.
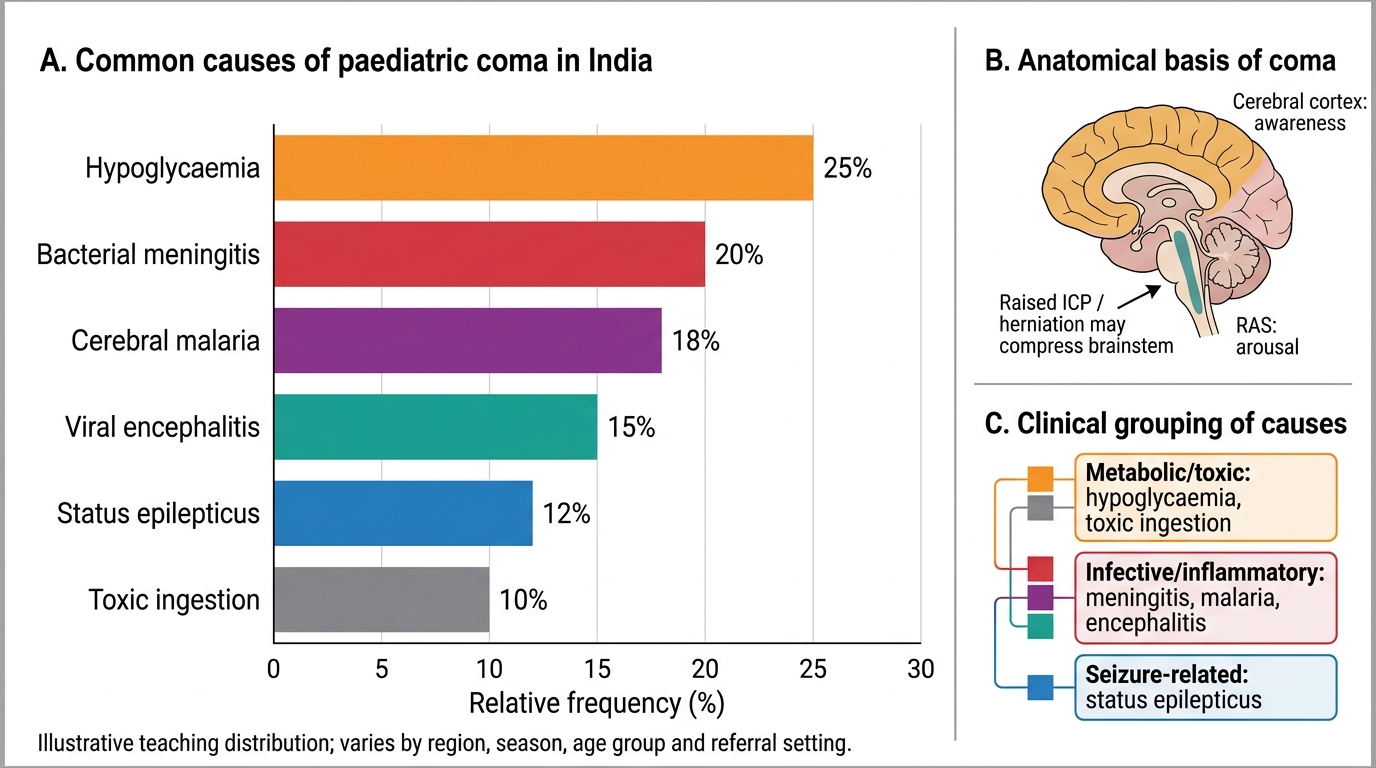
Common Causes of Paediatric Coma in India
Physiological Basis of Consciousness and AVPU/GCS
Consciousness depends on the integrity of two anatomical components: the ascending reticular activating system (RAS) in the brainstem and diencephalon (arousal) and the cerebral cortex (awareness). Both must be intact for normal consciousness. Coma can result from: (a) bilateral cortical injury or suppression (metabolic, toxic, hypoxic); (b) focal or diffuse brainstem pathology disrupting the RAS; or (c) raised intracranial pressure sufficient to produce transtentorial herniation compressing both. Understanding this anatomy explains why a child with meningococcal meningitis becomes comatose through cerebral oedema and raised ICP, while a child with a small subdural haematoma may remain alert because neither the RAS nor the whole cortex is yet compromised. This anatomical framework also clarifies why metabolic coma (hypoglycaemia, hyponatraemia, hepatic failure) is typically reversible — the structure is intact but transiently non-functional — whereas structural coma from compression or infarction carries a higher risk of permanent deficit even with rapid treatment.
Provided image
Two validated scales assess the level of consciousness at the bedside:
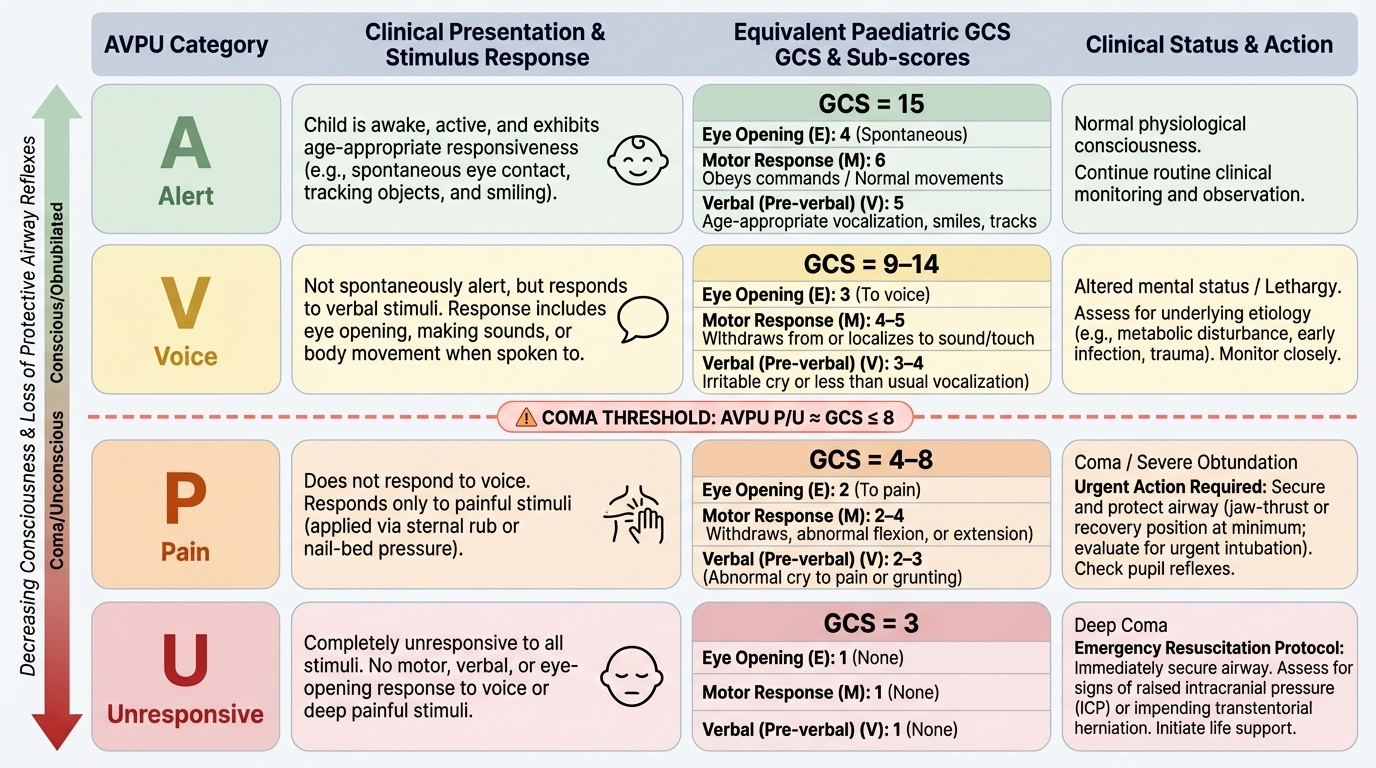
The AVPU scale is a rapid 4-point qualitative screen:
• A — Alert: child is awake and age-appropriately responsive
• V — Voice: responds to verbal stimuli (eye opening, sound, movement) but not spontaneously alert
• P — Pain: responds only to painful stimuli (sternal rub or nail-bed pressure)
• U — Unresponsive: no response to any stimulus
AVPU P/U approximately corresponds to GCS ≤8 (coma threshold). It is the IMNCI/community-level tool for rapid field triage.
The paediatric GCS (scale 3–15) quantifies the level more precisely across three domains. Critically, the verbal component is modified for pre-verbal children to assess developmentally appropriate responses rather than adult speech:
• Eye opening: 4 (spontaneous) → 3 (to voice) → 2 (to pain) → 1 (none)
• Motor: 6 (obeys commands) → 5 (localises pain) → 4 (withdraws) → 3 (abnormal flexion) → 2 (extension) → 1 (none)
• Verbal (pre-verbal modification): 5 (age-appropriate vocalisation/smile/tracking) → 4 (less than usual/irritable cry) → 3 (abnormal cry to pain) → 2 (grunts) → 1 (none)
GCS ≤8 is the clinical threshold for coma; ≤8 also mandates airway protection (jaw-thrust or recovery position at minimum; consider intubation if available). Serial GCS measurements track deterioration or improvement over time — a falling GCS is as important as the absolute value.
IMPORTANT: AVPU P/U ≈ GCS ≤8 — the coma threshold. AVPU P or U requires immediate airway management and urgent investigation regardless of other findings.
SELF-CHECK
A 6-year-old child opens her eyes only when you pinch her finger firmly. She makes incomprehensible sounds and withdraws her arm from pain. What is her AVPU grade, her GCS score, and the immediate next priority?
A. AVPU = V, GCS = 7, priority is blood glucose check
B. AVPU = P, GCS = 8, priority is airway positioning and blood glucose check
C. AVPU = P, GCS = 9, priority is blood pressure measurement
D. AVPU = U, GCS = 8, priority is CT head
Reveal Answer
Answer: B. AVPU = P, GCS = 8, priority is airway positioning and blood glucose check
Eye opening to pain = 2, verbal incomprehensible = 2, motor withdrawal = 4 → GCS = 8. AVPU = P (responds to Pain only). GCS ≤8 mandates immediate airway positioning (recovery position or jaw-thrust). Blood glucose must be checked simultaneously as hypoglycaemia is the most rapidly reversible life-threatening cause and takes 5 seconds to test.
Systematic Assessment: ABCDE and the AEIOU-TIPS Framework
The systematic assessment of an unconscious child follows the ABCDE framework, performed simultaneously with targeted history-taking from the caregiver. The framework ensures that life-threatening problems are treated in priority order — airway before breathing before circulation before disability — and prevents the common error of becoming fixated on a diagnosis before the child is haemodynamically stable. It is important to understand that in a paediatric emergency, assessment and treatment are not sequential steps; they occur in parallel. While one team member manages the airway, a second establishes IV access and draws blood, a third takes history from the parent, and a fourth records observations. This simultaneous team approach is why structured frameworks exist — they allocate tasks by priority so that nothing is forgotten and no time is wasted. Even working alone, internalising the ABCDE sequence prevents the common failure of an inexperienced clinician spending five minutes trying to obtain history before securing an airway.
ABCDE rapid assessment:
• A — Airway: Is it patent? Tongue fall and secretions are the most common obstructions in a comatose child. Head-tilt chin-lift (or jaw-thrust if trauma is possible), suction if needed, recovery position.
• B — Breathing: Rate, depth, work of breathing. Central hypoventilation may indicate brainstem compression.
• C — Circulation: Heart rate, capillary refill time, skin perfusion, blood pressure. Shock worsens cerebral perfusion.
• D — Disability: AVPU or GCS, pupil size and reactivity (unilateral fixed dilated pupil = herniation), posture (decorticate vs decerebrate = structural lesion vs metabolic at higher vs lower brainstem level), BGL.
• E — Exposure: Full undress for fever, rashes (petechiae/purpura = meningococcaemia), signs of trauma, jaundice.
The most important single test at step D is the bedside blood glucose (BGL). Hypoglycaemia is both the most common and the most rapidly reversible cause of altered consciousness in children, and it is missed if not measured. Do not skip this test.
Once stabilised, the history from the caregiver drives the aetiological search. The AEIOU-TIPS mnemonic organises causes of coma into a systematic, memorable framework:
• A — Alcohol / Acidosis (metabolic acidosis from DKA, sepsis, inborn errors of metabolism)
• E — Epilepsy / Encephalopathy
• I — Insulin / hypoglycaemia (most common and most treatable — DON'T EVER FORGET to check BGL)
• O — Overdose / Opiates / Organophosphates (accidental poisoning in toddlers)
• U — Uraemia / renal failure
• T — Trauma / Temperature (hyperthermia, hypothermia)
• I — Infection (meningitis, encephalitis, cerebral malaria, septic encephalopathy)
• P — Psychogenic (rare in children; diagnosis of exclusion)
• S — Stroke / Structural (space-occupying lesion, raised ICP, cerebrovascular events)
Each category has clinical pointers that allow bedside prioritisation: a petechial rash points to meningococcaemia (I); a fever and neck stiffness to bacterial meningitis (I); a history of fasting + seizure to hypoglycaemia (I-for-insulin); dilated pupils and empty tablet strip to overdose (O); a bruised scalp to non-accidental injury or trauma (T).
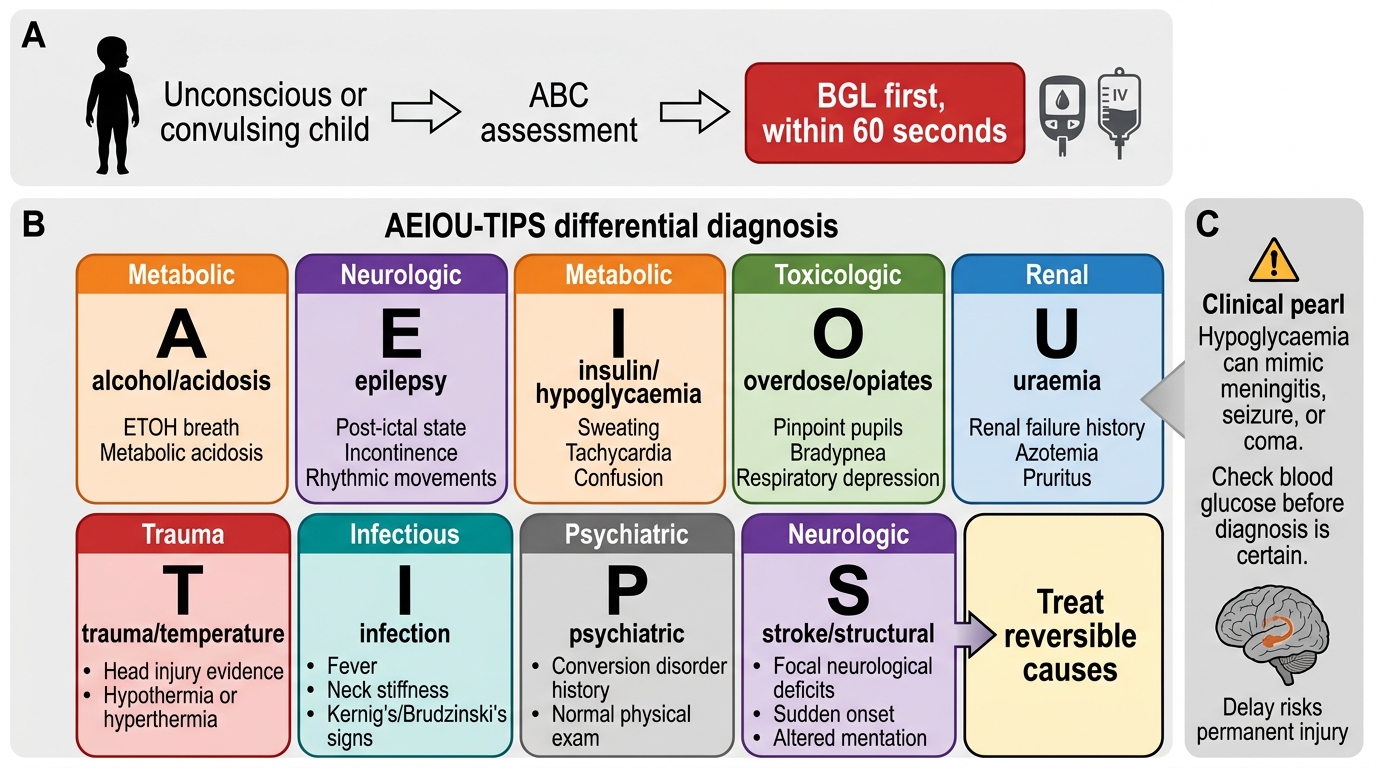
AEIOU-TIPS Approach to the Unconscious Child
CLINICAL PEARL
DON'T EVER FORGET hypoglycaemia. In any unconscious or convulsing child, check the blood glucose within the first 60 seconds of assessment — before you have a diagnosis, before you get IV access, at the same time as everything else. A child whose GCS is 6 from hypoglycaemia looks identical to a child with bacterial meningitis at first glance. Treating hypoglycaemia takes 30 seconds and can restore consciousness; missing it for 10 minutes while you do a lumbar puncture can produce permanent hippocampal damage. The rule is: BGL first, always.