Page 2 of 23
PE25.1 | Acute Otitis Media — SDL Guide (Part 2)
Management of AOM
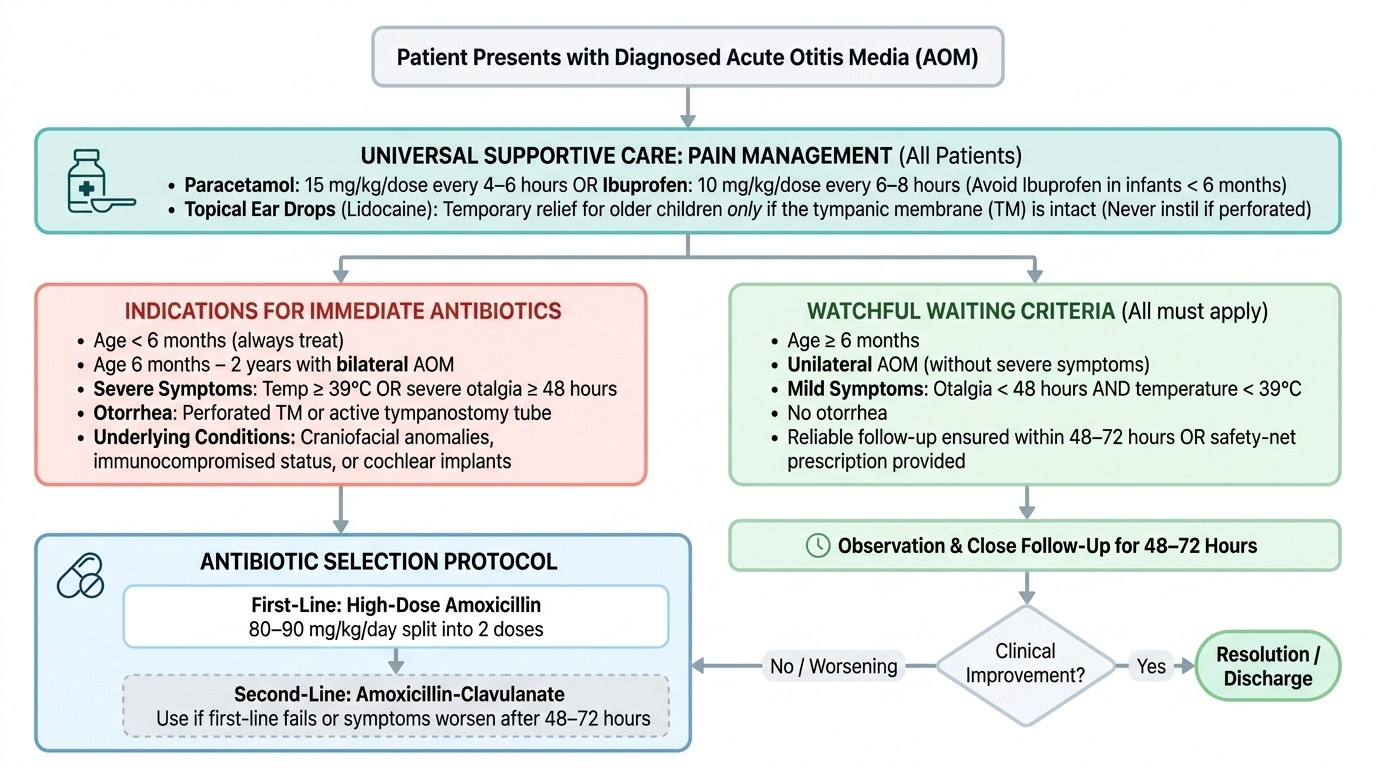
The management of AOM in children involves a two-stage decision framework: first, whether to initiate antibiotics immediately or to adopt watchful waiting (observation without antibiotics) for 48-72 hours; and second, if antibiotics are chosen, selecting the correct agent at the correct weight-based dose. This decision is driven by three clinical variables — the child's age, the severity of the presentation, and whether the AOM is unilateral or bilateral — each of which shifts the risk-benefit calculation. Watchful waiting is not the same as neglect: it is an evidence-based strategy supported by IAP and AAP guidelines, applicable only when specific eligibility criteria are met, and always accompanied by analgesics, close follow-up, and a clear safety-net instruction to the parent to return immediately if the child worsens. Pain management is always instituted regardless of the antibiotic decision — otalgia is distressing and requires treatment independently. The underlying principle is that many AOM episodes (particularly those caused by M. catarrhalis and NTHi) will resolve spontaneously, and judicious antibiotic use reduces selective pressure on resistant organisms while avoiding the adverse effects of unnecessary antibiotics.
Provided image
Pain relief (universal for all AOM):
- Paracetamol 15 mg/kg/dose every 4-6 hours OR ibuprofen 10 mg/kg/dose every 6-8 hours (avoid in infants <6 months). Both are effective analgesics for AOM-associated otalgia.
- Ear drops (lidocaine or naturopathic) may provide temporary topical relief in older children without perforation — never instil ear drops into a perforated ear.
Watchful waiting criteria (all of the following must apply):
- Child is ≥6 months of age (children <6 months always receive antibiotics)
- Unilateral AOM (bilateral AOM in children <2 years requires immediate antibiotics)
- Non-severe symptoms (mild otalgia <48 h, temperature <39°C)
- No otorrhoea
- Parent can reliably return for follow-up within 48-72 hours or has a safety-net prescription
Indications for IMMEDIATE antibiotic therapy:
- Any child <6 months
- Bilateral AOM in children <2 years
- Severe AOM (temperature ≥39°C or otalgia ≥48 h)
- Otorrhoea (perforated TM or through a tympanostomy tube)
- AOM with underlying conditions (craniofacial anomaly, immunocompromise, cochlear implant)
First-line antibiotic: High-dose Amoxicillin
- Dose: 80-90 mg/kg/day in 2-3 divided doses (weight-based — NEVER a fixed adult dose)
- Duration: 10 days for children <2 years or with severe/perforated AOM; 5-7 days for children ≥2 years with mild AOM
- High-dose strategy overcomes the relative amoxicillin resistance of some S. pneumoniae strains (requires serum concentrations above the MIC for >40-50% of the dosing interval)
Second-line therapy (treatment failure — no improvement at 72 h or worsening):
- Amoxicillin-clavulanate 90 mg/kg/day (amoxicillin component) — covers beta-lactamase-producing NTHi and M. catarrhalis
- Cefuroxime axetil 30 mg/kg/day or ceftriaxone 50 mg/kg IM/IV for 3 days (if oral therapy not tolerated)
Allergy management:
- Non-anaphylaxis penicillin allergy: cefdinir, cefpodoxime, or cefuroxime
- History of anaphylaxis to penicillin: clindamycin (covers S. pneumoniae but NOT NTHi) + cefdinir (if low cross-reactivity risk)
Indications for ENT referral:
- Recurrent AOM (≥3 episodes in 6 months or ≥4 in 12 months) → consideration of tympanostomy tubes
- Persistent otitis media with effusion >3 months with hearing loss
- Suspected suppurative complications
Complications of AOM:
- Intratemporal: CSOM (chronic perforation + discharge >6 weeks), mastoiditis (post-auricular swelling, tenderness, pinna displaced forward), hearing loss
- Intracranial (rare but serious): meningitis, extradural/subdural abscess, sigmoid sinus thrombosis, brain abscess
- Warning signs requiring urgent referral: post-auricular redness/swelling, pinna displaced forward, facial nerve palsy, high fever not settling, altered sensorium
CLINICAL PEARL
The single most important dosing rule for AOM: amoxicillin must be prescribed at HIGH DOSE — 80-90 mg/kg/day, NOT the standard 40-45 mg/kg/day used for other infections. The high dose is essential to achieve middle-ear fluid concentrations above the MIC of relatively penicillin-resistant S. pneumoniae. Using the standard dose in a child with pneumococcal AOM risks treatment failure. Always calculate the dose by weight; never use an adult fixed dose. Additionally, remember: bilateral AOM in a child under 2 years always needs antibiotics — do not apply watchful waiting to this group regardless of symptom severity.
Self-Assessment — AOM
This section helps you consolidate your understanding of AOM by integrating the clinical, pathophysiological, and therapeutic knowledge covered in this module. AOM is among the highest-volume diagnoses you will encounter in paediatric outpatient practice, and errors in diagnosis — particularly over-diagnosis without otoscopic confirmation, or under-dosing of amoxicillin — directly harm patients and contribute to antibiotic resistance. Before attempting the self-assessment quiz, take a moment to mentally trace the full management pathway for a child presenting with ear pain and fever: you should be able to articulate whether watchful waiting applies, what dose and duration of amoxicillin to prescribe if antibiotics are needed, what defines treatment failure, and which complication signs demand same-day ENT referral. The ability to answer these questions fluently and accurately constitutes readiness for clinical practice.
Key recall points:
- The three commonest bacterial pathogens of AOM: S. pneumoniae > NTHi > M. catarrhalis
- AOM diagnosis requires: acute onset + middle-ear effusion (bulging TM) + inflammatory signs
- Watchful waiting is safe for non-severe, unilateral AOM in children ≥6 months
- First-line antibiotic = high-dose amoxicillin 80-90 mg/kg/day (NOT standard dose)
- Treatment failure = no improvement at 72 h → switch to amoxicillin-clavulanate
- Complications to recognise: mastoiditis (pinna displaced forward), intracranial spread
Test yourself on these principles before the quiz.
SELF-CHECK
A 3-year-old child has been treated with amoxicillin 45 mg/kg/day for AOM for 3 days with no improvement. He now has a temperature of 39.5°C and the right tympanic membrane remains bulging. What is the most appropriate next step?
A. Continue the same amoxicillin dose for another 5 days
B. Switch to amoxicillin-clavulanate at 90 mg/kg/day (amoxicillin component)
C. Start oral co-trimoxazole as second-line therapy
D. Refer immediately for tympanocentesis without changing antibiotics
Reveal Answer
Answer: B. Switch to amoxicillin-clavulanate at 90 mg/kg/day (amoxicillin component)
This represents treatment failure (no improvement at 72 h). The most likely cause is beta-lactamase-producing NTHi or M. catarrhalis, or a relatively penicillin-resistant S. pneumoniae. The correct second-line therapy is amoxicillin-clavulanate at 90 mg/kg/day (amoxicillin component) to cover beta-lactamase producers, while also noting that the standard-dose amoxicillin used here (45 mg/kg/day) was subtherapeutic for AOM — high-dose (80-90 mg/kg/day) should have been used initially. Co-trimoxazole is not recommended due to high resistance rates. Tympanocentesis is reserved for immunocompromise, neonates, or multiple antibiotic failures.