Page 16 of 23
PE25.6 | Lower Respiratory Infection — SDL Guide
Learning Objectives
- Describe the clinical features of bronchiolitis, wheeze-associated LRTI, pneumonia, and empyema and distinguish each entity at the bedside
- Explain the aetiopathogenesis of each LRTI entity including the role of RSV, Streptococcus pneumoniae, and Staphylococcus aureus
- Apply WHO IMNCI age-specific fast-breathing thresholds to classify pneumonia severity as non-severe, severe, or very severe
- Identify chest indrawing as a sign of severe pneumonia and danger signs requiring urgent referral
- Select appropriate antibiotics and setting of care for pneumonia based on severity classification
- Describe the supportive management of bronchiolitis and the bronchodilator trial for wheeze-associated LRTI
- Outline the diagnosis and drainage-based management of empyema thoracis in children
- Describe the role of PCV and Hib vaccination in prevention of bacterial LRTI
INSTRUCTIONS
Lower respiratory infections are the leading cause of death from infectious disease in children under 5 years in India and globally. The WHO Integrated Management of Neonatal and Childhood Illness (IMNCI) algorithm — with its age-specific fast-breathing thresholds and severity tiers — is the single most important clinical tool for managing pneumonia at every level of health care, from the community health worker to the tertiary hospital. This module builds your ability to navigate the full LRTI spectrum, apply the IMNCI classification correctly, and select evidence-based treatment appropriate to each child's severity and setting.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 16 — Respiratory Disorders (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 428–432 — Lower Respiratory Infections (textbook)
- WHO/UNICEF IMNCI Chart Booklet, Revised 2014 (guideline)
- IAP Guidelines on Management of Community-Acquired Pneumonia 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old girl is brought to the health centre with a 3-day history of cough and rapid breathing. Her mother has been giving her home remedies but she is not improving. On examination, she is irritable, breathing rate is 55 per minute, temperature 38.4°C, and there is visible lower chest-wall indrawing. Oxygen saturation is 94% on room air. Lung auscultation reveals fine crackles at the right base. You are the duty doctor at a first-level referral centre with oral and injectable antibiotics, oxygen, and a chest X-ray available. What is the correct classification and initial management plan for this child?
WHY THIS MATTERS
Pneumonia alone kills an estimated 1 lakh children under 5 every year in India, and lower respiratory infections collectively account for more child deaths than diarrhoea and malaria combined. The majority of these deaths are preventable with correct and timely management. The IMNCI fast-breathing rule is one of the most validated clinical tools in global health — it was developed precisely so that a health worker without a stethoscope or X-ray can identify children who need antibiotics, and clinicians at every level need to know it precisely. The distinction between non-severe and severe pneumonia determines not only the antibiotic chosen but the entire setting of care — a mistake at this step can mean a child who needed admission goes home and deteriorates, or a child who needed only oral amoxicillin is unnecessarily hospitalised.
RECALL
Recall from your Anatomy studies that the lower respiratory tract begins at the level of the larynx and includes the trachea, bronchi, bronchioles, and alveoli. From Physiology, recall that ventilation depends on the elastic recoil of lung tissue and the muscular effort of the diaphragm and intercostal muscles; when lung compliance falls (as in consolidation) or airways narrow (as in bronchiolitis), increased respiratory effort is clinically visible as raised respiratory rate, intercostal recession, subcostal indrawing, and nasal flaring. Recall also from Immunology that maternal IgG crosses the placenta and provides passive protection for the first 3–6 months of life; thereafter, infants rely on their own developing immune response, which makes this age window highly vulnerable to respiratory pathogens.
Clinical Presentation: Recognising the LRTI Spectrum
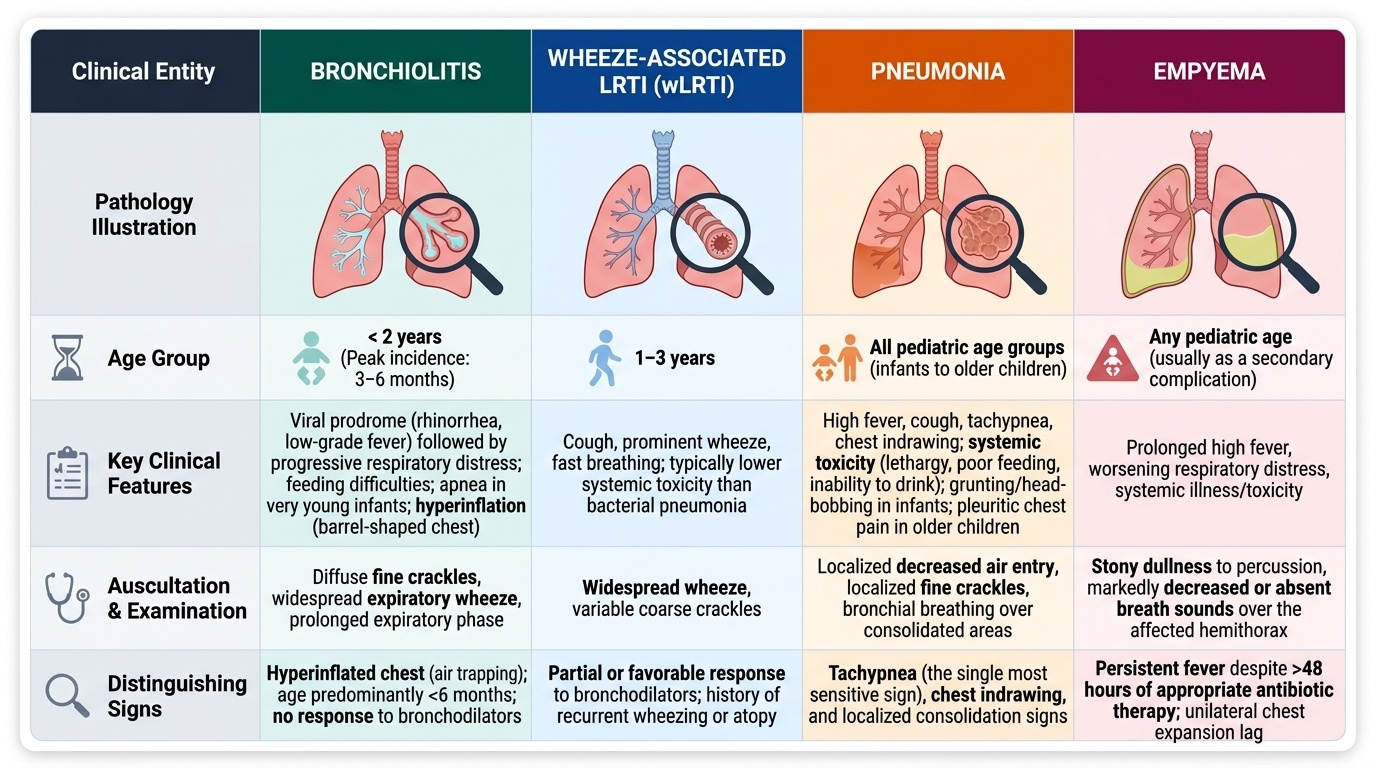
Lower respiratory tract infections in children span a spectrum of four distinct clinical entities, each with a characteristic age distribution, clinical presentation, and management approach. Recognising which entity is present — and where on the severity spectrum it falls — is the core clinical skill this module develops.
Provided image
Bronchiolitis is an acute viral infection of the small airways (bronchioles) characterised by inflammatory oedema, excessive mucus secretion, and partial luminal obstruction. It predominantly affects infants under 2 years of age, with peak incidence at 3–6 months. The clinical picture is one of a viral prodrome (rhinorrhoea, low-grade fever) followed by worsening respiratory distress with a characteristic prolonged expiratory wheeze and hyperinflation. On examination, the chest may be barrel-shaped (due to air-trapping), with diffuse fine crackles and widespread wheeze. Infants are often too young for productive coughing and may present with feeding difficulty or apnoea.
Wheeze-associated lower respiratory tract infection (wLRTI) overlaps with bronchiolitis in younger infants but is more commonly seen in children aged 1–3 years. It represents viral-triggered bronchospasm superimposed on a lower respiratory infection. Unlike pure bronchiolitis, wLRTI may show a partial bronchodilator response. Clinically, these children have cough, wheeze, and sometimes fast breathing, but typically less severe systemic toxicity than bacterial pneumonia.
Pneumonia is inflammation of the lung parenchyma — alveoli and distal airways — leading to alveolar consolidation. In children, it presents with fever, cough, and respiratory distress (fast breathing, indrawing). The hallmark clinical findings are tachypnoea (the single most sensitive sign), chest indrawing, and localised decreased air entry with crackles on auscultation. Systemic toxicity (lethargy, poor feeding, inability to drink) marks severe disease. In infants, grunting and head-bobbing may indicate severe hypoxia. In older children, pleuritic chest pain and dullness to percussion suggest parapneumonic complications.
Empyema thoracis is the accumulation of infected pus in the pleural space as a complication of pneumonia. It presents with prolonged fever unresponsive to antibiotics, increasing respiratory distress, and dullness to percussion with absent breath sounds over the effusion. Systemic signs of sepsis are often prominent. Mediastinal shift may occur with large collections.
Aetiopathogenesis and Pathophysiology
The aetiology of each LRTI entity follows a consistent age-pathogen relationship that reflects the interaction of developmental immune maturity, anatomical airway size, and pathogen tropism. Understanding this relationship prevents the common error of applying pneumonia treatment to bronchiolitis or missing bacterial co-infection in a child with viral wheeze.
Bronchiolitis: Respiratory syncytial virus (RSV) is responsible for up to 80% of bronchiolitis cases worldwide. Other causative viruses include human metapneumovirus, rhinovirus, influenza, and parainfluenza. RSV infects the bronchiolar epithelium, causing epithelial necrosis, submucosal oedema, and luminal obstruction by sloughed cells and mucus plugs. The resulting partial obstruction leads to ball-valve air-trapping, hyperinflation, and ventilation-perfusion mismatch. Secondary bacterial infection is uncommon in classic bronchiolitis.
Wheeze-associated LRTI: Viral pathogens (rhinovirus, RSV, hMPV) trigger both airway inflammation and smooth-muscle bronchoconstriction in children with atopic predisposition. The pathophysiology involves mast-cell degranulation, leukotriene release, and IgE-mediated early responses in genetically susceptible hosts — this represents the interface between infectious LRTI and early asthma.
Bacterial pneumonia: Streptococcus pneumoniae is the single commonest bacterial cause of pneumonia in children across all age groups. Haemophilus influenzae type b (Hib) was previously important but has declined markedly with universal Hib vaccination. In neonates, Group B Streptococcus and enteric Gram-negatives predominate. In school-age children, Mycoplasma pneumoniae causes atypical pneumonia. Pneumococcal pneumonia produces lobar or segmental consolidation via filling of alveoli with inflammatory exudate (hepatisation), impairing gas exchange.
Viral pneumonia (RSV, influenza, measles, COVID-19) typically causes interstitial pneumonitis — inflammation of the alveolar walls and interstitium — producing a diffuse, bilateral, hazy pattern on X-ray rather than lobar consolidation.
Empyema: Results from direct extension of bacterial pneumonia into the pleural space. In Indian children, Staphylococcus aureus and Streptococcus pneumoniae are the most common causative organisms. The pleural exudate progresses through three stages: exudative (free-flowing), fibrinopurulent (loculated with fibrin), and organised (thick peel restricting lung expansion). Early drainage in the exudative stage is more effective and less complex.
IMPORTANT NOTE on epidemiology: Severe pneumonia disproportionately affects malnourished children, those not exclusively breastfed, those without PCV vaccination, and those living in overcrowded households with indoor air pollution exposure.
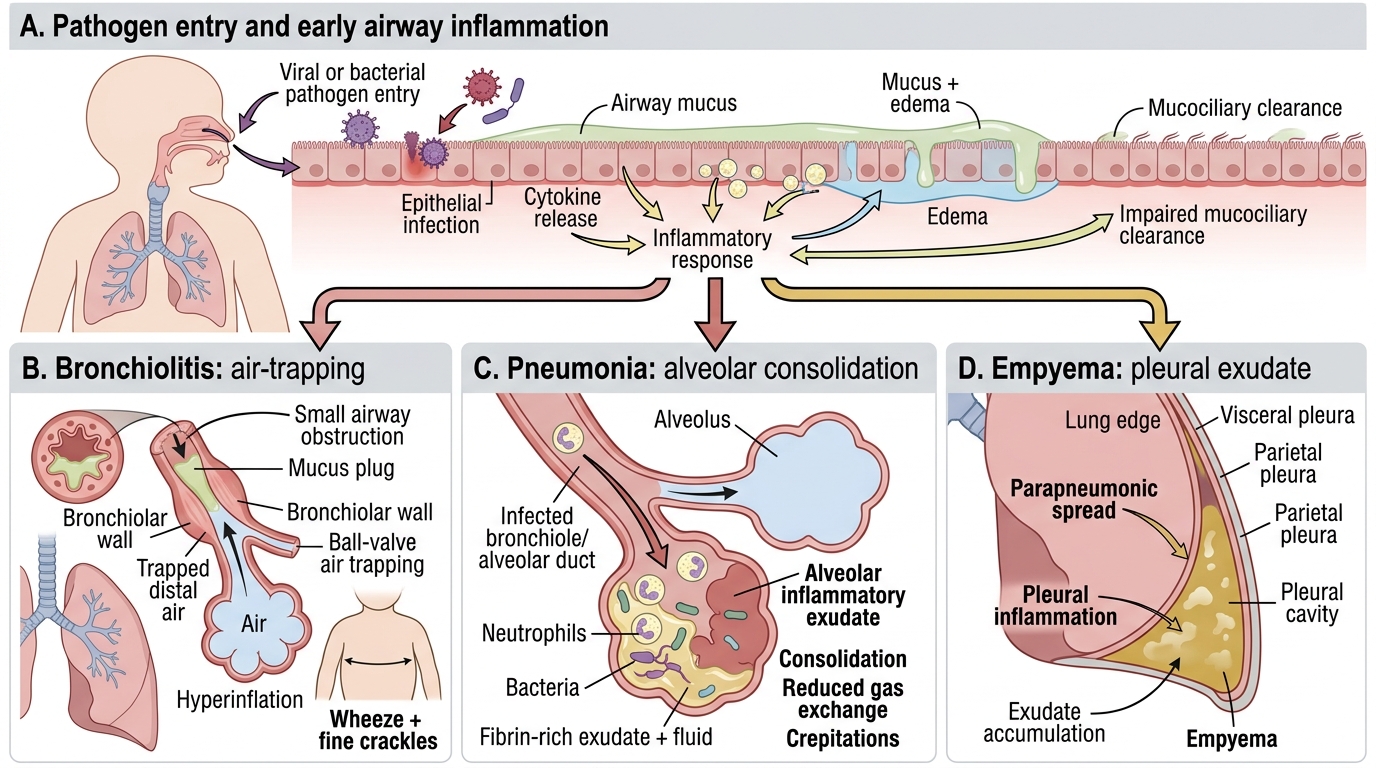
Pathophysiology of Bronchiolitis, Pneumonia, and Empyema
SELF-CHECK
A 6-month-old infant presents with 2 days of cough, runny nose, low-grade fever, and now breathing at 58 per minute. On examination there is diffuse wheeze, bilateral fine crackles, and a barrel-shaped chest. There is no chest indrawing. What is the most likely diagnosis and the most important immediate step?
A. Severe pneumonia — administer IV ampicillin immediately
B. Bronchiolitis — provide supportive care (oxygen if SpO2 <92%, maintain hydration, avoid routine bronchodilators)
C. Bronchiolitis — administer a salbutamol nebulisation trial and observe for response
D. Non-severe pneumonia — discharge with oral amoxicillin
Reveal Answer
Answer: B. Bronchiolitis — provide supportive care (oxygen if SpO2 <92%, maintain hydration, avoid routine bronchodilators)
The clinical picture is classic bronchiolitis: infant under 2 years, viral prodrome, bilateral wheeze, crackles, hyperinflation (barrel chest), and no chest indrawing. The cornerstone of management is supportive care — oxygen for SpO2 below 92%, careful nasogastric or IV hydration if unable to feed, and nasal suctioning for mucus. Routine bronchodilator use is NOT recommended by evidence-based guidelines (trials show no consistent benefit). IV antibiotics are not indicated in uncomplicated viral bronchiolitis. Oral amoxicillin is for bacterial pneumonia. The respiratory rate of 58/min meets the fast-breathing threshold for age (≥50/min for 2–12 months), but in the context of bilateral wheeze and barrel chest, the overall syndrome is bronchiolitis, not bacterial pneumonia.
Diagnosis and IMNCI Classification
The clinical diagnosis and severity classification of paediatric pneumonia is built on the WHO IMNCI framework, which uses two cardinal signs — fast breathing and chest indrawing — that can be assessed without special equipment. These two signs were chosen because they are reproducible even without a stethoscope, can be taught to community health workers, and have been validated in large studies across low-resource settings in South Asia and sub-Saharan Africa. They anchor the severity tiers that determine the entire management pathway: the setting of care (home vs hospital), the route of antibiotic delivery (oral vs parenteral), and the urgency of referral. Recognising each sign correctly — especially distinguishing lower chest-wall indrawing from intercostal recession — is a clinical skill that must be practised on real patients and not left to description alone.
Provided image
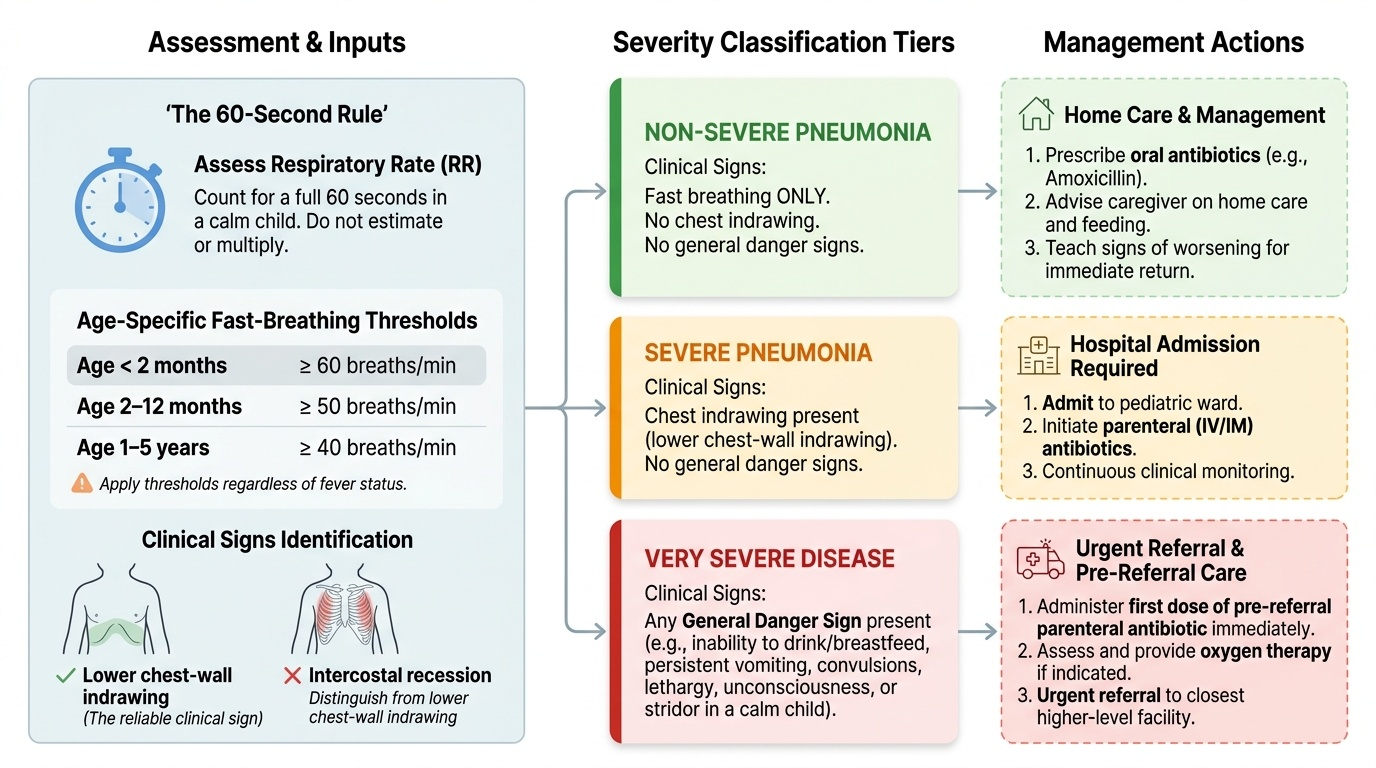
WHO IMNCI fast-breathing thresholds (age-specific — memorise precisely):
• Children under 2 months: respiratory rate ≥60 breaths per minute
• Children 2–12 months: respiratory rate ≥50 breaths per minute
• Children 1–5 years: respiratory rate ≥40 breaths per minute
These thresholds reflect the physiological baseline respiratory rates for each age group; a rate at or above the threshold signals lower respiratory involvement. The respiratory rate should be counted for a full 60 seconds in a calm child, not estimated — even 10 seconds multiplied by 6 introduces error. In children with fever, tachypnoea may be partially explained by the elevated temperature, but the IMNCI threshold is applied regardless.
Severity classification:
• Non-severe pneumonia (cough/cold with fast breathing only): The child is breathing fast for age, but there is no chest indrawing and no danger signs. This child can be managed at home with oral antibiotics and safety-net advice to return immediately if condition worsens.
• Severe pneumonia (fast breathing + lower chest-wall indrawing): Chest indrawing is defined as the lower chest wall drawing inward on inspiration. This sign indicates that the child is making forceful inspiratory efforts against increased airway resistance or reduced lung compliance. Chest indrawing mandates hospital admission and parenteral antibiotics.
• Very severe pneumonia / general danger signs: Any of the following require urgent referral to a higher centre — unable to drink or breastfeed, persistent vomiting, convulsions, lethargy or unconsciousness, stridor in a calm child, or severe acute malnutrition.
Investigations:
Chest X-ray is the key imaging investigation. Lobar or segmental consolidation confirms bacterial pneumonia. Bilateral perihilar haziness suggests viral pneumonitis. An air-fluid level or opacified hemithorax suggests empyema. Hyperinflation with flattened diaphragms is the hallmark of bronchiolitis.
Blood investigations: White blood cell count and differential (neutrophilia in bacterial infection, lymphocytosis in viral); C-reactive protein; blood culture (mandatory in severe/very severe cases before starting antibiotics — do not delay treatment for this). Pulse oximetry is essential: SpO2 less than 92% on room air indicates hypoxia and the need for supplemental oxygen.
Pleural fluid analysis in suspected empyema: pH <7.2, glucose <40 mg/dL, LDH >1000 IU/L, or frank pus on aspiration — all indicate a need for drainage. Ultrasound is the investigation of choice for confirming and localising pleural collections.
CLINICAL PEARL
Chest indrawing in a child with pneumonia is a critical severity marker that mandates admission — do not be reassured by the absence of cyanosis. Cyanosis is a late and unreliable sign of hypoxia in children. Measure the SpO2 with a pulse oximeter and watch for chest indrawing as your primary severity markers. Additionally, remember that the IMNCI thresholds are different from normal adult fast-breathing definitions — a respiratory rate of 45/min that is normal in a calm adult is fast-breathing in a 3-year-old. Age-appropriateness is the key.