Page 25 of 34
PE26.{10-15,17} | Hemato-Oncology Examination and Investigations — SDL Guide
Learning Objectives
- Perform a systematic abdominal examination in a child to detect and measure hepatomegaly and splenomegaly
- Interpret a complete blood count (CBC) including RBC indices, reticulocyte count, and coagulation profile using age-appropriate reference ranges
- Prepare and systematically interpret a peripheral blood smear, identifying microcytic, macrocytic, and morphologically abnormal red cells (spherocytes, sickle cells, target cells, blasts, hypersegmented neutrophils)
- Explain the clinical indications for haemoglobin electrophoresis and interpret the resulting HbA, HbA2, HbF, and HbS band pattern
- Demonstrate bone marrow aspiration technique on a manikin, selecting the correct site by patient age and listing key aftercare steps
- Apply referral criteria for haematological conditions in the Indian paediatric setting
- Enumerate the indications for splenectomy in children and describe the essential post-splenectomy precautions
INSTRUCTIONS
Haematological disorders — anaemia, thalassaemia, leukaemia, haemophilia, and ITP — collectively represent one of the highest-burden disease categories in Indian children. Yet diagnosis at the primary-care level hinges entirely on a doctor's ability to find organomegaly on abdominal examination and to read a peripheral smear and a CBC correctly. This module trains the core investigative skill-set: examination, smear morphology, CBC interpretation, haemoglobin electrophoresis, bone marrow aspiration, and the clinical judgements around referral and splenectomy. These competencies appear repeatedly in CBME milestones and in postgraduate entrance examinations.
References
- Ghai Essential Pediatrics, 9th ed., Ch 14 (Haematology) & Ch 15 (Oncology) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Part XIX (Diseases of the Blood) (textbook)
- IAP Guidelines for Management of Iron Deficiency Anaemia and Thalassaemia Major, 2022 (guideline)
- WHO Haemoglobin Thresholds for Anaemia Diagnosis, 2011 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Riya, a 6-year-old girl from a rural district in Karnataka, is brought to the outpatient clinic by her mother, who reports that the child has been looking pale and tired for the past three months and has had two episodes of fever in the last fortnight. On inspection you notice marked pallor of the conjunctivae and a noticeably protuberant abdomen. When you place your hand gently on her left flank and percuss, the dullness extends well below the costal margin — you suspect massive splenomegaly. The nurse hands you the CBC report: haemoglobin 5.8 g/dL, MCV 62 fL, MCH 18 pg, TLC 78,000/µL with 35% blast cells. The peripheral smear shows a population of immature cells with large nuclei and scanty cytoplasm. Your next steps — ordering a haemoglobin electrophoresis, preparing a bone marrow aspiration on the manikin, recognising that this child needs urgent tertiary referral — depend entirely on the haematological skill-set you will build in this module.
WHY THIS MATTERS
Anaemia affects an estimated 53% of Indian children under five years of age (NFHS-5, 2019–21), making it the single most prevalent paediatric nutritional disorder in the country. Beyond iron deficiency, thalassaemia major affects approximately 10,000–12,000 newly affected births per year in India, and acute leukaemia accounts for roughly 30% of all childhood cancers seen at tertiary centres. The paediatrician at the primary or secondary level is the first point of contact for all these children — and the clinical examination finding of hepatosplenomegaly, combined with a correctly read peripheral smear, is often the pivotal observation that determines whether a child receives timely curative therapy or is lost to late diagnosis. NMC CBME competencies PE26.10–26.17 are therefore among the highest-impact skill competencies in the haematology-oncology cluster: they translate directly into saved lives.
RECALL
Before proceeding, consolidate the following prior knowledge from your Year-1 physiology and biochemistry courses:
- Haematopoiesis — in the fetus, the spleen and liver are haematopoietic organs; postnatally, active haematopoiesis shifts to the red marrow of flat bones and vertebrae. Extramedullary haematopoiesis is reactivated in conditions of chronic marrow stress (e.g., thalassaemia major), explaining the massive hepatosplenomegaly that is characteristic.
- Red cell lifespan and indices — normal RBC survives ~120 days; MCV (mean corpuscular volume) reflects cell size, MCH (mean corpuscular haemoglobin) reflects haemoglobin content per cell, MCHC (mean corpuscular haemoglobin concentration) reflects the concentration in the cell; RDW (red cell distribution width) quantifies the anisocytosis (variation in size).
- Haemoglobin structure — adult haemoglobin (HbA) is α₂β₂; foetal haemoglobin (HbF) is α₂γ₂ and has higher oxygen affinity. HbA2 (α₂δ₂) constitutes ~2–3.5% in normal adults. Mutations in β-globin gene produce HbS (sickle cell disease) and β-thalassaemia.
- Spleen anatomy — located in the left hypochondrium under ribs IX–XI; the normal paediatric spleen is not palpable; it becomes palpable at 1 cm below the left costal margin only when enlarged ~1.5–2× its normal size.
Clinical Indication and Relevance: Why Haematological Skills Matter in Paediatric Practice
Haematological disease in Indian children presents across a wide spectrum — from the commonplace iron deficiency anaemia (IDA) of the toddler age group to the haematological emergencies of acute leukaemia and severe thalassaemia crises. The paediatrician's skill in abdominal examination for organomegaly is the entry point: both thalassaemia major and chronic haemolytic anaemias produce progressive enlargement of the spleen (and often the liver) because of trapping of abnormal red cells and extramedullary haematopoiesis, while leukaemia infiltrates these organs with malignant cells. Detecting and correctly quantifying the size of the spleen and liver is therefore not merely an examination technique — it is the physical sign that most often triggers the appropriate investigative workup.
Parallel to examination, the ability to interpret a CBC and peripheral smear is the single most cost-effective diagnostic skill in resource-limited settings: a Leishman-stained peripheral smear costing a few rupees can differentiate IDA (microcytic, hypochromic, pencil cells) from megaloblastic anaemia (macrocytic, hypersegmented neutrophils) from thalassaemia (target cells, nucleated RBCs) from acute leukaemia (blasts) — all of which require entirely different management pathways.
The higher-level skills — haemoglobin electrophoresis interpretation, bone marrow aspiration, referral decisions, and splenectomy indications — represent the next tier of competence that a final-year student must be able to apply at the secondary-care level and recognise when to escalate.
- Haematological disease accounts for ~25–30% of all paediatric outpatient visits in India (Ghai, Ch 14)
- CBME milestones PE26.10–PE26.17 span the full diagnostic skill arc from bedside examination to subspecialty referral
- Early referral of leukaemia and thalassaemia major correlates directly with improved event-free survival
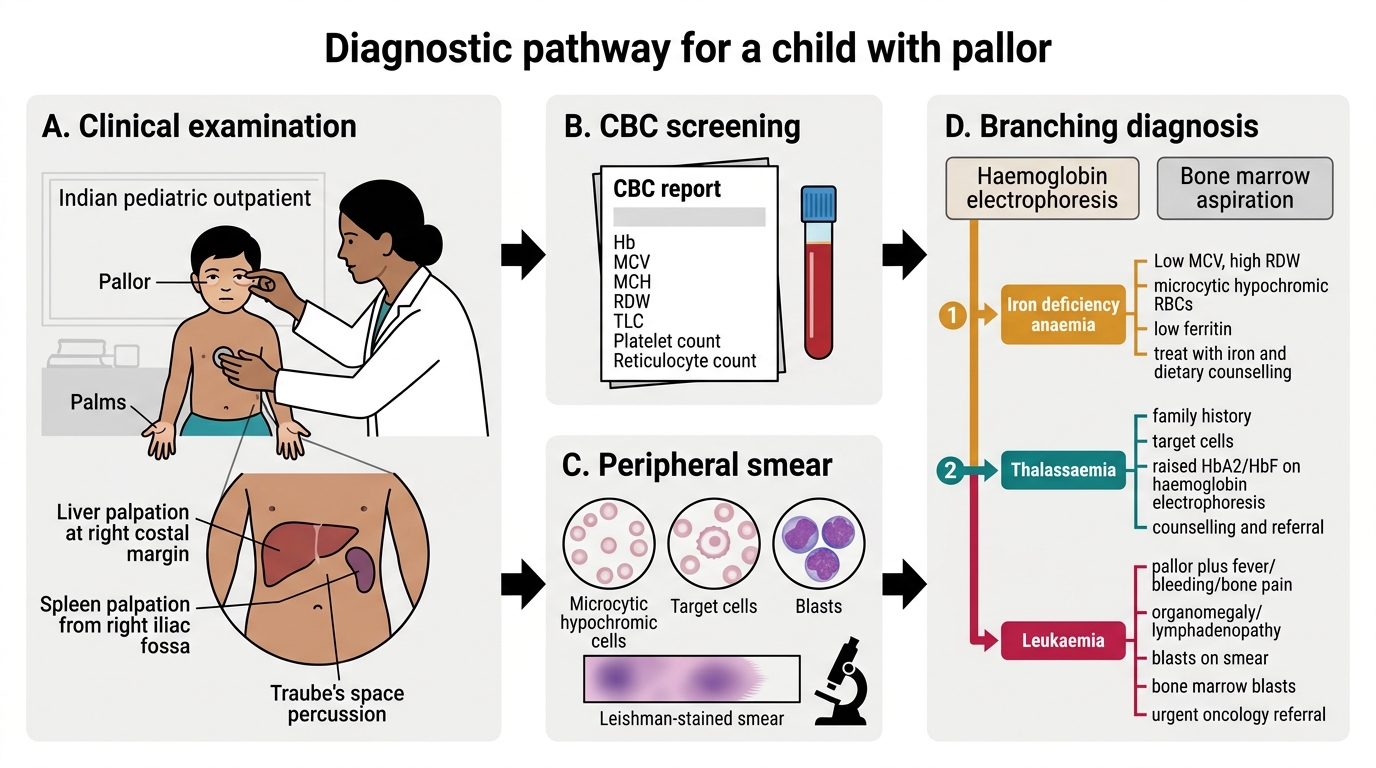
Diagnostic Pathway for Childhood Pallor
Anatomy and Governing Principles: The Haematopoietic System and Examination Foundations
Understanding the anatomical positions and physical boundaries of the liver and spleen is indispensable for accurate organomegaly examination. The liver occupies the right hypochondrium and extends into the epigastrium; its lower border normally lies along the right costal margin in children, and it may descend 1–2 cm below the margin in neonates and infants without being pathologically enlarged. The spleen lies obliquely in the left hypochondrium, with its long axis along the 10th rib; because it is protected by the lower ribs, it must enlarge significantly before becoming palpable. Traube's space — the left lower chest triangle bounded by the 6th rib superiorly, the left midaxillary line laterally, and the left costal margin inferiorly — is normally tympanitic on percussion; obliteration of Traube's space (dullness replacing tympany) is an early sign of splenomegaly and should always be elicited before palpation.
For the peripheral smear, the governing principle is the preparation of a thin, even film with a feathered edge, Leishman-stained to allow identification of red cell morphology, white cell differential, and platelet estimate. The smear must be read systematically — low power (10×) to survey the feathered-edge area, high power (40×) for detailed morphology, and oil-immersion (100×) for nuclear details of blasts or malarial parasites. The correct counting zone is where cells are single-layered and not overlapping, typically ~2/3 of the way from the thick end toward the feathered edge.
For bone marrow aspiration (BMA), the key anatomical principle is site selection by age: the posterior superior iliac spine (PSIS) is the preferred site in children over 18 months and in adolescents, because the bone is superficial, flat, accessible, and carries minimal risk of visceral injury. In neonates and infants under 18 months, the anterior tibial plateau (medial surface, 1–2 cm below the tibial tuberosity) is preferred. The iliac crest and sternum (used in adults) are avoided in young children.
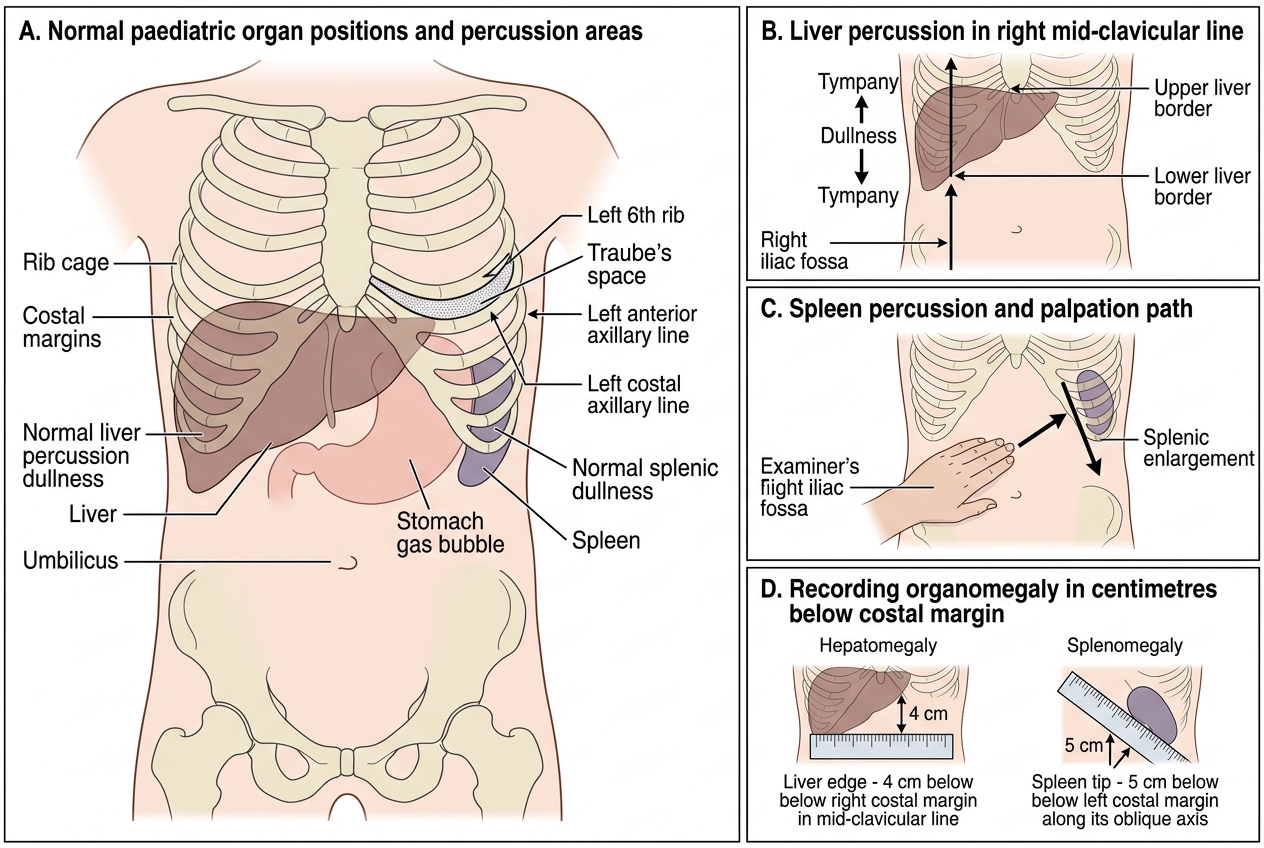
Paediatric Liver and Spleen Examination Landmarks
Procedure and Technique: Abdominal Examination for Organomegaly
A systematic abdominal examination for organomegaly in a child follows a strict sequence that maximises sensitivity while remaining comfortable for the patient. The child should be positioned supine with the knees slightly flexed to relax the abdominal muscles; a crying, tense child will resist palpation and mask a moderately enlarged spleen. Warm your hands before beginning — cold hands provoke voluntary muscle guarding that can simulate a rigid abdomen and hide deep organs. Begin with a careful inspection of the entire abdomen: note the contour, symmetry, visible veins, and any asymmetric fullness in the flanks. A visibly distended left flank with a medially displaced umbilicus is already a sign of massive splenomegaly and should raise your clinical suspicion before you have even placed your hand on the child. The order of examination — inspection → auscultation → percussion → palpation — is maintained in paediatric practice, but for organomegaly detection the most critical steps are percussion (to delineate organ borders and assess Traube's space) before palpation.
Examination of the liver:
1. Start percussion from the right iliac fossa, moving superiorly along the right mid-clavicular line to define the lower border of liver dullness.
2. Confirm with bimanual palpation — place the left hand flat under the right flank, and use the right hand with fingers pointing toward the costal margin, advancing from the right iliac fossa upward in the direction of liver movement with each breath.
3. The lower edge should be described in centimetres below the right costal margin (RCM) in the mid-clavicular line. Normal: ≤1–2 cm below RCM in infants; not palpable in older children.
4. Note the consistency (soft, firm, hard), surface (smooth, nodular), and tenderness.
Examination of the spleen:
1. Begin with percussion of Traube's space — obliteration of tympany indicates splenomegaly before the organ is palpable.
2. Start palpation from the right iliac fossa, moving toward the left costal margin diagonally (toward the left shoulder), advancing with each inspiration.
3. Ask the child to take a deep breath — the spleen descends with inspiration and meets your advancing fingers.
4. Never start palpation from the left costal margin — a massive spleen will be missed if you begin too close.
5. Measure the distance from the left costal margin to the tip in centimetres — use the Hackett grading for splenomegaly: Grade 0 (not palpable), I (<costal margin to umbilicus line), II (reaches umbilicus), III (below umbilicus), IV (into pelvis), V (massive, crosses midline).
Documenting findings: always record size in centimetres below the costal margin rather than simply 'hepatomegaly' or 'splenomegaly', as size guides differential diagnosis (massive splenomegaly >10 cm is most consistent with thalassaemia, chronic malarial spleen, or portal hypertension in Indian children) and tracks response to treatment.
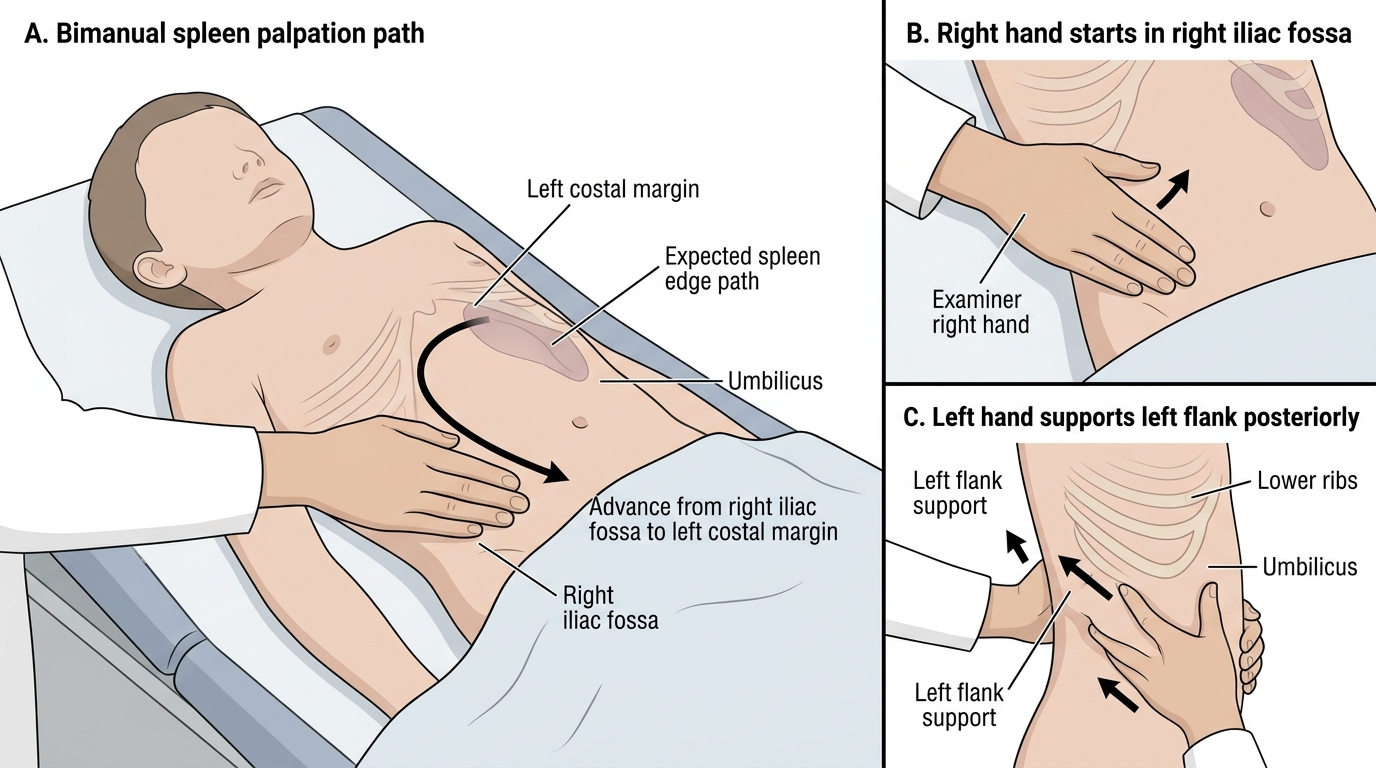
Bimanual Palpation of the Spleen in a Child