Page 14 of 34
PE26.6 | Idiopathic Thrombocytopenic Purpura — SDL Guide (Part 2)
Management of ITP
Management of ITP in children is guided by the severity of bleeding rather than the platelet count alone — many children with platelet counts as low as 10,000–20,000/µL have only minor skin bleeding and are at low risk of major haemorrhage. The fundamental principle is to stratify by clinical severity and treat accordingly, because the majority of childhood ITP resolves spontaneously within 6–12 months regardless of treatment.
Provided image
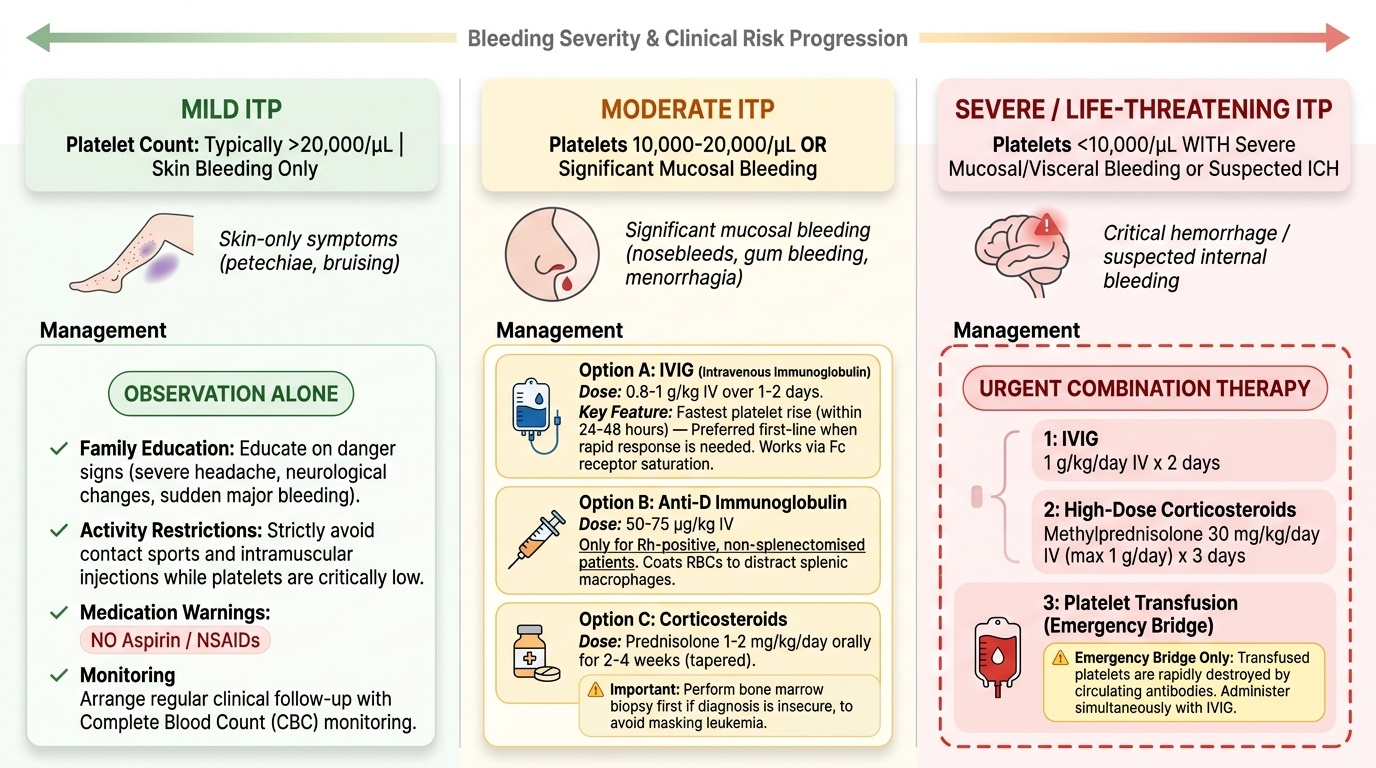
Mild ITP (skin bleeding only, platelet count typically >20,000/µL): Observation alone is appropriate. The family is educated on danger signs (headache, neurological symptoms, excessive bleeding from any site) and advised to avoid contact sports and intramuscular injections while platelet counts are very low. Aspirin and NSAIDs must be strictly avoided as they impair platelet function and can worsen bleeding. Follow-up with CBC monitoring is arranged.
Moderate ITP (significant mucosal bleeding — gum, epistaxis, menorrhagia — or platelet <10,000–20,000/µL with any bleeding): Treatment options include:
• IVIG (Intravenous Immunoglobulin): 0.8–1 g/kg IV over 1–2 days. Mechanism: saturates Fc receptors on splenic macrophages, reducing antibody-coated platelet destruction. Produces the fastest platelet rise (within 24–48 hours), making it the preferred first-line agent when a rapid response is needed. Suitable for Rh-positive and Rh-negative patients and those who have undergone splenectomy.
• Anti-D immunoglobulin: 50–75 µg/kg IV. Works only in Rh-positive, non-splenectomised patients — it coats Rh+ red cells, distracting splenic macrophages from platelet destruction. Cannot be used in Rh-negative children or after splenectomy.
• Corticosteroids: Prednisolone 1–2 mg/kg/day orally for 2–4 weeks (tapered). Important caveat: a bone marrow biopsy should be performed before steroids if the diagnosis is not secure, as steroids can mask leukaemia.
Severe/life-threatening ITP (platelet <10,000/µL with significant mucosal/visceral bleeding or suspected ICH): IVIG (1 g/kg/day × 2 days) combined with high-dose methylprednisolone (30 mg/kg/day IV, max 1 g/day × 3 days) is initiated urgently. Platelet transfusion is reserved for active life-threatening bleeding (e.g., ICH, massive GI haemorrhage) — transfused platelets are rapidly destroyed by circulating antibodies, so they are used only as a temporary bridge, given simultaneously with IVIG. Splenectomy (removal of the major site of platelet destruction and antibody production) is considered for refractory chronic ITP; in children it is deferred as long as possible given the risks of post-splenectomy sepsis.
SELF-CHECK
A 7-year-old Rh-positive girl presents with ITP and gum bleeding. Her platelet count is 12,000/µL. She has not had a splenectomy. Which of the following is an appropriate treatment option SPECIFICALLY limited to Rh-positive, non-splenectomised patients?
A. Intravenous immunoglobulin (IVIG)
B. Prednisolone
C. Anti-D immunoglobulin
D. Platelet transfusion
Reveal Answer
Answer: C. Anti-D immunoglobulin
Anti-D immunoglobulin works by coating Rh-positive red blood cells, which compete with antibody-coated platelets for Fc receptors on splenic macrophages — thereby reducing platelet destruction. This mechanism only works in Rh-positive patients whose spleen is intact (to produce the competitive sequestration). IVIG, prednisolone, and platelet transfusion can all be used regardless of Rh status or splenectomy status.
Self-Assessment
Use the following case to consolidate your learning. Work through each question before reading the answer below.
Case: A 4-year-old boy is brought with sudden-onset petechiae over the trunk and lower limbs. His mother reports a mild cold 3 weeks ago. He is active and afebrile. Examination: multiple non-blanching petechiae, no lymphadenopathy, no hepatosplenomegaly, no pallor. CBC: Hb 11.8 g/dL, WBC 8,200/µL (normal differential), platelets 7,000/µL.
Q1: What is the most likely diagnosis?
Answer: Acute ITP — isolated thrombocytopenia in a well child following a viral illness, with no organomegaly or cytopenias in other lineages.
Q2: Is a bone marrow biopsy required before treatment?
Answer: No — the presentation is typical (well child, post-viral, isolated thrombocytopenia, no organomegaly). Bone marrow biopsy is indicated only if the diagnosis is atypical or if corticosteroids are to be started before confirmation.
Q3: The family asks if you will prescribe steroids immediately. What is the appropriate initial management?
Answer: With platelets at 7,000/µL (severe range), treatment is warranted. IVIG 0.8–1 g/kg IV over 1–2 days is the preferred first-line agent — it acts fastest and does not require bone marrow confirmation. If the child were Rh-positive and spleen-intact, anti-D would also be an option. Platelet transfusion is reserved only if active life-threatening bleeding develops.
Q4: What danger signs should you counsel the family to return immediately for?
Answer: Any headache, vomiting, unusual drowsiness or behavioural change (suggesting ICH); haemorrhage from any mucous membrane not controlled by direct pressure; increasing purpura; passage of blood in stool or urine.
SELF-CHECK
A child with ITP has platelet count of 5,000/µL and is now complaining of severe headache and vomiting. What is the most urgent next step?
A. Oral prednisolone 2 mg/kg and observation
B. Emergency CT brain, IVIG 1 g/kg IV × 2 days + high-dose methylprednisolone, and platelet transfusion if ICH confirmed
C. Anti-D immunoglobulin and discharge home
D. Elective splenectomy referral
Reveal Answer
Answer: B. Emergency CT brain, IVIG 1 g/kg IV × 2 days + high-dose methylprednisolone, and platelet transfusion if ICH confirmed
Headache and vomiting in a child with a platelet count of 5,000/µL should be treated as a possible intracranial haemorrhage (ICH) until proven otherwise — an emergency CT brain is mandatory. Simultaneously, IVIG (1 g/kg/day × 2 days) combined with high-dose methylprednisolone (30 mg/kg/day IV) should be started urgently. Platelet transfusion is given if ICH is confirmed. Oral prednisolone alone is insufficient in this scenario, and discharge or elective procedures are inappropriate.