Page 8 of 34
PE26.3 | Vitamin B12 Folate Deficiency Anaemia — SDL Guide (Part 2)
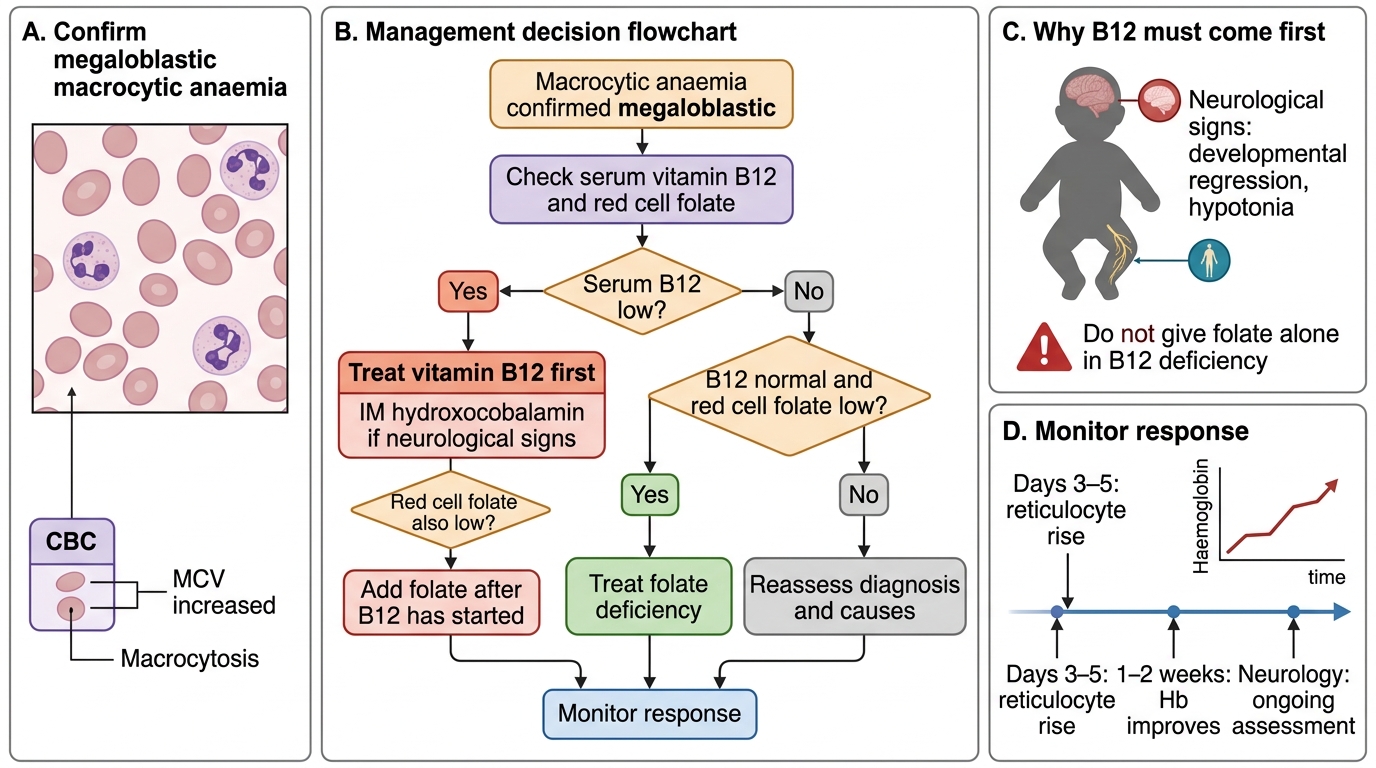
Management: The Critical Rule — B12 Before Folate
The single most important principle in managing megaloblastic anaemia is the B12-before-folate rule: always establish B12 status and treat B12 deficiency before administering folate alone, or concurrently if both deficiencies are present. The rationale for this rule is that folic acid supplementation corrects the haematological picture of megaloblastic anaemia regardless of its cause — a patient with B12 deficiency given folate alone will see a reticulocyte response and rising haemoglobin within 2 weeks. This creates a dangerous clinical trap: the anaemia resolves (and the clinician may believe the diagnosis was folate deficiency), but the underlying B12 deficiency is untreated, and the neurological damage of subacute combined degeneration continues to progress undetected. By the time neurological signs are severe, the window for full recovery may have passed. The rule is operationally simple: check serum B12 before starting folate; if B12 is low or the cause is unclear, start B12 first.
Treatment of vitamin B12 deficiency:
• For dietary deficiency without neurological signs (most common in Indian infants/children): oral high-dose cyanocobalamin or hydroxocobalamin can be effective — doses of 25–100 µg/day orally in infants, or 500–1000 µg/day orally in children (high-dose oral B12 works even in the absence of intrinsic factor because a small fraction is absorbed by passive diffusion)
• For B12 deficiency with neurological signs or in suspected intrinsic factor deficiency: intramuscular hydroxocobalamin preferred — 1000 µg IM on alternate days for 2 weeks, then weekly for 4 weeks, then monthly for life (in intrinsic factor deficiency); for nutritional deficiency in infants, a shorter IM course followed by dietary correction is usually sufficient
• Response: reticulocyte rise within 3–5 days; Hb normalises in 6–8 weeks; neurological improvement begins within weeks but may be incomplete if significant damage has occurred — the single most compelling reason for early diagnosis and treatment
Treatment of folate deficiency:
• Oral folic acid 1–5 mg/day (children: 1 mg/day is standard; 5 mg/day for malabsorption states)
• Continue for 4 months or until the underlying cause is corrected
• In haemolytic anaemias with chronic high folate demand (thalassaemia, sickle cell, hereditary spherocytosis), prophylactic folic acid supplementation is standard practice
• In antiepileptic-drug-related folate deficiency, supplement without stopping the AED; consider switching to a less folate-antagonising drug if anaemia is severe
Dietary sources and prevention:
• B12 is found exclusively in animal-derived foods: meat, fish, eggs, and dairy (including milk and yoghurt). Strict vegans and lacto-vegetarians with minimal dairy have marginal B12 intake. For infants of such mothers, B12 supplementation during pregnancy and lactation (or maternal supplementation with subsequent breast-milk enrichment) is the most effective preventive measure.
• Folate is found in dark green leafy vegetables (spinach, fenugreek, amaranth), legumes, oranges, and fortified cereals. Cooking destroys up to 90% of folate — steaming is preferable to boiling. Goat's milk-fed infants require folate supplementation.
Management of Macrocytic Megaloblastic Anaemia
SELF-CHECK
A 9-month-old exclusively breastfed infant of a vegan mother has megaloblastic anaemia with developmental regression and hypotonia. Serum B12 is 85 pg/mL (low). Serum homocysteine is elevated. What is the CORRECT first step in management?
A. Start oral folic acid 1 mg/day immediately
B. Start oral folic acid and vitamin B12 simultaneously
C. Start vitamin B12 therapy (IM hydroxocobalamin) before any folate
D. Perform bone marrow aspiration to confirm the diagnosis before treating
Reveal Answer
Answer: C. Start vitamin B12 therapy (IM hydroxocobalamin) before any folate
This infant has confirmed B12 deficiency (serum B12 85 pg/mL, <200 pg/mL) with neurological signs (developmental regression, hypotonia) — he needs B12 therapy first. Starting folate first (option A) would correct the CBC while allowing B12 deficiency-related neurological damage to progress silently. Starting both simultaneously (option B) is acceptable in some guidelines, but B12 must be included and started first or concurrently — never folate alone. With confirmed B12 deficiency and neurological involvement, IM hydroxocobalamin is the appropriate route. Bone marrow is not needed when the diagnosis is clear from serum assays.
Self-Assessment
Apply the complete framework from this module to the case below before reading the analysis. Focus on the sequence of investigations and the logic of the treatment decision — these are the skills that are tested in clinical examinations and that you will apply directly at the bedside when managing an infant with macrocytic anaemia and neurological signs.
Case: Kavya, an 8-month-old exclusively breastfed girl, is brought because she has become progressively lethargic and is no longer smiling or reaching for objects as she did at 5 months. Her mother has been vegan for 8 years. Examination: marked pallor, mild jaundice, hypotonia, absent knee and ankle jerks. CBC: Hb 6.5 g/dL, MCV 118 fL, WBC 4.2 × 10⁹/L, platelets 98 × 10⁹/L. Peripheral smear: macro-ovalocytes, one neutrophil with 7 lobes.
Questions:
1. What type of anaemia is this? What mechanism explains the pancytopenia?
2. Which specific investigation confirms the cause is B12 rather than folate deficiency?
3. What is the correct treatment sequence and why does sequence matter?
4. What dietary advice would you give the mother for preventing recurrence in Kavya and any future children?
Analysis:
1. This is megaloblastic anaemia (MCV 118 fL, macro-ovalocytes, hypersegmented neutrophil). Pancytopenia arises because megaloblastic changes affect all marrow cell lines — erythroid, myeloid (producing leucopenia), and megakaryocytic (thrombocytopenia) — as all dividing cells depend on B12/folate for DNA synthesis.
2. Serum B12 will be low (<200 pg/mL). Serum methylmalonic acid (MMA) will be elevated, confirming deficiency of adenosylcobalamin — the B12-specific pathway. Serum homocysteine will also be elevated (but this is non-specific). Red cell folate may be low due to the methylfolate trap (functional folate deficiency secondary to B12 deficiency) — this does NOT mean primary folate deficiency; the primary diagnosis is B12 deficiency.
3. Treat B12 first. Give hydroxocobalamin 1000 µg IM on alternate days for 2 weeks, then assess neurological response. Folate may be added after B12 has been confirmed and begun. Sequence matters because: if folate is given first, the CBC normalises but B12 deficiency continues, and Kavya's neurological damage (hypotonia, loss of reflexes, developmental regression) may progress to an irreversible state. The window for neurological recovery is time-sensitive.
4. The mother should supplement with B12 herself during any future breastfeeding (B12 1000 µg/day orally). She should introduce B12-containing complementary foods at 6 months (dairy products if lacto-vegetarian) or use B12-fortified foods. Kavya should continue IM B12 until her serum B12 normalises, then receive oral supplementation. Neurodevelopmental follow-up at 3, 6, and 12 months to monitor for recovery of milestones.