Page 32 of 48
PE27.10 | Cerebral Palsy — SDL Guide (Part 2)
Management: MDT and Functional Outcomes
Management of cerebral palsy is multidisciplinary, goal-oriented, and adapts across the child's developmental stages from infancy through adulthood. The overarching aims are to maximise functional independence (GMFCS-appropriate goals), prevent secondary complications (contractures, hip dislocation, scoliosis), manage comorbidities, and support family coping. Since CP is a permanent condition with no cure, all therapy goals are rehabilitative. The treating team includes the developmental paediatrician, physiotherapist, occupational therapist, speech and language therapist, orthopaedic surgeon, orthotist, neurologist (for epilepsy), ophthalmologist, audiologist, psychologist, and social worker. Family members — particularly parents — are trained as the primary therapy providers in the home environment, which is the most important setting for functional gains.
1. Physiotherapy:
The cornerstone of motor rehabilitation. Goals include improving range of motion, preventing contractures, facilitating gross motor milestones, and optimising GMFCS-appropriate mobility. Techniques include neurodevelopmental therapy (NDT/Bobath), task-specific training, constraint-induced movement therapy (CIMT) for hemiplegia, and aquatic therapy. Physiotherapists also prescribe assistive devices (walkers, standing frames) and advise on home exercise programmes.
2. Occupational therapy (OT):
Addresses fine motor function, hand use, activities of daily living (ADL — feeding, dressing, writing), sensory integration, and cognitive-perceptual skills. OT is particularly critical in hemiplegic CP to develop bimanual coordination and in quadriplegic CP for positioning and adaptive equipment.
3. Speech and language therapy (SLT):
Addresses dysarthria, communication difficulties, and dysphagia (swallowing assessment + texture modification advice). Augmentative and alternative communication (AAC) devices are prescribed for non-verbal children.
4. Spasticity management:
A stepped approach is used depending on severity and functional impact:
• Physiotherapy and stretching: First-line for all grades of spasticity.
• Oral agents: Baclofen (GABA-B agonist — reduces spasticity), diazepam (adjunct for severe spasm), dantrolene (peripheral muscle relaxant) — all weight-based mg/kg dosing in children; never adult fixed doses.
• Botulinum toxin A (BTX-A) injections: For focal, dynamic spasticity (gastrocnemius, iliopsoas, adductors) — repeated every 3–6 months; combined with physiotherapy; evidence-based for improving gait pattern.
• Intrathecal baclofen (ITB) pump: For severe, generalised spasticity or dystonia not responsive to oral agents; implanted programmable pump.
• Selective dorsal rhizotomy (SDR): Neurosurgical procedure for carefully selected children with pure spastic diplegia; cuts sensory rootlets to reduce spasticity.
5. Orthotics and orthopaedic surgery:
Ankle-foot orthoses (AFO) are the most commonly prescribed device — prevent equinus deformity and improve gait in spastic diplegia. Orthopaedic surgery addresses fixed contractures (tendon lengthening — Achilles, hamstrings, hip adductors), hip dislocation surveillance and correction, and scoliosis management.
6. Management of comorbidities:
• Epilepsy: Appropriate anticonvulsant (valproate, carbamazepine, levetiracetam — weight-based dosing).
• Feeding difficulties: Feeding therapy (SLT-led); gastrostomy (PEG) for severe dysphagia with recurrent aspiration.
• Nutritional support: Growth monitoring; modified texture food; supplementation.
• Drooling (sialorrhoea): Anticholinergic (glycopyrrolate), BTX-A to salivary glands.
7. Prognosis (GMFCS-based):
Children at GMFCS I–II typically achieve independent ambulation by school age. GMFCS III children usually achieve community ambulation with aids. GMFCS IV–V require lifelong attendant care. Dyskinetic CP may have better cognitive outcomes than motor classification suggests. CP is associated with increased mortality at extremes of severity.
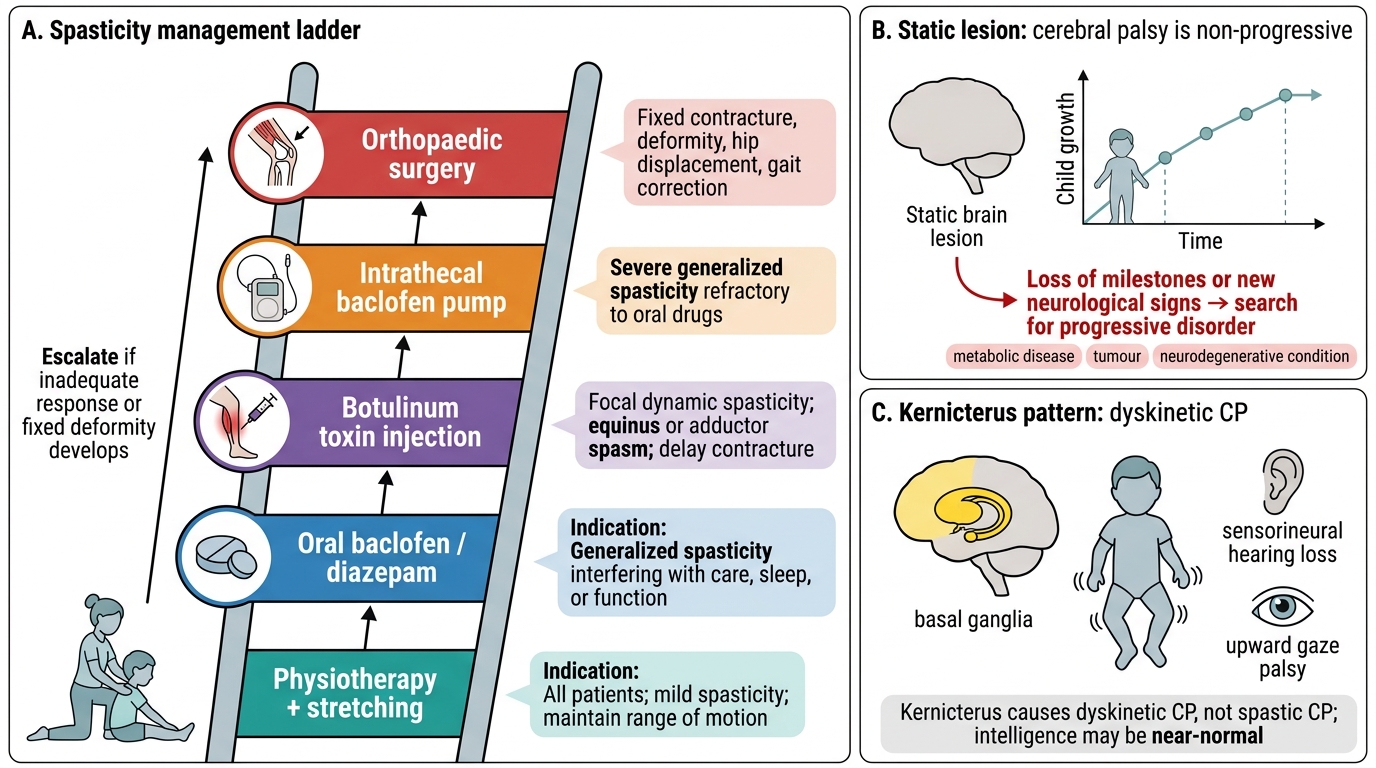
Spasticity Management Ladder in Cerebral Palsy
CLINICAL PEARL
Two critical clinical points about cerebral palsy that are frequently tested and clinically vital: First, CP is NON-PROGRESSIVE — the brain lesion is static and does not worsen over time. If a child diagnosed with CP appears to be deteriorating (losing milestones, new neurological signs), this should prompt a serious search for a PROGRESSIVE neurological disorder (metabolic disease, tumour, neurodegenerative condition) rather than assuming it is CP-related. Second, kernicterus classically produces dyskinetic (choreoathetoid) CP — NOT spastic CP — and is paired with sensorineural hearing loss and upward gaze palsy (the basal ganglia triad). A child with choreoathetosis and high-frequency hearing loss in a setting of neonatal jaundice almost certainly has kernicterus. This distinction matters because children with dyskinetic CP from kernicterus frequently have near-NORMAL intelligence — a prognosis the family needs to understand accurately for educational planning.
SELF-CHECK
A 2-year-old child born at term is brought with writhing, purposeless movements of the limbs that worsen when he tries to reach for objects. Birth history reveals severe neonatal jaundice requiring exchange transfusion. Audiometry reveals bilateral high-frequency sensorineural hearing loss. His intelligence appears age-appropriate. Which type of CP does this child most likely have?
A. Spastic quadriplegia — severe neonatal jaundice always causes quadriplegic CP
B. Dyskinetic (choreoathetoid) CP due to kernicterus — basal ganglia damage from bilirubin
C. Ataxic CP — neonatal jaundice preferentially damages the cerebellum
D. Spastic diplegia — the hearing loss confirms prematurity-related periventricular leukomalacia
Reveal Answer
Answer: B. Dyskinetic (choreoathetoid) CP due to kernicterus — basal ganglia damage from bilirubin
Kernicterus (bilirubin toxicity) preferentially damages the basal ganglia (globus pallidus), cochlear nuclei, and oculomotor nuclei in the neonatal brain. This produces the classic triad: dyskinetic (choreoathetoid) CP (basal ganglia), bilateral high-frequency sensorineural hearing loss (cochlear nuclei), and upward gaze palsy (oculomotor nuclei). Intelligence is often relatively preserved because the cerebral cortex is spared. Spastic quadriplegia results from cortical–subcortical HIE, not kernicterus. Periventricular leukomalacia causes spastic DIPLEGIA in preterm infants.
Self-Assessment: Cerebral Palsy
Use these structured case vignettes to consolidate your understanding of cerebral palsy across the clinical framework: presentation, classification, investigation, and management. Attempt each question independently and check your reasoning against the key concepts listed below. These vignettes reflect the clinical scenarios commonly encountered in paediatric outpatient and ward settings and are representative of examination formats that test applied clinical reasoning about CP diagnosis and management in the Indian paediatric setting.
Case vignette 1: A 2.5-year-old girl born at term with perinatal asphyxia (APGAR 2/5 at 1/5 minutes, required resuscitation) presents with failure to walk. She has bilateral spasticity of all four limbs (worse in legs), brisk reflexes throughout, and bilateral Babinski responses. She makes eye contact but does not speak in words. She has had two generalised tonic-clonic seizures.
Questions:
1. What type of CP does she have? What GMFCS level would you assign initially?
2. Which investigations would you prioritise?
3. List three comorbidities you must screen for.
4. What anticonvulsant would you prescribe (name the drug and state it is weight-based)?
Case vignette 2: A 5-year-old boy with CP walks with a Zimmer frame outdoors but can walk short distances indoors without aids. He attends a mainstream school with educational support.
Questions:
1. What GMFCS level is this child?
2. What does this functional classification imply for his long-term prognosis?
3. What orthopaedic complication should be screened for in a child with spastic CP who is ambulant?
Key concepts checklist:
• CP = non-progressive motor disorder from a static brain lesion in the developing brain.
• Spastic CP (70–80%) = UMN; subtypes: hemiplegia/diplegia/quadriplegia.
• Dyskinetic CP = basal ganglia lesion; kernicterus triad = choreoathetosis + SNHL + upward gaze palsy.
• Ataxic CP = cerebellar lesion; often genetic.
• GMFCS I–V: I = independent ambulation, V = fully dependent — must be assigned for every child.
• Comorbidities: epilepsy (35–40%), ID (~50%), visual/hearing impairment, dysphagia.
• MDT: physio, OT, SLT, neurologist, orthopaedic surgeon, orthotist, psychologist, family.
• Spasticity ladder: physio → oral baclofen/diazepam → BTX-A → ITB pump → SDR/surgery.