Page 40 of 48
PE27.13-14 | CSF Analysis and Lumbar Puncture — SDL Guide
Learning Objectives
- State the clinical indications and contraindications for lumbar puncture in paediatric patients
- Identify the correct intervertebral interspace and patient position for lumbar puncture using surface landmarks
- Describe the step-by-step aseptic technique for lumbar puncture including manometry and specimen collection
- Enumerate the complications of lumbar puncture and outline management of post-LP headache
- Interpret CSF analysis findings — appearance, pressure, cell count, protein, and glucose — for normal, bacterial, viral, tuberculous, and fungal meningitis
- Differentiate a traumatic tap from true subarachnoid haemorrhage using the three-tube method and xanthochromia
INSTRUCTIONS
Lumbar puncture (LP) is a cornerstone diagnostic procedure in paediatric neurology — the CSF obtained can confirm or exclude bacterial meningitis, a condition where a delayed diagnosis can be fatal within hours, and guide empirical antibiotic therapy. Yet LP done at the wrong time, in the wrong patient, can precipitate brain herniation. This module builds both the procedural competence to perform LP safely on a mannequin and the interpretive skill to extract diagnostic meaning from every CSF parameter. By the end you will be able to confidently decide when to proceed, when to defer for imaging, and how to read a CSF report that arrives at the bedside.
References
- Ghai Essential Pediatrics, 9th edition, Ch 17 (Infections of the Nervous System) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 631 (Meningitis) and Ch 642 (Procedures) (textbook)
- IAP Guidelines on Management of Bacterial Meningitis in Children (current edition) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is rushed to the emergency department with a 2-day history of high-grade fever, a severe headache, and vomiting. His mother reports he had two generalised seizures this morning. On examination he is drowsy (GCS 11/15), febrile at 39.8 °C, has a stiff neck, and you can barely flex his chin to his chest. His right pupil appears slightly larger than the left. The resident prepares the LP tray. You pause — should you proceed immediately, or should you obtain a CT head first? The answer to this question, and what you do with the CSF report that follows, can determine whether this child walks out of hospital or does not survive the week.
WHY THIS MATTERS
Bacterial meningitis kills or permanently disables a child within 24 hours if undiagnosed and untreated. CSF analysis obtained via lumbar puncture provides microbiological confirmation that no blood test can replicate — it identifies the organism, its antibiotic sensitivity, and the severity of inflammation. For a final-year MBBS student rotating through paediatrics, LP is one of the handful of bedside procedures you are expected to observe and assist with, and CSF interpretation is a core competency you will exercise in every posting that includes infectious disease, neurology, or emergency medicine. Performing this skill safely on a mannequin — understanding every step including the contraindications — is the NMC expectation behind PE27.14, and interpreting the resulting analysis is the expectation behind PE27.13.
RECALL
Before proceeding, consolidate what you already know from your foundation years:
- Vertebral anatomy (AN): The lumbar spine has five vertebrae (L1-L5). The spinal cord (conus medullaris) ends at the L1-L2 level in adults and at L2-L3 in neonates. Below the conus, the subarachnoid space contains only the cauda equina nerve roots floating in CSF — this is why LP below L2-L3 in adults is safe (you cannot impale the cord). The epidural space lies outside the dura; the subarachnoid space lies inside — LP enters the subarachnoid space.
- CSF physiology (PY): CSF is produced by the choroid plexus (~500 mL/day; total volume ~150 mL). Normal CSF is clear, colourless, with cells <5/mm³ (all lymphocytes), protein 20-45 mg/dL, and glucose approximately two-thirds of the simultaneous blood glucose (ratio ≥0.6). The blood-brain barrier regulates this composition.
- Clinical context (PE): In paediatric practice the most common indications for LP are suspected meningitis and encephalitis. You should already know the classic triad of meningitis — fever, headache, and neck stiffness — and the kernig/brudzinski signs.
When and Why We Perform a Lumbar Puncture
Lumbar puncture is the gold-standard procedure for sampling cerebrospinal fluid from the subarachnoid space, and its primary diagnostic value in paediatrics lies in the evaluation of central nervous system infections. The decision to perform LP must be based on a clear clinical indication, because the information obtained is irreplaceable — no blood culture, no serum marker, and no imaging substitute can tell you whether the organisms in the meninges are Streptococcus pneumoniae (requiring high-dose penicillin) or Mycobacterium tuberculosis (requiring four-drug antitubercular therapy for at least twelve months). Initiating the correct treatment early saves brain, hearing, and life. The clinician who understands both the indications and the contraindications for LP is the clinician who avoids the twin traps of delay (missing the diagnosis) and harm (precipitating herniation in a child with raised intracranial pressure).
Indications for lumbar puncture in paediatric practice include the following:
- Suspected bacterial meningitis — the most urgent indication; CSF culture, Gram stain, cell count, protein, and glucose together confirm the diagnosis and guide therapy.
- Suspected viral meningoencephalitis — CSF lymphocytic pleocytosis with normal glucose distinguishes viral from bacterial meningitis and can prevent unnecessary prolonged antibiotics.
- Suspected tuberculous meningitis — CSF with high protein, low glucose, lymphocytic pleocytosis, and pellicle formation; AFB smear and culture confirm (though culture takes weeks).
- Suspected fungal meningitis — especially in immunocompromised children; India ink stain and cryptococcal antigen (CrAg) test on CSF.
- Subarachnoid haemorrhage (SAH) — when CT is normal but clinical suspicion is high; xanthochromia on spectrophotometry confirms SAH.
- Measurement of CSF pressure — in idiopathic intracranial hypertension (pseudotumour cerebri) where LP both diagnoses and therapeutically reduces pressure.
- Intrathecal drug administration — e.g. methotrexate in ALL, antibiotics in gram-negative ventriculitis (therapeutic LP).
The urgency of LP is greatest in suspected bacterial meningitis — in this setting, if LP is safe to proceed, it should be done before antibiotics so as not to sterilise the CSF and obscure culture results. However, this must never delay antibiotic administration beyond 30-60 minutes in a deteriorating child; in that case, blood cultures are drawn and antibiotics commenced immediately, with LP deferred.
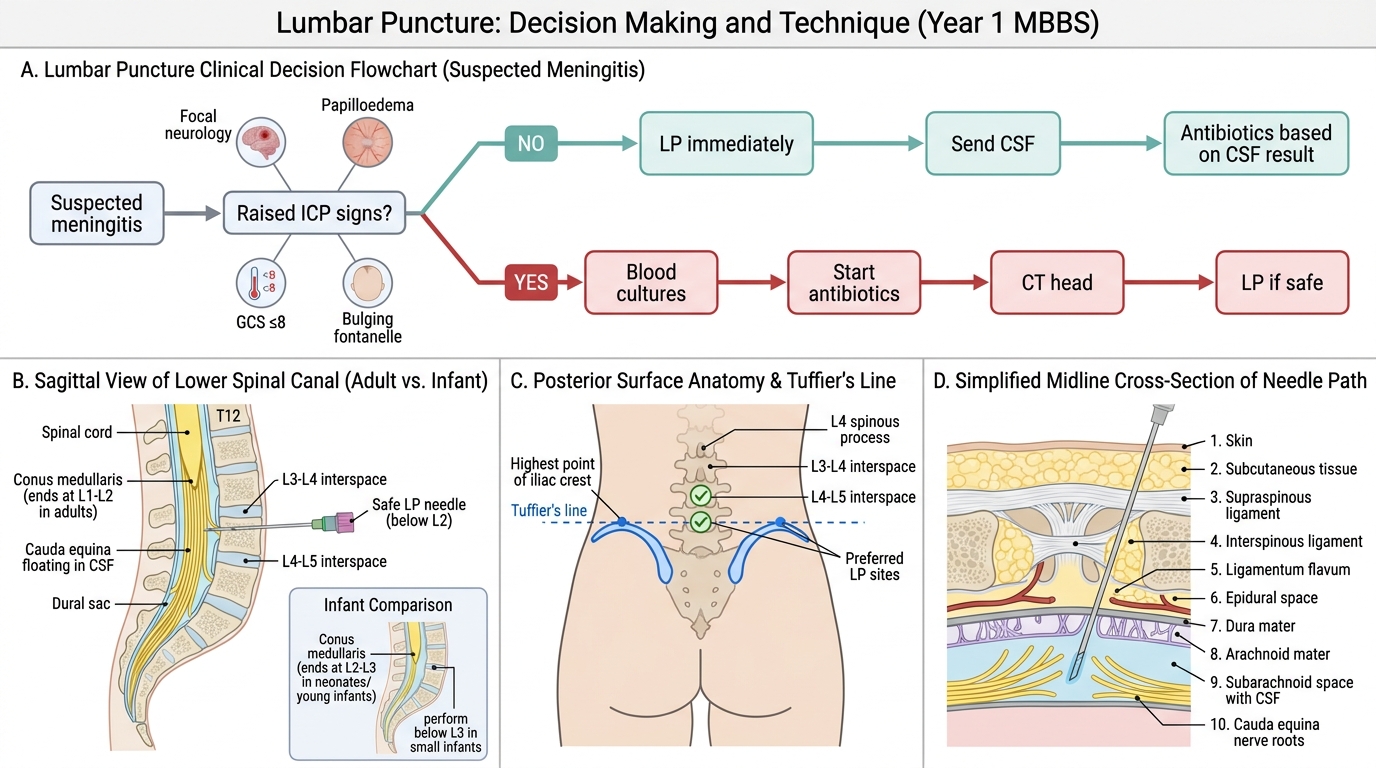
Lumbar Puncture Decision Flow and Safe Anatomy in Suspected Meningitis
Lumbar Anatomy and Governing Principles
The safety of LP depends entirely on understanding the anatomy of the lumbar region and selecting the correct needle entry point. The spinal cord tapers into the conus medullaris, which ends at the level of the L1-L2 intervertebral disc in adults and at L2-L3 in neonates and young infants. Below this level, the neural canal contains only the cauda equina — a collection of lumbar, sacral, and coccygeal nerve roots that float freely in cerebrospinal fluid and are displaced (not punctured) by a needle. This is the anatomical rationale for performing LP below the L2 level in adults and below L3 in small infants.
The chosen interspace is L3-L4 or L4-L5 in older children and adults. To identify L4, draw an imaginary horizontal line connecting the highest points of both posterior superior iliac crests — this Tuffier's line crosses the L4 spinous process (or the L4-L5 interspace). One interspace above is L3-L4. Either is safe in children over approximately 12-18 months of age.
A cross-sectional approach to the structures encountered from skin inward during LP:
1. Skin and subcutaneous tissue
2. Supraspinous ligament (connects spinous process tips)
3. Interspinous ligament (runs between adjacent spinous processes)
4. Ligamentum flavum — the thickest, most elastic layer; a characteristic resistance-then-give is felt as the needle pierces it
5. Epidural space — contains fat and epidural venous plexus; LP targets the space beyond this
6. Dura mater — second resistance felt; piercing it produces another "give"
7. Subdural space (potential; not targeted)
8. Arachnoid mater — closely applied to dura
9. Subarachnoid space — the target; contains CSF and cauda equina roots
Once the needle tip enters the subarachnoid space, stylet withdrawal produces free-flowing, dripping CSF. Resistance, no flow, or haemorrhagic fluid at this step indicates needle repositioning is needed.
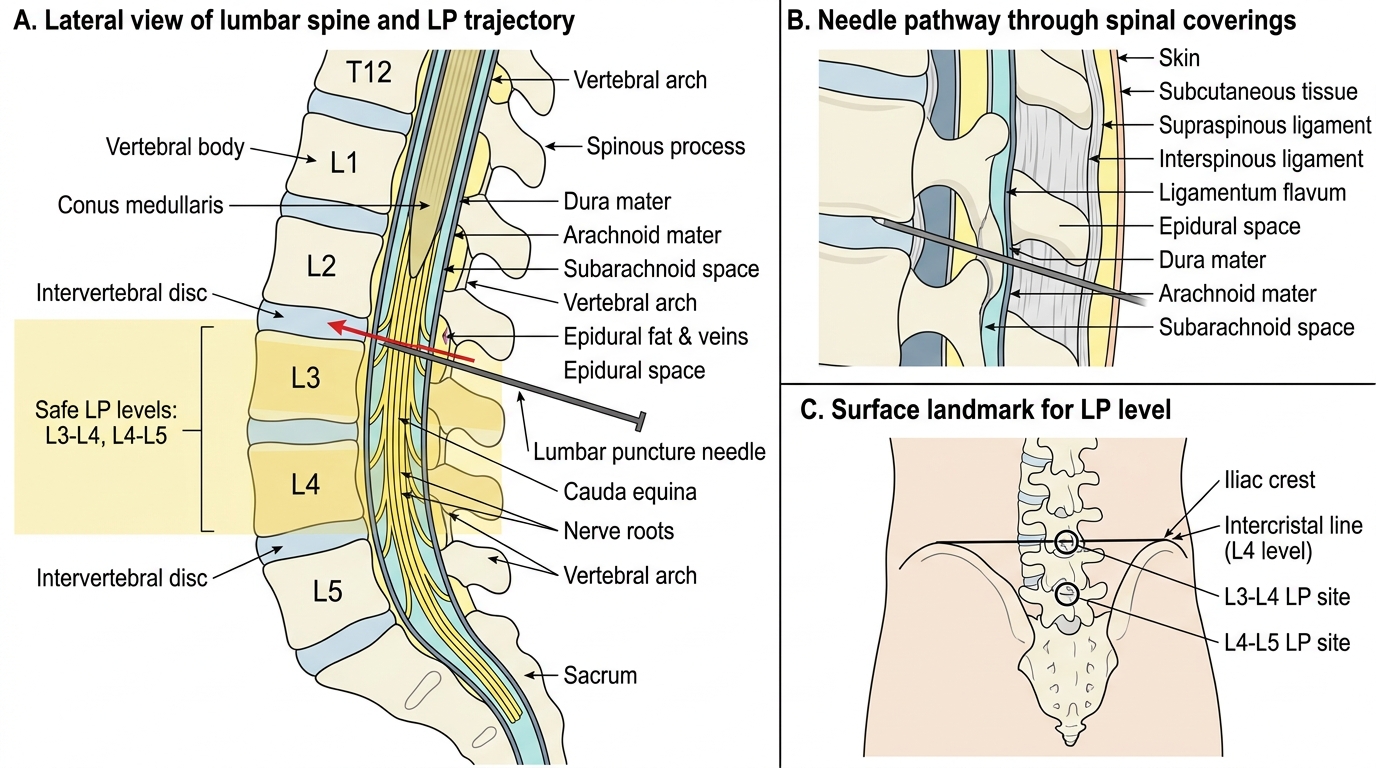
Lumbar Puncture Anatomy in Lateral View
Contraindications to Lumbar Puncture
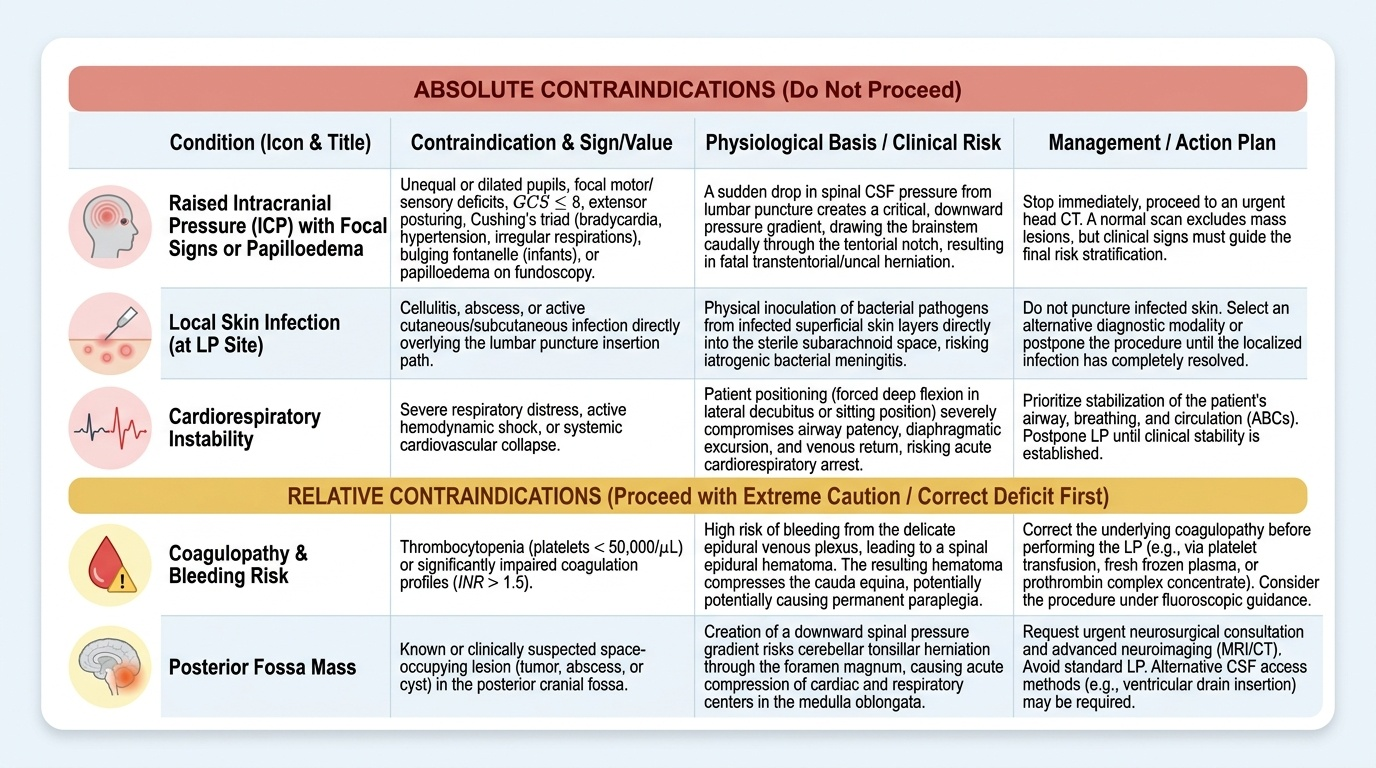
Understanding contraindications is as important as understanding how to perform LP — proceeding in a contraindicated patient can kill them through transtentorial (uncal) herniation, a catastrophic event in which supratentorial pressure suddenly decompresses through the tentorial notch as the LP reduces spinal CSF pressure. Every contraindication flows from a clinical concern about this risk, bleeding risk, or local infection risk. These are not arbitrary rules but consequences of basic pathophysiology: the subarachnoid space communicates freely with the intracranial compartment, and any procedure that reduces spinal CSF pressure creates a pressure gradient that can draw the brainstem caudally through the tentorium in a patient whose brain is already under supranormal pressure. Recognising the warning signs before picking up the needle is therefore a life-saving clinical skill in its own right, and one that the NMC explicitly expects you to be able to discuss (PE27.14 — "discuss the contraindications").
Provided image
Absolute contraindications:
- Signs of raised intracranial pressure with focal neurology or papilloedema. These include: unequal pupils or pupillary dilatation (III nerve compression from uncal herniation), focal motor/sensory deficit, extensor posturing, Cushing's triad (bradycardia + hypertension + irregular respirations), bulging fontanelle in an infant, papilloedema on fundoscopy, or a GCS ≤8. When any of these signs are present, proceed immediately to CT head before LP. A normal CT does not guarantee absence of raised ICP (the CT findings of raised ICP — effaced sulci, obliterated cisterns — can be subtle), but it excludes a mass lesion and helps stratify the risk.
- Local skin infection or soft tissue infection at the intended puncture site. Introducing the needle through infected tissue risks seeding organisms into the subarachnoid space and creating iatrogenic meningitis.
- Cardiorespiratory instability (haemodynamic shock or severe respiratory distress). The procedure requires the child to be in a flexed position which may compromise an already-stressed airway and cardiovascular system. Stabilise the child first.
Relative contraindications (proceed with caution, specialist guidance, or defer):
- Coagulopathy or thrombocytopenia. A platelet count below 50,000/mm³ or an INR above 1.5 significantly increases the risk of epidural haematoma, which can cause acute paraplegia. Correct the coagulopathy first, or in a critically ill meningitic child, give platelets/FFP before LP. The exact threshold is clinical-judgement-based.
- Posterior fossa mass lesion — even without overt raised ICP signs, a posterior fossa tumour or abscess on CT is a contraindication because the pressure gradient during LP can cause upward or downward herniation of cerebellar tonsils.
Key clinical rule: in any child with suspected meningitis AND signs of raised ICP, do NOT delay antibiotics waiting for CT. Draw blood cultures → start empirical antibiotics → proceed to CT → perform LP only if CT shows no contraindication. The antibiotic should be in the child within 30-60 minutes of clinical recognition of meningitis, regardless of LP status.
SELF-CHECK
A 3-year-old with fever and neck stiffness has a bulging fontanelle and sunset-sign eye deviation. Which is the MOST appropriate immediate next step?
A. Perform lumbar puncture immediately for CSF culture
B. Draw blood cultures, start empirical antibiotics, and arrange urgent CT head
C. Perform fundoscopy only; if no papilloedema, proceed with LP
D. Administer mannitol and defer all further investigations to the ICU
Reveal Answer
Answer: B. Draw blood cultures, start empirical antibiotics, and arrange urgent CT head
A bulging fontanelle and sunset-sign deviation are clinical signs of raised intracranial pressure — absolute contraindications to immediate LP. However, the child has suspected bacterial meningitis, which must not have antibiotic treatment delayed. The correct sequence is: blood cultures → empirical antibiotics within 30-60 minutes → urgent CT head → LP only if CT does not show contraindication. Option A risks herniation. Option C is insufficient — a bulging fontanelle itself mandates CT regardless of fundoscopy. Option D is premature without antibiotic coverage.