Page 19 of 48
PE27.6 | Febrile Seizures — SDL Guide
Learning Objectives
- Define febrile seizures and describe the classic clinical presentation
- Distinguish simple from complex febrile seizures using precise criteria
- Explain the pathophysiology of febrile seizure generation and identify common precipitating infections
- Outline the acute management and provide evidence-based parental counselling
INSTRUCTIONS
Febrile seizures are the most common convulsive disorder of childhood, affecting 2–5% of all children. A frightened parent rushing to the emergency department with a convulsing child is one of the most anxiety-laden scenarios in paediatric practice. Your ability to rapidly assess severity, reassure appropriately, and avoid unnecessary investigations depends on a firm grasp of the classification and evidence base. This module will equip you to manage febrile seizures confidently and counsel families effectively.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Neurology — Febrile Seizures) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 611 (Febrile Seizures) (textbook)
- IAP Consensus Statement on Febrile Seizures (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An anxious mother rushes into the emergency department carrying her 18-month-old son. "He just shook all over for about a minute and went stiff — I thought he was dying!" The child is now sleepy but responding to his name. He has been febrile since this morning (temperature 39.2°C). There is no neck stiffness, rash, or bulging fontanelle. This is his first such episode. You recognise this as a classic febrile seizure — the most common convulsive disorder in childhood. Your twin tasks are: (1) rapidly determine whether this is a simple or complex febrile seizure, and (2) reassure the mother that her child is very likely to be fine — while remaining alert to the warning signs that would demand further investigation.
WHY THIS MATTERS
Febrile seizures affect 2–5% of all children aged 6 months to 5 years, making them one of the most common neurological presentations in general paediatrics and emergency medicine. As a final-year student and future doctor, you will encounter febrile seizure presentations both in the emergency setting (acute management and investigations) and in the outpatient setting (parental counselling, recurrence risk). The key skill is not just recognition — it is calibrated reassurance backed by evidence. Overinvestigating a simple febrile seizure (unnecessary lumbar puncture, routine EEG, prophylactic anti-epileptics) causes harm without benefit. Underrecognising a complex febrile seizure misses children at higher risk of later epilepsy. Getting the classification right is the hinge of all subsequent management.
RECALL
Before proceeding, recall from Physiology (PY): neuronal excitability depends on the balance between excitatory (glutamate, AMPA/NMDA receptors) and inhibitory (GABA, GABA-A receptors) neurotransmission. A seizure occurs when there is excessive synchronous neuronal discharge — either from increased excitation or reduced inhibition. Recall from paediatrics (Year 2): fever is mediated by endogenous pyrogens (IL-1, IL-6, TNF) acting on the hypothalamus to raise the set-point temperature; febrile illness in children commonly results from viral upper respiratory infections and gastroenteritis. Recall also the developmental paediatric principle: the immature brain has a lower seizure threshold than the adult brain — this is the biological substrate for febrile seizures.
Clinical Presentation of Febrile Seizures
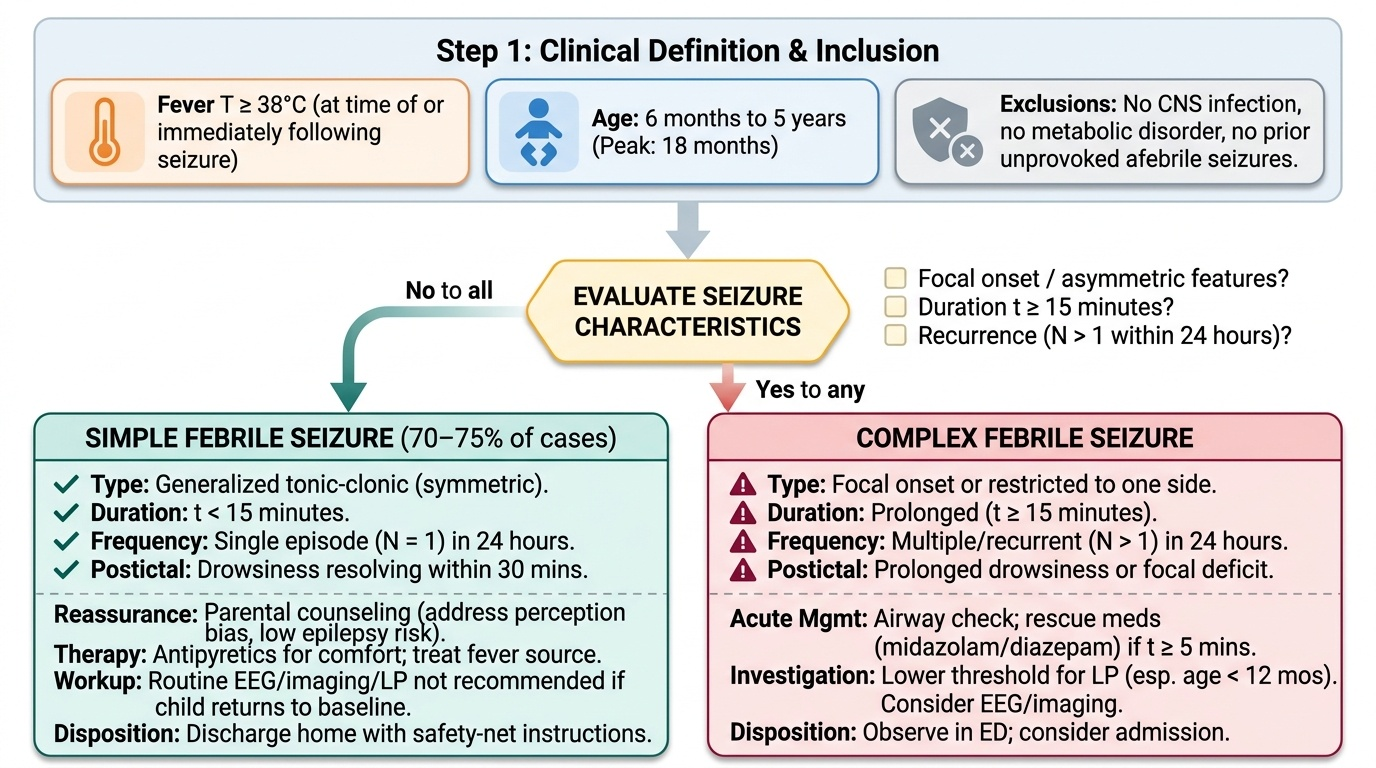
A febrile seizure is defined as a seizure occurring in association with fever (temperature ≥38°C) in a child aged 6 months to 5 years, in the absence of a central nervous system (CNS) infection, metabolic disorder, or prior history of unprovoked afebrile seizures. The key word in this definition is 'association' — the child is febrile at the time of the seizure, but the seizure itself is not caused by the CNS infection. This definition also excludes neonatal seizures (under 6 months, when the diagnosis of febrile seizure cannot be applied) and excludes children with a prior diagnosis of epilepsy, where the fever may simply be a provocation for an already established seizure disorder. The prevalence of febrile seizures in India and globally is approximately 2–5% of children in the target age range — making this one of the highest-volume paediatric neurological diagnoses you will encounter in practice.
Provided image
The classic presentation of a simple febrile seizure — which accounts for approximately 70–75% of all febrile seizures — is highly recognisable:
• The child is typically aged 6 months to 5 years (peak incidence 18 months)
• The seizure is generalised tonic-clonic: initial stiffening of all limbs (tonic phase) followed by rhythmic jerking of all four limbs (clonic phase)
• Duration is less than 15 minutes (usually 1–3 minutes)
• The episode is single within a 24-hour period
• There is a postictal period of drowsiness or confusion lasting minutes to about 30 minutes; the child then returns to baseline
• The fever is usually rising rapidly at the time of seizure onset; the seizure often occurs on the first day of the febrile illness, before the fever is recognised
Parents are typically terrified and describe the episode vividly — the child's eyes rolling back, limbs shaking, possible brief colour change (cyanosis during the tonic phase). They often report that it lasted much longer than it actually did (perception bias during a distressing event).
On examination after the seizure:
• Child is postictal — drowsy but arousable, returning to normal within 30 minutes
• Febrile — temperature ≥38°C
• No meningeal signs (no neck stiffness, no Kernig's sign, no photophobia)
• No focal neurological deficit
• Normal fontanelle (not bulging)
• Source of fever should be identified (otitis media, URTI, pharyngitis, gastroenteritis — HHV-6/roseola infantum is the classic association)
The history distinguishing the seizure as simple or complex is taken immediately on presentation:
1. Was the movement generalised (whole body) or focal (one limb, one side, deviation of eyes/head)?
2. How long did it last — was it less than 15 minutes or prolonged?
3. Was there more than one seizure episode in the last 24 hours?
These three questions determine the simple/complex classification and the subsequent investigation and management pathway.
Pathophysiology and Aetiology
The pathophysiology of febrile seizures reflects the interaction between an immature, developmentally low-threshold brain and the physiological cascade of fever. To understand why seizures occur with fever in young children but almost never in healthy adults, one must appreciate how the developing nervous system differs from the mature brain in its excitatory-inhibitory balance.
The immature brain (6 months to 5 years) has several physiological features that lower seizure threshold compared to the adult brain: GABA-A receptors in the immature cortex mediate excitation rather than inhibition (because of high intracellular chloride — depolarising GABA responses), sodium channels are denser and more easily activated, and myelination of inhibitory interneurons is incomplete. These developmental characteristics mean that even modest perturbations — including fever — can precipitate synchronised neuronal discharge.
How fever triggers seizures:
Fever-associated seizure generation involves multiple mechanisms:
1. Direct temperature effect: neuronal firing rate increases with temperature; at high temperatures, sodium channel inactivation fails, leading to sustained depolarisation and burst firing
2. Cytokine-mediated excitability: IL-1β (the key endogenous pyrogen) also directly enhances NMDA receptor-mediated excitation in hippocampal neurons, increasing seizure susceptibility independent of core temperature elevation
3. Respiratory alkalosis: fever-associated hyperventilation (hyperpnea) reduces PaCO₂, producing cerebral vasoconstriction and neuronal hypersynchrony
4. Genetic predisposition: approximately 25–40% of children with febrile seizures have a first- or second-degree relative with a history of febrile seizures; SCN1A mutations (sodium channel) and GABRG2 mutations (GABA receptor) are identified in some families with febrile seizure-plus (FS+) phenotype
Common aetiological triggers:
• Human Herpesvirus-6 (HHV-6 / roseola infantum) is the most common identifiable viral trigger in infants; the primary HHV-6 infection (roseola infantum) is characterised by 3–5 days of high fever followed by a maculopapular rash as the fever resolves; febrile seizures occur at the height of the fever
• Influenza virus — particularly type A; febrile seizures associated with influenza are often prolonged and may recur within the illness
• Upper respiratory tract infections (rhinovirus, adenovirus, coronavirus)
• Gastroenteritis (rotavirus, especially)
• Otitis media and tonsillitis in toddlers
• Post-immunisation fever: febrile seizures can occur 6–14 days after MMR (due to the vaccine-induced fever); this should be distinguished from vaccine-related adverse events — the seizure mechanism is the same as any febrile seizure and carries the same prognosis
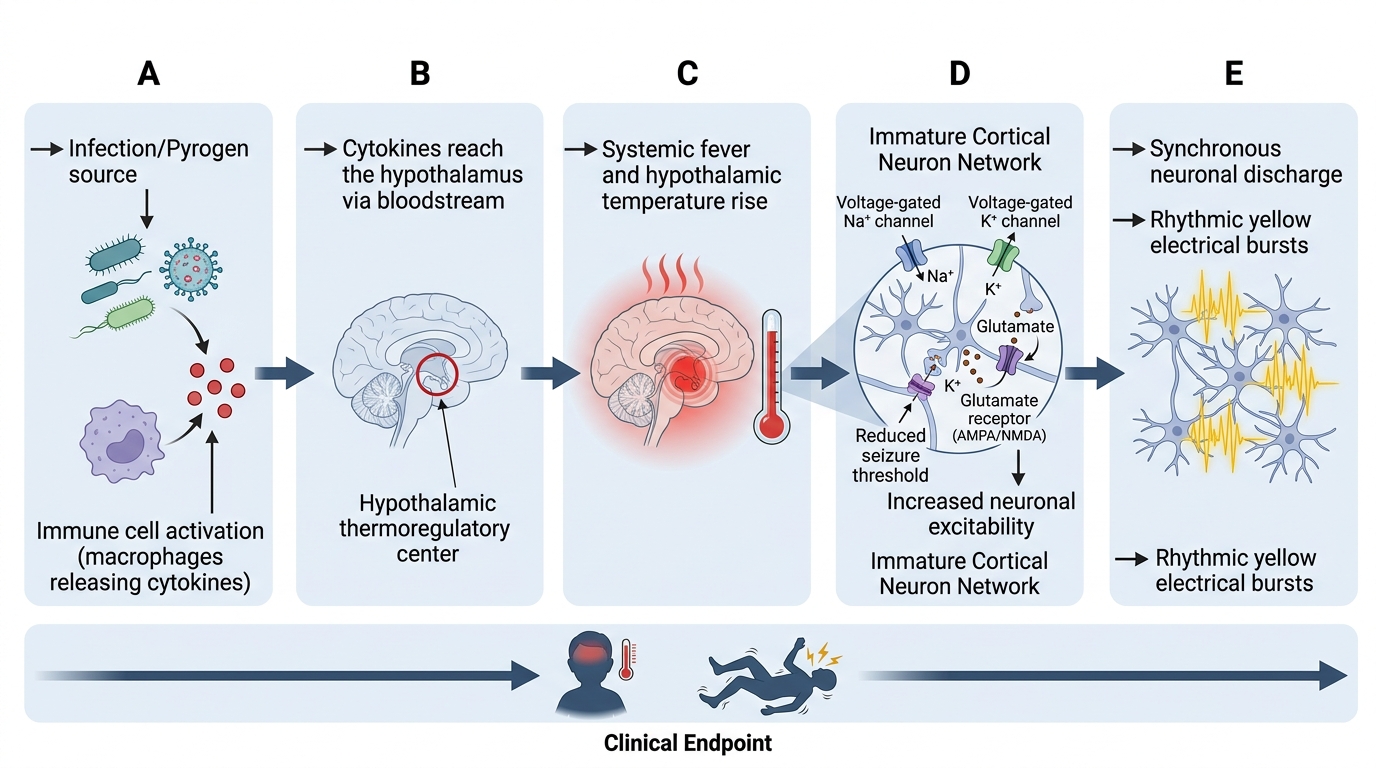
Fever-Induced Lowering of Seizure Threshold in the Immature Brain
Classification: Simple vs Complex Febrile Seizures
The distinction between simple and complex febrile seizures is not merely semantic — it determines the risk of recurrence, the risk of later epilepsy, the need for investigations, and the management approach. The classification is based on three binary questions about seizure character, duration, and frequency within a 24-hour period. Every student must be able to apply these criteria instantly at the bedside, because the classification drives every subsequent decision: whether to perform a lumbar puncture, whether to order an EEG or MRI, whether to prescribe prophylactic medication, and how to counsel the family regarding prognosis. Importantly, a febrile seizure is classified at the time of presentation — you cannot change the classification retrospectively. The three defining features are: generalised versus focal; duration less than versus 15 minutes or more; and single versus recurrent within 24 hours.
A simple febrile seizure must fulfil ALL three of the following criteria:
1. Generalised — synchronised tonic-clonic movements involving both sides of the body simultaneously, with no focal onset and no head or eye deviation
2. Short — duration less than 15 minutes (typically 1–3 minutes; nearly always self-terminates)
3. Single — only one episode within a 24-hour period; no clustering of seizures
A complex febrile seizure is one that meets ANY of the following:
1. Focal onset — unilateral clonic movements, head/eye deviation, focal Todd's paralysis post-ictally, or focal EEG changes
2. Prolonged — duration ≥15 minutes (also qualifies as febrile status epilepticus if ≥30 minutes or if it represents status epilepticus)
3. Recurrent — more than one seizure episode within a 24-hour period
Clinical importance of the distinction:
| Feature | Simple | Complex |
|---|---|---|
| Proportion of all febrile seizures | ~70–75% | ~25–30% |
| Risk of recurrence | ~30–35% | Higher (~50%) |
| Risk of subsequent epilepsy | ~1–2% (close to baseline population) | ~4–10% |
| Indication for LP | Only if meningitis suspected | Higher suspicion warranted |
| Prophylactic AED | NOT recommended | Discuss in selected cases |
| Routine EEG | NOT indicated | Not routine, but more justified |
A febrile seizure longer than 30 minutes (or a cluster totalling >30 min without full recovery) is defined as febrile status epilepticus and requires treatment per the status epilepticus protocol. Prolonged febrile seizures (≥15–30 min) have been associated with hippocampal injury on MRI (FEBSTAT study), and a subset of children with prolonged febrile seizures go on to develop mesial temporal lobe epilepsy — one of the most common drug-resistant epilepsy syndromes. This link, while well-documented in temporal lobe epilepsy surgery series, does not mean that all prolonged febrile seizures cause mesial temporal sclerosis; causation vs shared underlying vulnerability is still debated.