Page 10 of 48
PE27.3 | Meningitis Differentiation — SDL Guide (Part 2)
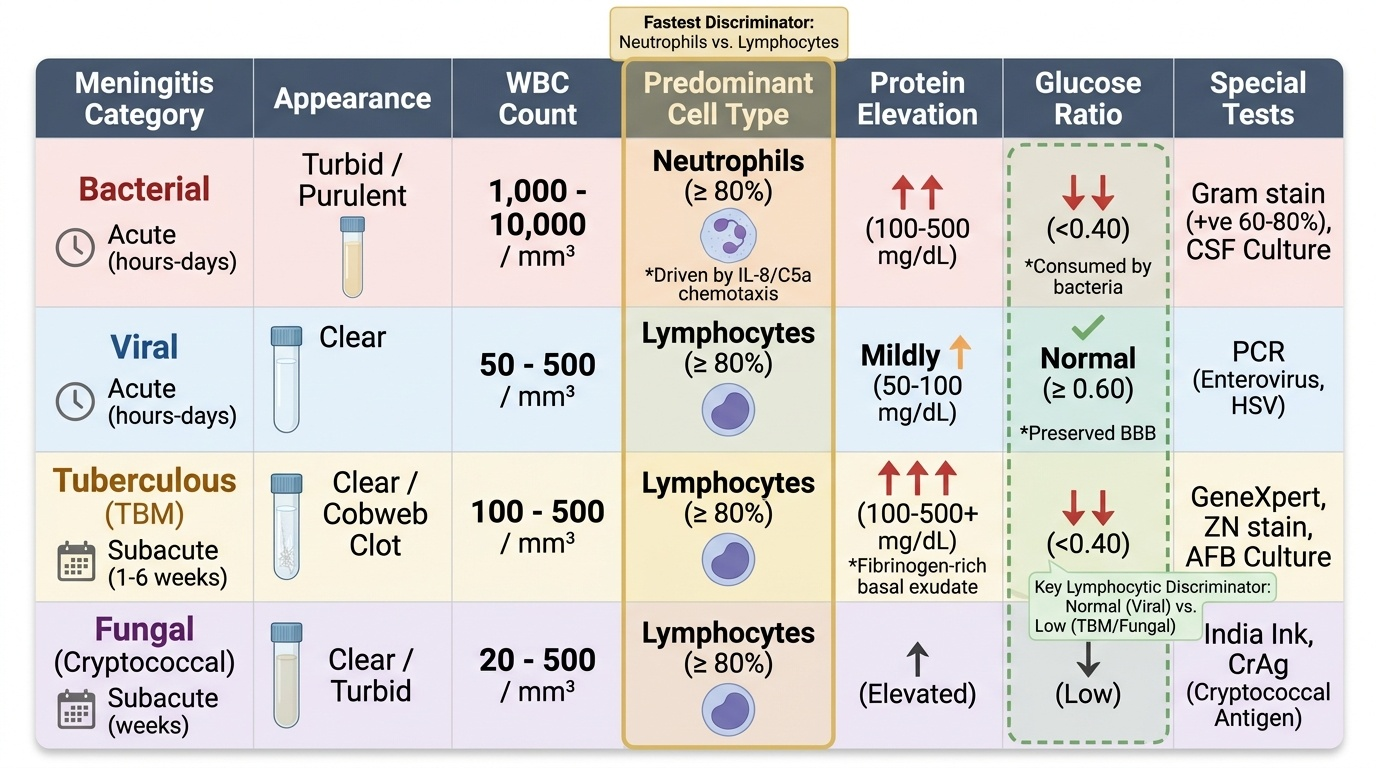
Full Differential Table: Bacterial vs Viral vs TBM vs Fungal
The table below consolidates the CSF profile of each meningitis category into a single reference that integrates all the parameters discussed in the preceding sections. It is perennially one of the highest-yield topics in paediatric neurology finals examinations, but its clinical value goes far beyond examination performance — in the emergency setting, you will refer mentally to this framework within seconds of seeing a CSF report. However, studying the table as an isolated list of numbers is a fragile strategy: numbers are easily mis-remembered under pressure, and atypical cases will not match the columns exactly. The table is most powerful when each entry is anchored to the pathophysiological explanation from the previous section — neutrophils because of IL-8/C5a bacterial chemotaxis; normal viral glucose because of preserved BBB; very high TBM protein because of the fibrinogen-rich basal exudate. With that understanding, the table becomes a predictable consequence of the biology rather than an arbitrary collection of facts.
Provided image
Key points to anchor the table in memory:
• The cell type is the single fastest discriminator: neutrophils = bacterial; lymphocytes = viral/TBM/fungal.
• The glucose is the most important discriminator within the lymphocytic group: normal glucose = viral; low glucose = TBM or fungal.
• The protein elevation is proportional to the severity of BBB breakdown: bacterial < TBM (generally), with fungal variable.
• The appearance and special tests add specificity for organism identification.
| Feature | Bacterial | Viral | TBM | Fungal (Cryptococcal) |
|---|---|---|---|---|
| Appearance | Turbid/purulent | Clear | Clear/faintly turbid (cobweb clot) | Clear/turbid |
| Opening pressure | ↑↑ | Normal/mildly ↑ | ↑ | ↑↑ |
| WBC count | 1,000–10,000/mm³ | 50–500/mm³ | 100–500/mm³ | 20–500/mm³ |
| Cell type | >80% neutrophils | >80% lymphocytes | >80% lymphocytes | >80% lymphocytes |
| Protein | ↑↑ (100–500 mg/dL) | Mildly ↑ (50–100 mg/dL) | ↑↑↑ (100–>500 mg/dL) | ↑ |
| Glucose | ↓↓ (ratio <0.40) | Normal (ratio >0.60) | ↓↓ (ratio <0.40) | ↓ |
| Gram stain | Positive 60–80% | Negative | Negative | Negative |
| Special tests | Culture/sensitivity | PCR (enterovirus/HSV) | GeneXpert, ZN stain, culture | India ink, CrAg |
| Clinical tempo | Acute (hours–days) | Acute (hours–days) | Subacute (1–6 weeks) | Subacute (weeks) |
CLINICAL PEARL
The glucose is the most important single differentiator between viral and TBM: A child with lymphocytic pleocytosis and LOW glucose almost certainly has TBM (or fungal meningitis), NOT viral meningitis. Viral meningitis preserves CSF glucose because the inflammatory response is mild and the BBB disruption is minimal. If a student tells you a case has viral meningitis and the CSF glucose is 18 mg/dL, they are wrong — reassess for TBM. Conversely, lymphocytic pleocytosis with NORMAL glucose in an immunocompetent child (not HIV, not malnourished) favours viral meningitis strongly, provided protein is only mildly elevated. This one rule resolves the majority of clinically difficult cases where the cell type alone would not separate TBM from viral.
Interpretation of Findings: Diagnostic Pitfalls
The standard CSF profiles described above represent fully developed, untreated cases. Clinical practice presents several scenarios where the CSF profile deviates from the classic pattern, and failure to anticipate these pitfalls leads to diagnostic errors. The four most important pitfalls in the paediatric context are described here.
Pitfall 1 — Partially treated bacterial meningitis:
This is the most common diagnostic trap in daily practice. When a child with bacterial meningitis has received one or more doses of antibiotics before the LP is performed, the CSF changes in a predictable direction: the neutrophil count begins to fall and shifts toward lymphocytes; the glucose starts to normalise (bacteria are dying); and the protein may still be elevated. The result is a mixed-cell CSF with borderline glucose and elevated protein that can look like TBM, viral meningitis, or an indeterminate picture. The key distinguishing factor is the clinical tempo: bacterial meningitis is acute (hours to days); TBM is subacute (1–6 weeks). If the child presented acutely with fever and meningism and received antibiotics before the LP, partial treatment must be considered. Always ask specifically about prior antibiotics before interpreting any CSF report.
Pitfall 2 — Early TBM with a neutrophilic shift:
In the very early phase of TBM (first days of CSF infection), the initial inflammatory response may be predominantly neutrophilic before shifting to the characteristic lymphocytic pattern over 24–48 hours. A child with early TBM may therefore have a CSF report showing 60–70% neutrophils, mimicking bacterial meningitis. The clues are the clinical tempo (weeks, not hours), the relatively low total cell count (rarely >1,000 in TBM), the very high protein, and the history of TB contact.
Pitfall 3 — Traumatic lumbar puncture:
If the LP needle traverses an epidural vein, blood contaminates the CSF. This creates spuriously elevated WBC and protein counts. The rule of thumb for correction: subtract 1 WBC per 700 red cells (for normal haematocrit); subtract 1 mg/dL protein per 1,000 red cells. A traumatic tap produces a uniformly blood-tinged CSF that clears from tube 1 to tube 3 (in contrast to subarachnoid haemorrhage where all tubes are equally bloody and xanthochromia develops after 2–4 hours).
Pitfall 4 — Xanthochromia:
Yellow discolouration of CSF indicates previous haemorrhage (RBCs lysed and haemoglobin converted to bilirubin/oxyhaemoglobin), severe hyperbilirubinaemia, or very high protein (>150 mg/dL). It is not a feature of primary meningitis, but very high-protein TBM CSF may appear slightly yellow. Xanthochromia in the context of sudden-onset severe headache = subarachnoid haemorrhage until proven otherwise.
SELF-CHECK
A 3-year-old received amoxicillin for 24 hours before a lumbar puncture. CSF: clear; WBC 300/mm³ (55% lymphocytes, 45% neutrophils); protein 120 mg/dL; glucose 52 mg/dL (serum glucose 90 mg/dL). What is the correct interpretation?
A. Viral meningitis — lymphocyte predominance and near-normal glucose
B. TBM — lymphocyte predominance and elevated protein
C. Partially treated bacterial meningitis — cannot exclude; treat empirically with antibiotics
D. Normal CSF — mild elevation due to traumatic tap
Reveal Answer
Answer: C. Partially treated bacterial meningitis — cannot exclude; treat empirically with antibiotics
This CSF pattern — mixed neutrophilic/lymphocytic pleocytosis with elevated protein and borderline low glucose (ratio 52/90 = 0.58, at the lower boundary of normal) — in a child who received antibiotics before LP is a classic partially treated bacterial meningitis picture. The neutrophilic dominance is diminishing because antibiotics are killing the bacteria, shifting the cell type. The clinical history (acute onset, prior antibiotics) is crucial. The correct action is to treat as bacterial meningitis with ceftriaxone + vancomycin rather than risk under-treating a life-threatening infection. Do not dismiss this as viral on the basis of the lymphocyte shift.
Applied Practice: Worked CSF Scenarios
Apply the five-step interpretation method to each of the three CSF reports below. Work through your reasoning for each step before reading the interpretation. The goal is to practice the method as a habit, not just to arrive at the right answer.
Scenario A:
Child: 8-month-old boy, 1-day history of fever and seizure. No prior antibiotics. BCG scar present, fully vaccinated per NIS.
CSF: turbid; WBC 4,200/mm³ (88% neutrophils); protein 210 mg/dL; glucose 15 mg/dL (serum 85 mg/dL). Gram stain: gram-negative diplococci.
Step 1: Turbid → bacterial. Step 2: 4,200 WBC, 88% neutrophils → bacterial. Step 3: Protein 210 mg/dL → elevated, consistent with bacterial. Step 4: Glucose ratio = 15/85 = 0.18, markedly low → bacterial/TBM. Step 5: Gram-negative diplococci → Neisseria meningitidis.
Interpretation: Bacterial meningitis — meningococcal. Empirical treatment: ceftriaxone + vancomycin. Contact prophylaxis: rifampicin for all close contacts.
Scenario B:
Child: 7-year-old girl, 3-week subacute onset of headache, vomiting, and low-grade fever. TB contact in household (father on ATT).
CSF: clear with cobweb clot; WBC 240/mm³ (88% lymphocytes); protein 380 mg/dL; glucose 20 mg/dL (serum 82 mg/dL). Gram stain negative. GeneXpert: MTB detected.
Step 1: Clear with cobweb clot → TBM. Step 2: 240 WBC, 88% lymphocytes → TBM/viral. Step 3: Protein 380 mg/dL → very high, TBM. Step 4: Glucose ratio = 20/82 = 0.24 → low, excludes viral. Step 5: GeneXpert positive → confirms M. tuberculosis.
Interpretation: TBM (MRC Stage I — alert, no focal deficit at this stage). Start 2HRZE + 10HR (12 months total) + dexamethasone.
Scenario C:
Child: 5-year-old boy, 4-day fever, headache, and vomiting. No TB contact. Fully immunised. Viral illness in the family.
CSF: clear; WBC 180/mm³ (92% lymphocytes); protein 72 mg/dL; glucose 60 mg/dL (serum 88 mg/dL). Gram stain negative. GeneXpert negative.
Step 1: Clear → viral or TBM. Step 2: 180 WBC, 92% lymphocytes → viral/TBM. Step 3: Protein 72 mg/dL → mildly elevated, viral. Step 4: Glucose ratio = 60/88 = 0.68 → NORMAL → viral (excludes TBM and bacterial). Step 5: No organism on stain; consider CSF enterovirus PCR.
Interpretation: Viral (aseptic) meningitis. Supportive care; no antibiotics; monitor closely; discharge when improving.