Page 7 of 20
PE30.5 | Ambiguous Genitalia — SDL Guide
Learning Objectives
- Recognise ambiguous genitalia in a newborn and identify clinical features requiring immediate investigation
- Describe the systematic approach to genital examination in suspected disorders of sex development (DSD)
- State the urgent investigations required and interpret key results (karyotype, 17-OHP, electrolytes)
- Counsel the family appropriately — what to say, what not to say, and how to refer urgently
INSTRUCTIONS
Ambiguous genitalia — the finding that external genitalia cannot be clearly assigned as male or female — is one of the most emotionally charged and medically urgent situations in neonatal paediatrics. It is not simply a surgical or aesthetic issue: the underlying diagnosis may be a life-threatening adrenal crisis. The way you handle this presentation in the first hours — your examination, your communication, your decision to refer — can prevent a fatality, prevent a misassigned sex at birth, and begin an appropriate long-term care pathway. This competency demands both clinical skill and compassionate communication.
References
- Ghai Essential Pediatrics, 9th edition, Ch 17 (Endocrinology) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 594 (Disorders of Sex Development) (textbook)
- ESPE/LWPES Chicago Consensus on DSD Management 2006, updated Lisbon 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 2-day-old baby is brought for the routine neonatal check. As you examine the genitalia, you are uncertain — there is a prominent phallus-like structure, fused labioscrotal folds, and no clearly palpable gonads bilaterally. The parents anxiously ask, 'Is it a boy or a girl?' You pause. Your instinct is to give them an answer immediately to relieve their distress — but you know that the wrong answer given hastily could harm this child for life. Three days later, if you had said 'it's a boy' and sent the family home, this baby might return in florid adrenal crisis. What you do in the next hour matters more than you know.
WHY THIS MATTERS
Ambiguous genitalia affects approximately 1 in 4,500–5,000 newborns. The commonest cause in India is congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency, which — in the classic salt-wasting form — causes a potentially fatal adrenal crisis in the first two weeks of life if not recognised and treated. Beyond the emergency, the long-term stakes are high: incorrect sex assignment at birth causes profound psychological harm to the child and family. Every medical practitioner should be able to recognise ambiguous genitalia, initiate the correct emergency and investigative pathway, counsel the family without assigning sex, and refer to a multidisciplinary DSD team. The skills in this module are also testable in OSCE settings — examine, investigate, counsel, refer.
RECALL
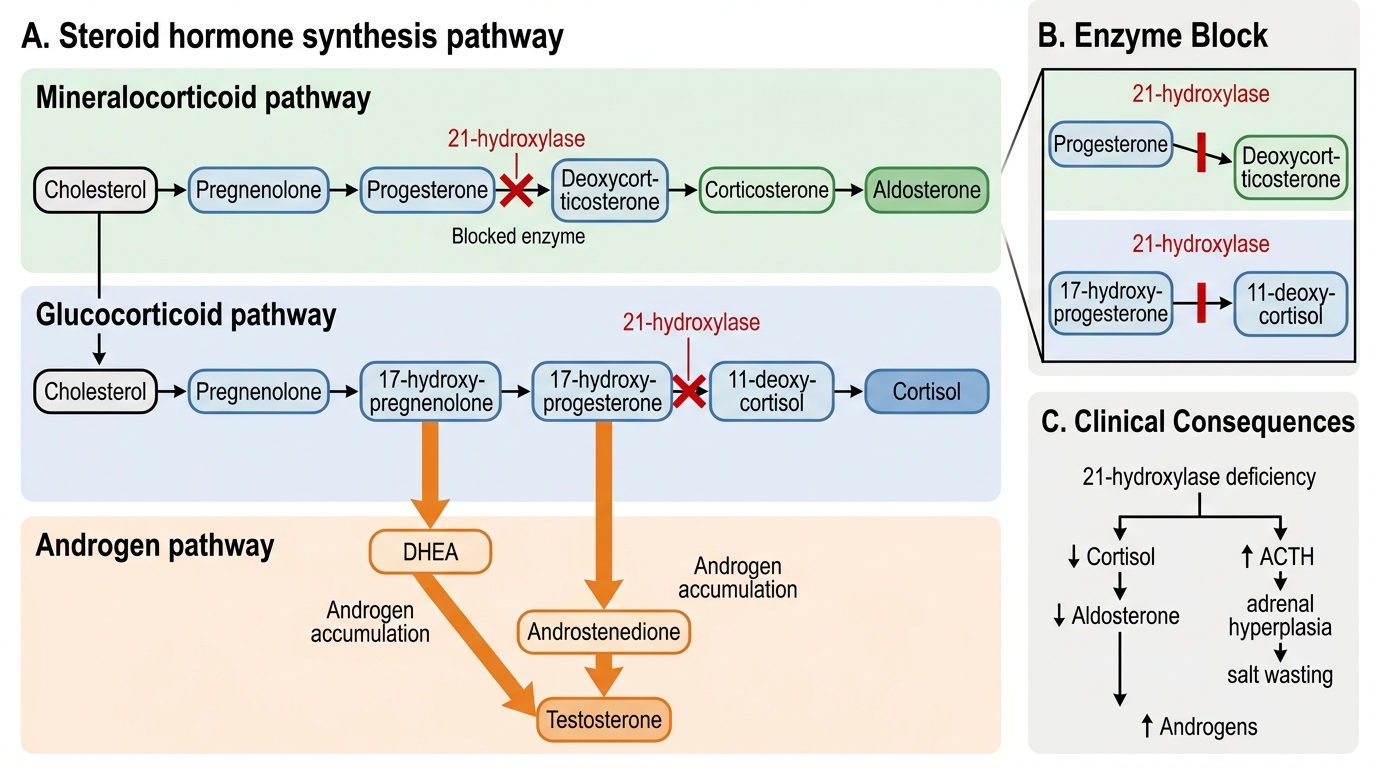
Recall from anatomy and biochemistry: In normal sex development, the SRY gene on the Y chromosome drives undifferentiated gonadal tissue to become testes, which then produce testosterone (Wolffian duct development → male internal genitalia) and anti-Müllerian hormone (AMH, regression of Müllerian structures). In the absence of SRY and testosterone, Müllerian ducts develop into uterus, tubes, and upper vagina (female internal genitalia). External genitalia are undifferentiated until 8 weeks of gestation — they virilise under dihydrotestosterone (DHT, from 5α-reduction of testosterone) or remain female in its absence. Recall the steroid hormone synthesis pathway: cholesterol → pregnenolone → progesterone → 17-hydroxyprogesterone (17-OHP) → 11-deoxycortisol (requires 21-hydroxylase) → cortisol. The adrenal gland also makes aldosterone via a parallel pathway. A block at 21-hydroxylase diverts precursors toward androgens — the biochemical basis of CAH.
Clinical Indication: When to Suspect and Recognise Ambiguous Genitalia
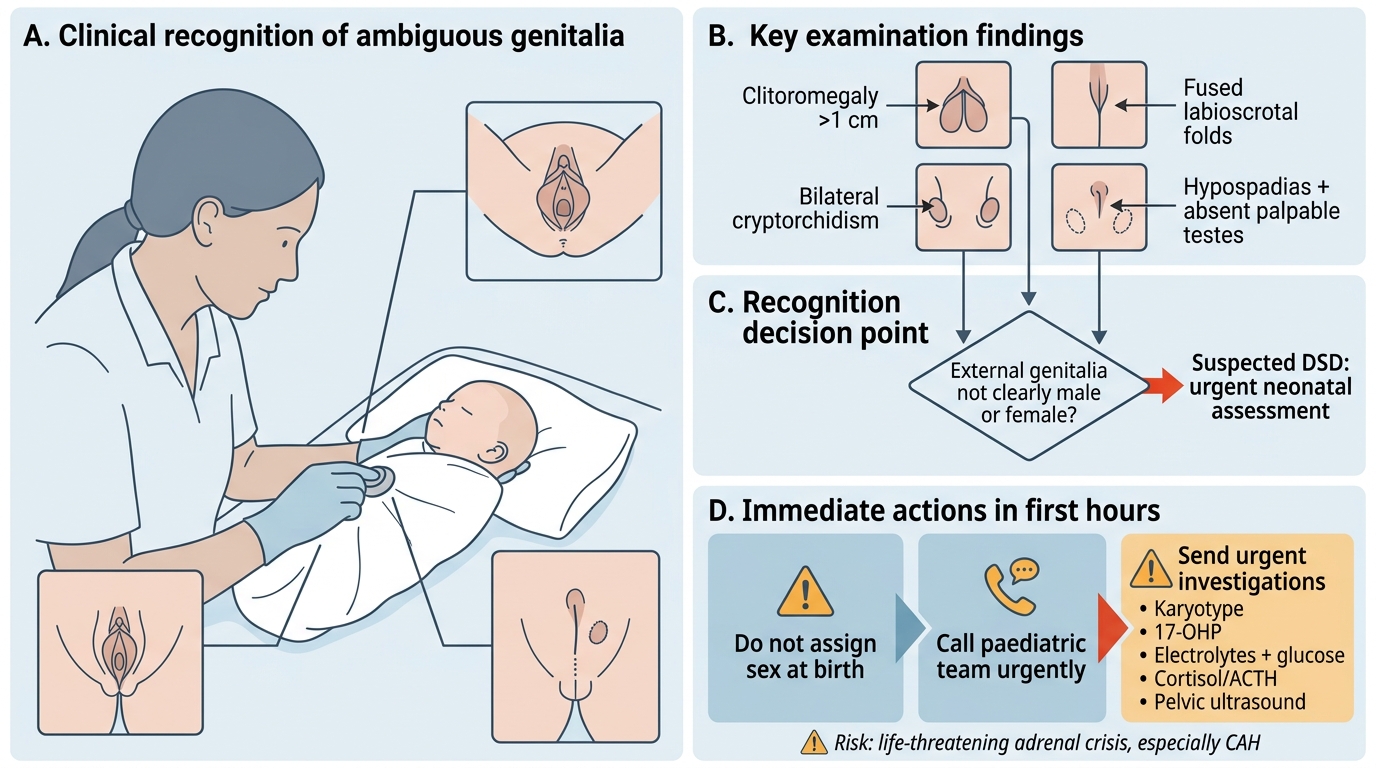
Ambiguous genitalia is defined as external genitalia that cannot be clearly assigned as unambiguously male or female at birth. The immediate clinical task is twofold: correctly identify the finding, and simultaneously screen for life-threatening complications. Several presentations should raise immediate clinical concern: clitoromegaly (enlarged clitoris >1 cm in a newborn), labioscrotal fusion (fused structures with a masculine appearance), hypospadias combined with undescended testes or bifid scrotum, apparent bilateral cryptorchidism (both gonads absent from the scrotum in an apparent male — always suspect DSD), or any genital appearance that does not fit clearly into male or female categories.
Emergency red flag — salt-wasting crisis: In classic 21-hydroxylase deficiency, the aldosterone deficiency causes salt-wasting that typically presents between day 5 and 15 of life. Features include: poor feeding, vomiting, weight loss, lethargy, progressive dehydration, and cardiovascular collapse (hypotension, shock). Electrolytes show hyponatraemia (Na typically <130 mEq/L) and hyperkalaemia (K >6 mEq/L), with hypoglycaemia. A baby with ambiguous genitalia who is unwell, vomiting, or losing weight in the first two weeks of life must be considered to have a salt-wasting crisis until proved otherwise. This is a medical emergency requiring immediate IV hydrocortisone and saline — not a wait-and-see situation.
Important point: At the delivery room, if the midwife or attendant is uncertain about the sex of a newborn, the correct immediate action is to say 'We need to do some tests before we can tell you whether your baby is a boy or a girl' — and call the paediatric team. Never guess and never assign sex based solely on external appearance.
Ambiguous Genitalia at Birth: Recognition and Immediate Action
Anatomy and Governing Principles of Sex Development
Understanding the embryological and biochemical basis of sex development is essential for interpreting the clinical findings in DSD. The critical pathway is: genetic sex (XX or XY) → gonadal differentiation → hormonal environment → internal and external genital differentiation. Disruption at any step produces a DSD.
21-Hydroxylase deficiency (21-OHD) is by far the commonest cause of ambiguous genitalia in India and globally, accounting for >90% of CAH and the majority of 46,XX DSD. The enzyme 21-hydroxylase (encoded by CYP21A2) is essential for both cortisol and aldosterone synthesis. When it is deficient: (1) cortisol synthesis is blocked → corticotropin (ACTH) rises → adrenal hyperplasia; (2) aldosterone synthesis is blocked (in classic salt-wasting type) → sodium loss, potassium retention, adrenal crisis; (3) steroid precursors accumulate and are shunted to androgen synthesis (androstenedione, testosterone, DHT) → virilisation of the 46,XX fetus. The result in a genetic female (46,XX) is female internal genitalia (uterus, ovaries intact — Müllerian structures are preserved because there is no AMH source) but virilised external genitalia (clitoromegaly, labioscrotal fusion, urogenital sinus). The baby is genetically and gonadally female but appears intersex externally.
Other causes of ambiguous genitalia include: (a) 46,XY undervirilisation — androgen insensitivity syndrome (AIS: 5α-reductase deficiency, Leydig cell hypoplasia); (b) Mixed gonadal dysgenesis (45,X/46,XY mosaicism); (c) Maternal androgen excess (ingestion of progestogens, maternal CAH/virilising tumour).
21-Hydroxylase Deficiency in Steroid Hormone Synthesis
Genital Examination Technique and Initial Investigations
A systematic, sensitive, and unhurried genital examination is the foundation of DSD assessment. The examination must be conducted in a private setting, with both parents ideally present (to observe the findings and receive explanation), and performed with the awareness that every action communicates something to the family. The examiner should avoid expressions of surprise, distress, or uncertainty in front of the family.
Structured examination approach: The examiner should begin with general inspection of the perineum before touching, form an initial impression of the anatomy, and then proceed in a standard sequence to ensure nothing is missed. The goal of this structured examination is not to reach a conclusion immediately — it is to gather factual observations that will allow the MDT to reach a diagnosis. Document every finding precisely in writing, ideally with a labelled sketch or photograph (with parental consent), because these observations must be communicated to the specialist team in the referral note.
- Phallus/clitoris size: Measure stretched penile/clitoral length (normal newborn penis: 3.5 ± 0.7 cm; clitoris >1 cm = clitoromegaly); degree of fusion of urogenital folds
- Urogenital anatomy: Location of the urethral opening (normal position vs hypospadiac); presence of a vaginal opening; single perineal opening vs two (suggests urogenital sinus in CAH)
- Gonad palpation: Palpate labioscrotal folds and inguinal canal bilaterally for gonadal tissue. Palpable gonad = contains testicular tissue (ovaries do not descend). In a phenotypic female, a palpable gonad in the labium or inguinal canal strongly suggests 46,XY DSD (e.g. AIS)
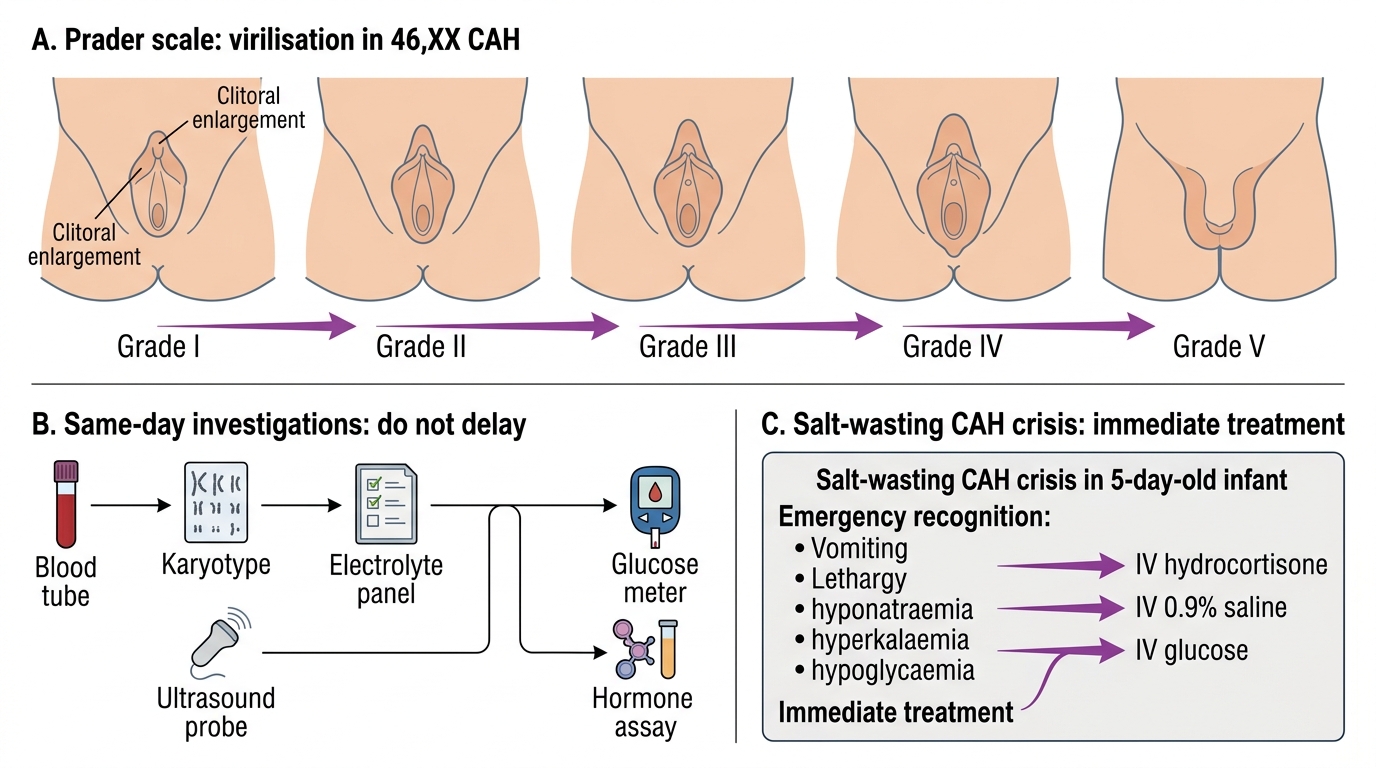
- Prader scale grading (for 46,XX virilised females): Grade I = clitoromegaly only; Grade II = clitoromegaly + partial labial fusion; Grade III = significant clitoromegaly + fused labia with a single perineal opening; Grade IV = phallus with single opening at base; Grade V = male-appearing genitalia with no palpable uterus (but ovaries present)
- General examination: Features of Turner syndrome (webbed neck, lymphoedema); hyperpigmentation of areolae and genitalia (ACTH excess in CAH); signs of dehydration/shock
Prader Scale and Emergency Workup in 46,XX CAH
Urgent initial investigations (send the same day — do NOT delay):
• Karyotype — 46,XX or 46,XY or mosaic
• Serum 17-OHP (17-hydroxyprogesterone) — markedly elevated (>10,000 ng/dL) in 21-hydroxylase deficiency; drawn after 48h of age (neonatal surge normalises by then)
• Serum electrolytes (Na, K) — hyponatraemia + hyperkalaemia = salt-wasting crisis
• Blood glucose — hypoglycaemia in adrenal crisis
• Pelvic and abdominal ultrasound — identify uterus (confirms XX internal anatomy), ovaries/testes, adrenal gland size
• Testosterone and DHT if 46,XY DSD suspected
• Full blood count, blood gas, cortisol if shocked
SELF-CHECK
A 5-day-old with ambiguous genitalia is brought in with vomiting and lethargy. Serum Na is 121 mEq/L and K is 7.4 mEq/L. Blood glucose is 2.1 mmol/L. What is the diagnosis and the IMMEDIATE treatment?
A. Congenital hypothyroidism — start levothyroxine
B. Salt-wasting CAH crisis — IV hydrocortisone (25 mg/m2 bolus) + IV 0.9% saline + glucose
C. Pyloric stenosis — arrange ultrasound for pyloric thickness
D. Septic shock — start broad-spectrum antibiotics and normal saline bolus
Reveal Answer
Answer: B. Salt-wasting CAH crisis — IV hydrocortisone (25 mg/m2 bolus) + IV 0.9% saline + glucose
This is a classic salt-wasting CAH crisis in the setting of ambiguous genitalia: hyponatraemia (Na 121), hyperkalaemia (K 7.4), and hypoglycaemia in a 5-day-old. The immediate treatment is IV hydrocortisone (stress dose 25–50 mg/m2 for crisis, or 100 mg/m2/day in divided doses) plus isotonic saline for volume repletion and glucose for hypoglycaemia. This is a medical emergency — delay of even hours can lead to cardiovascular collapse and death. Sepsis is a differential but the electrolyte pattern (hyponatraemia + hyperkalaemia) is characteristic of mineralocorticoid deficiency in CAH.