Page 4 of 20
PE30.3-4 | Diabetes Mellitus — SDL Guide
Learning Objectives
- Describe the aetiology, clinical types, and clinical features of diabetes mellitus in children
- State the diagnostic criteria for DM and DKA in children
- Perform and interpret a urine dipstick test for glucose and ketone bodies
- Outline the acute management of DKA including weight-based fluid and insulin protocols
- Recognise the warning signs of cerebral oedema in DKA and initiate appropriate referral
INSTRUCTIONS
Diabetes mellitus in children is a lifelong condition with a potentially fatal acute presentation — diabetic ketoacidosis (DKA). Type 1 DM is the commonest form in children, often presenting acutely with DKA at diagnosis. The ISPAD and IAP guidelines set the standards for paediatric DM care. This module prepares you to recognise DM in a child, correctly use the urine dipstick as a first-line screening and monitoring tool, and implement the DKA protocol — including the specific paediatric precautions around cerebral oedema that make paediatric DKA management different from adults.
References
- Ghai Essential Pediatrics, 9th edition, Ch 17 (Endocrinology) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 608–611 (Diabetes) (textbook)
- ISPAD Clinical Practice Consensus Guidelines 2022 (Pediatric DM Management) (guideline)
- IAP Guidelines on Pediatric Diabetes Management 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 8-year-old boy is brought to the emergency room at 2 AM. His mother says he has been drinking large amounts of water and urinating frequently for the past three weeks, has lost 4 kg, and tonight started vomiting and breathing deeply and fast. He looks ill, his eyes are sunken, his breath has a fruity smell, and he is drowsy. His blood sugar on the glucometer reads 'HIGH'. You recognise this pattern immediately — this is not a vague unwell child, this is a paediatric emergency. What you do in the next 30 minutes determines whether this child survives without neurological damage.
WHY THIS MATTERS
Type 1 diabetes mellitus is one of the commonest chronic diseases of childhood, and its acute complication — diabetic ketoacidosis — is a leading cause of paediatric morbidity and mortality. In India, the incidence of both Type 1 and, increasingly, Type 2 DM in children is rising. Approximately 30% of children with Type 1 DM present with DKA at first diagnosis — meaning clinicians at every level need to recognise the condition. The urine dipstick is a universally available, inexpensive bedside tool that can diagnose DKA within minutes and triage patients appropriately. Beyond acute management, understanding DM empowers you to support long-term care: insulin regimens, monitoring, and complication prevention from childhood onwards.
RECALL
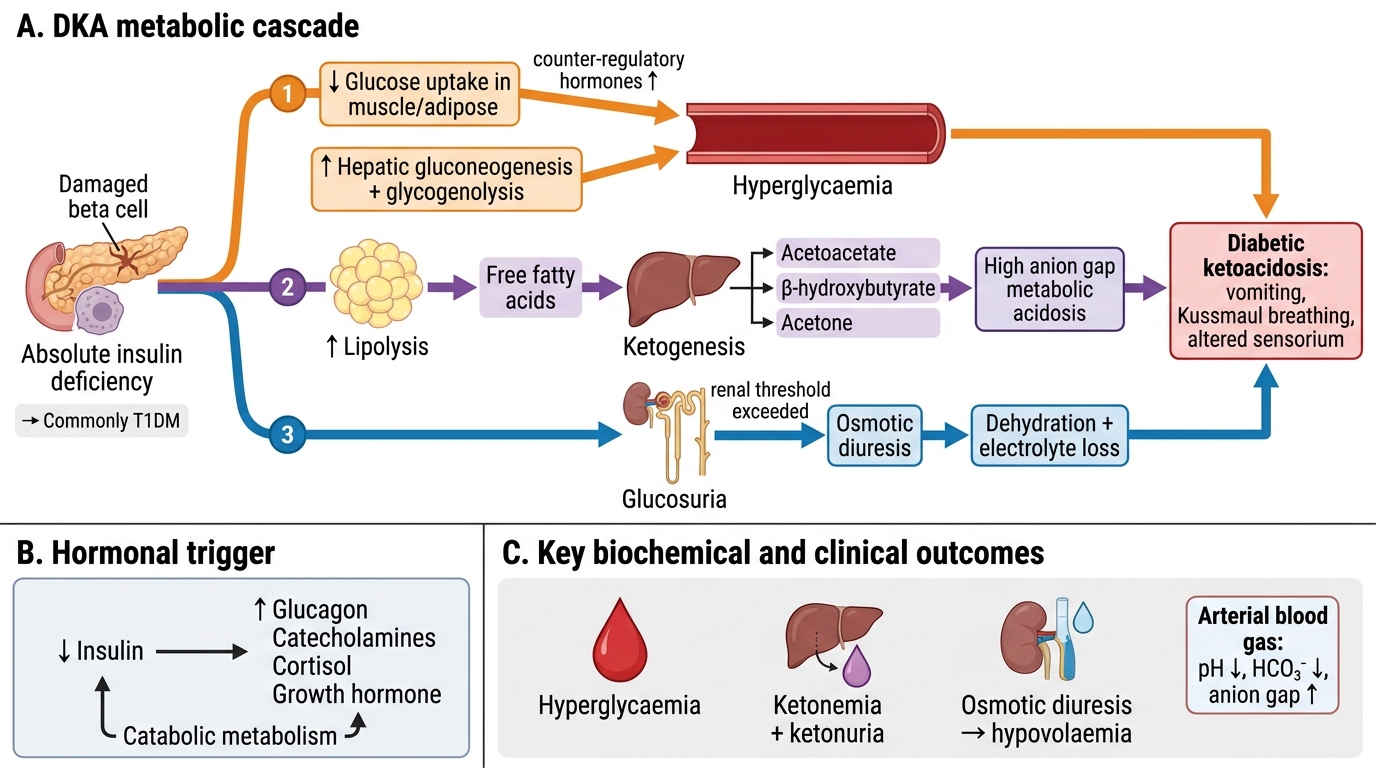
Recall from your basic sciences: The pancreatic beta cells of the islets of Langerhans secrete insulin in response to rising blood glucose. Insulin facilitates glucose uptake into muscle and adipose tissue via GLUT-4 transporters, promotes glycogen synthesis, and inhibits lipolysis and gluconeogenesis. Glucagon from alpha cells opposes insulin — it stimulates glycogenolysis and gluconeogenesis. In insulin deficiency, the metabolic consequence is unopposed glucagon action: glucose cannot enter cells (despite hyperglycaemia), fat is mobilised via lipolysis → free fatty acids → acetyl-CoA → ketone bodies (acetoacetate, beta-hydroxybutyrate). Recall acid-base: ketone bodies are acids — their accumulation lowers blood pH, and the body compensates with hyperventilation (Kussmaul respiration — the deep, rapid breathing you saw in the hook).
Clinical Presentation and Types of Diabetes in Children
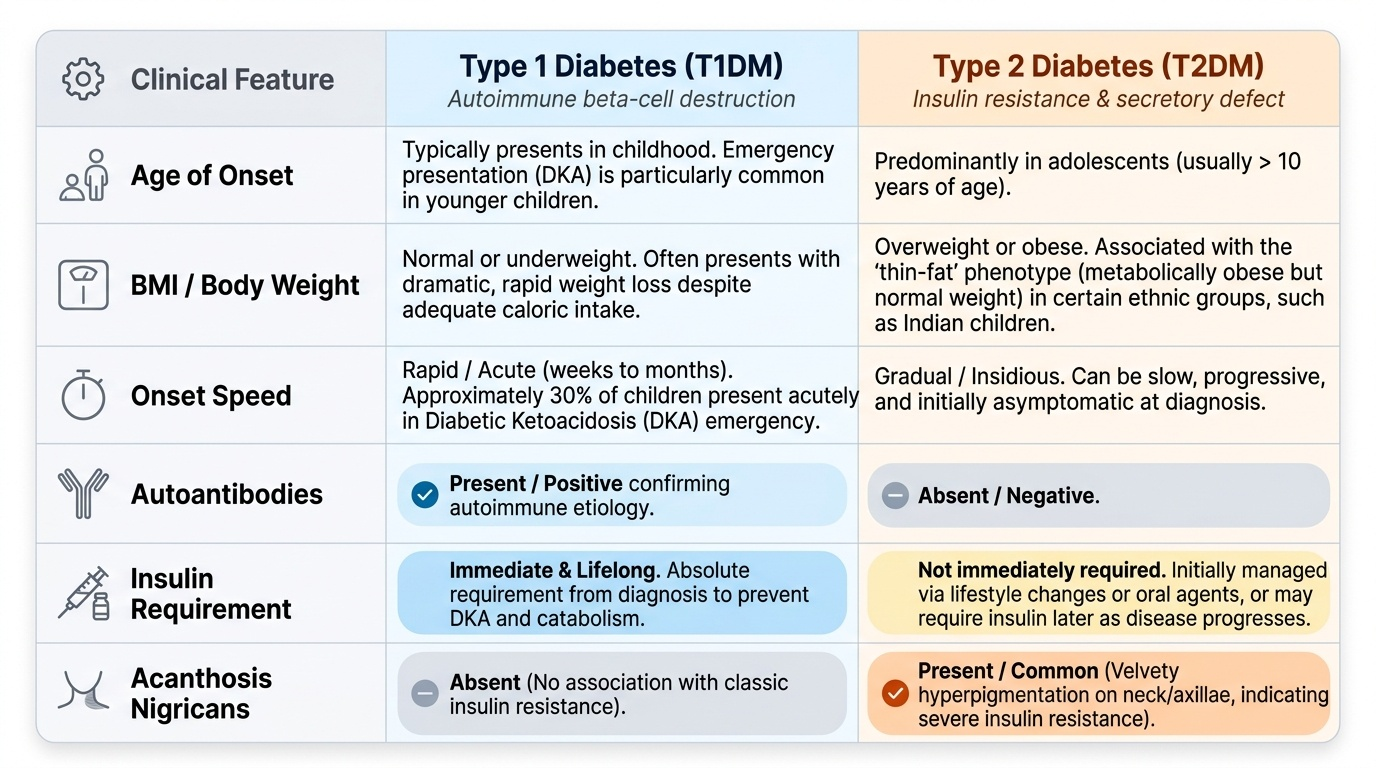
The classic presentation of Type 1 diabetes mellitus (T1DM) in a child is the triad of polyuria, polydipsia, and weight loss — often developing over weeks to months before the child presents acutely. The mechanism is straightforward: hyperglycaemia exceeds the renal glucose threshold (~180 mg/dL), causing glycosuria, osmotic diuresis, and dehydration, which triggers polydipsia. Without insulin, the body catabolises fat and protein — hence the dramatic weight loss despite adequate caloric intake. Children may also present with secondary enuresis (a child who was dry at night beginning to wet the bed again), recurrent skin infections (high glucose = impaired immunity), and blurring of vision. Importantly, 30% of children with T1DM present acutely in diabetic ketoacidosis (DKA) — the metabolic emergency — with nausea, vomiting, abdominal pain, Kussmaul breathing (deep, sighing respirations compensating for metabolic acidosis), fruity-smelling breath (acetone), and deteriorating consciousness. DKA is the typical emergency presentation, particularly in younger children.
Provided image
Type 2 diabetes mellitus (T2DM) in children has a very different clinical picture: it occurs predominantly in overweight and obese adolescents (often with a family history), has an insidious onset, and the patient may be asymptomatic at diagnosis or have features of insulin resistance — acanthosis nigricans (velvety hyperpigmentation of the neck and axillae), signs of polycystic ovary syndrome in girls, and hypertension. T2DM in Indian children is associated with the 'thin-fat' phenotype (metabolically obese but normal weight) as well as frank obesity.
Monogenic diabetes (MODY — maturity-onset diabetes of the young) is rare but important: autosomal-dominant single-gene defects (most common GCK-MODY and HNF1A-MODY), typically non-ketotic, family history in three generations, and often misdiagnosed as T1DM. Neonatal DM (diagnosis <6 months of age) is always monogenic.
Pathophysiology and Aetiology
Type 1 DM results from autoimmune destruction of pancreatic beta cells — a T-cell-mediated process in genetically susceptible individuals (HLA-DR3, DR4), triggered by environmental factors (viral infections such as enteroviruses, dietary factors). The process is gradual: there is a pre-diabetic phase lasting months to years during which beta cells are progressively destroyed, and autoantibodies (anti-GAD65, anti-islet cell antibodies, anti-IA2, anti-ZnT8) appear in the blood before clinical disease. Diabetes manifests when approximately 80–90% of beta-cell mass is lost and insulin secretion is insufficient to control blood glucose. Once established, T1DM requires lifelong exogenous insulin.
DKA metabolic cascade: The absence of insulin triggers a hormonal storm — glucagon, cortisol, adrenaline, and growth hormone all rise. Glycogenolysis and gluconeogenesis drive blood glucose higher (hyperglycaemia → osmotic diuresis → dehydration). Lipolysis releases free fatty acids → hepatic oxidation → acetyl-CoA → ketone bodies (acetoacetate, beta-hydroxybutyrate). Ketone bodies are acids — they deplete bicarbonate (anion-gap metabolic acidosis). The body compensates with hyperventilation (Kussmaul respiration). The combined effect of dehydration (from osmotic diuresis + vomiting), electrolyte loss (Na, K, Cl, phosphate), and acidosis constitutes DKA — a life-threatening emergency.
Type 2 DM pathophysiology in children mirrors the adult form: insulin resistance in muscle, liver, and adipose tissue (driven by obesity and physical inactivity), initially compensated by increased insulin secretion. Over time, beta cells exhaust → relative insulin deficiency → frank hyperglycaemia. Genetic susceptibility (strong family history), environmental (high-calorie diet, sedentary lifestyle), and intrauterine factors (low birth weight → programming of insulin resistance) all contribute.
Metabolic Cascade in Diabetic Ketoacidosis
| Feature | T1DM | T2DM | MODY |
|---|---|---|---|
| Pathogenesis | Autoimmune beta-cell destruction | Insulin resistance + relative deficiency | Monogenic beta-cell/insulin-secretion defect |
| Age of onset | Any age (peak 5–7 yr, 10–14 yr) | Adolescence (pubertal) | Adolescence–young adult |
| Autoantibodies | Anti-GAD, anti-IA2, anti-ZnT8 | Negative | Negative |
| Body habitus | Normal/underweight | Overweight/obese | Variable |
| Insulin required | Always | Not initially | Often not (esp. GCK-MODY) |
SELF-CHECK
A 10-year-old girl is brought with 3-week history of polyuria and polydipsia. Random blood glucose is 310 mg/dL and urine dipstick shows 3+ glucose and 2+ ketones. She is alert and not in distress. What is the MOST appropriate next step?
A. Advise dietary restriction and repeat blood glucose in 2 weeks
B. Start oral metformin immediately
C. Admit for DM workup; check fasting glucose, HbA1c, anti-GAD antibodies, electrolytes, blood gas; begin insulin therapy
D. Perform OGTT to confirm the diagnosis before starting any treatment
Reveal Answer
Answer: C. Admit for DM workup; check fasting glucose, HbA1c, anti-GAD antibodies, electrolytes, blood gas; begin insulin therapy
A random glucose of 310 mg/dL with glycosuria and ketonuria in a child is diagnostic of diabetes mellitus and requires hospital admission. The child is not in DKA (alert, no vomiting, no acidotic breathing) but ketonuria means she is at risk. Workup (anti-GAD, HbA1c, electrolytes) is needed to characterise the type. Metformin alone is not appropriate with ketonuria — insulin is required initially. OGTT is unnecessary when the diagnosis is already confirmed by a random glucose ≥200 mg/dL with symptoms.
Diagnostic Criteria, Investigations, and Urine Dipstick Interpretation
The diagnostic criteria for diabetes mellitus are the same in children as in adults (WHO/ISPAD standards) — but context and urgency differ significantly. Understanding these thresholds is essential because the management decision — whether to investigate further, admit, or begin insulin immediately — depends entirely on which diagnostic tier the child falls into. The WHO and ISPAD diagnostic criteria for DM are based on three measurement types: fasting plasma glucose, post-load (OGTT) glucose, and glycated haemoglobin (HbA1c), with the option of a symptomatic random glucose for acute presentations. In practice, a symptomatic child who is clearly unwell (weight loss, polyuria, polydipsia) does not need an OGTT — the diagnosis can be made from a single random glucose measurement plus symptoms. The OGTT is reserved for asymptomatic individuals where borderline values require clarification. Diabetes is diagnosed when any of the following are present:
• Fasting plasma glucose ≥126 mg/dL (7.0 mmol/L) on two occasions
• 2-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during a 75 g OGTT
• HbA1c ≥6.5% (48 mmol/mol)
• Random plasma glucose ≥200 mg/dL with symptoms of hyperglycaemia
Provided image
In a symptomatic child with classic features (polyuria, polydipsia, weight loss) and a random glucose ≥200 mg/dL, the diagnosis is established — no further testing is needed before starting treatment. The OGTT is reserved for asymptomatic or borderline cases.
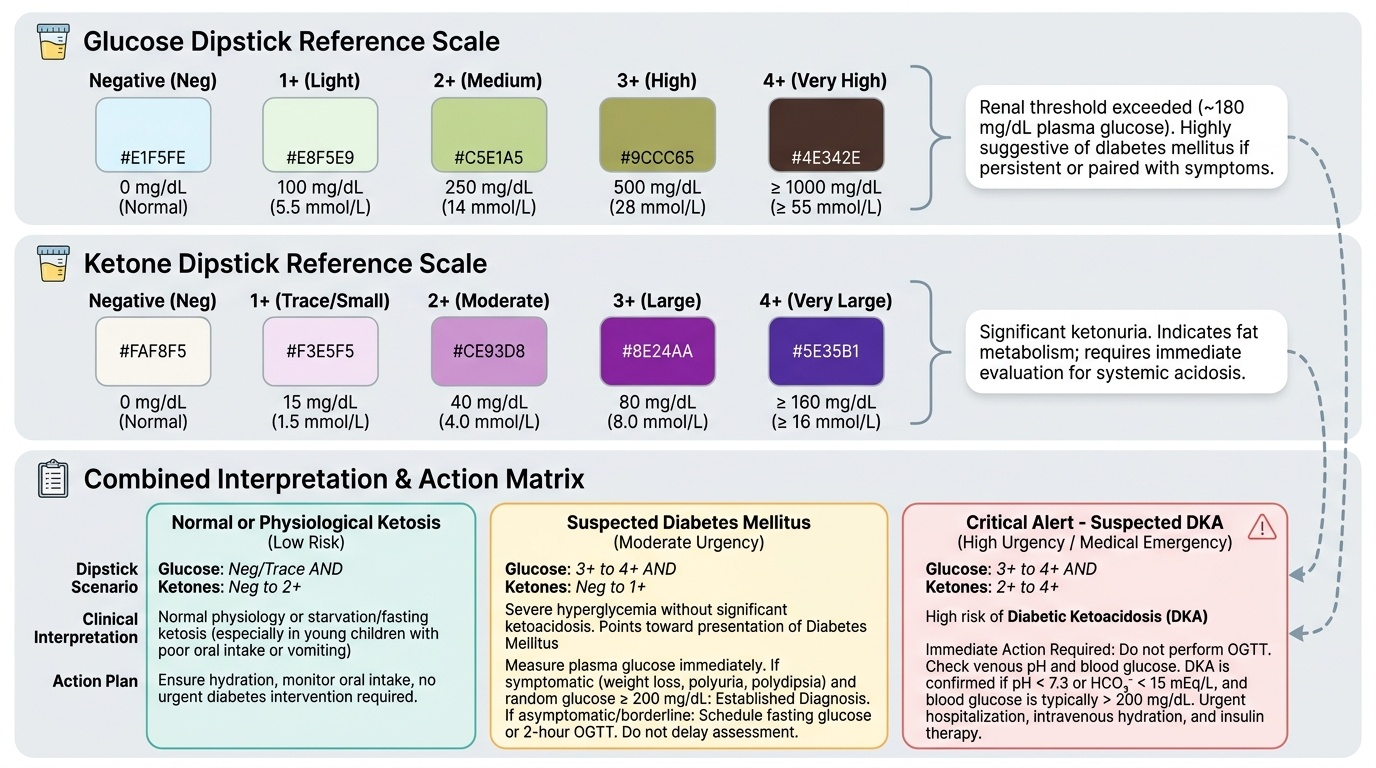
Diabetic Ketoacidosis (DKA) diagnosis requires all three of: (1) Blood glucose >200 mg/dL; (2) Venous pH <7.3 or HCO3 <15 mEq/L; (3) Ketonaemia or ketonuria. Severity is graded: mild (pH 7.2–7.3, HCO3 10–15), moderate (pH 7.1–7.2, HCO3 5–10), severe (pH <7.1, HCO3 <5). Investigations in DKA: blood glucose, venous blood gas, serum electrolytes (Na, K, Cl, HCO3), urea, creatinine, FBC, urine dipstick.
Urine dipstick interpretation: The dipstick is the first-line bedside tool. Glucose: appears when blood glucose exceeds the renal threshold (~180 mg/dL); 1+ to 4+ reflects increasing glucosuria. Ketones: detected as acetoacetate (not beta-hydroxybutyrate — which is the predominant ketone in DKA but is NOT detected by standard dipsticks). A child with 2+ or more ketonuria + glycosuria must be evaluated for DKA. Note that urine glucose alone is non-specific (it occurs in other conditions with low renal threshold); always combine with blood glucose for diagnosis. Critical point for PE30.4 skill: When performing the dipstick, collect a fresh midstream urine sample, dip the strip fully, remove immediately and read at the specified times (30 seconds for glucose, 40 seconds for ketones) — timing errors cause false low readings.
Monitoring investigations in established DM: HbA1c every 3 months (target <7.0–7.5% in children); urine microalbumin/creatinine ratio annually (screening for nephropathy); fundoscopy after 5 years' duration; blood pressure; lipid profile.