Page 14 of 20
PE30.7 | Endocrine Growth Deviation Referral — SDL Guide (Part 2)
Pattern Recognition: Distinguishing Variant from Pathological Growth
Once the growth data are correctly plotted and velocity calculated, the clinical task is to interpret the pattern. The majority of children presenting with short stature in a paediatric clinic will have a normal variant — either familial short stature (FSS) or constitutional delay of growth and puberty (CDGP). However, the minority with a pathological cause — GH deficiency, hypothyroidism, Turner syndrome, chronic illness — require identification. Distinguishing these groups requires integrating the growth pattern, family history, pubertal staging, bone age, and targeted clinical examination.
Provided image
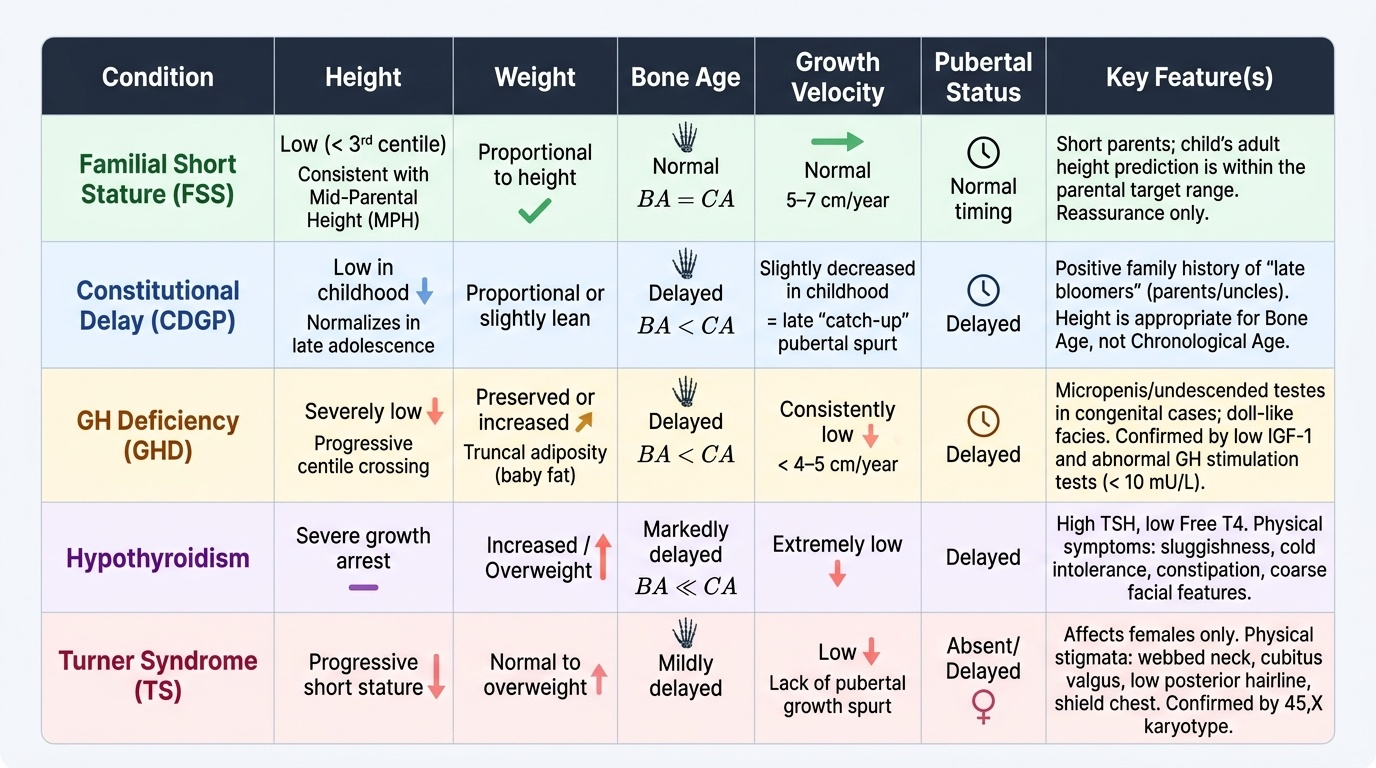
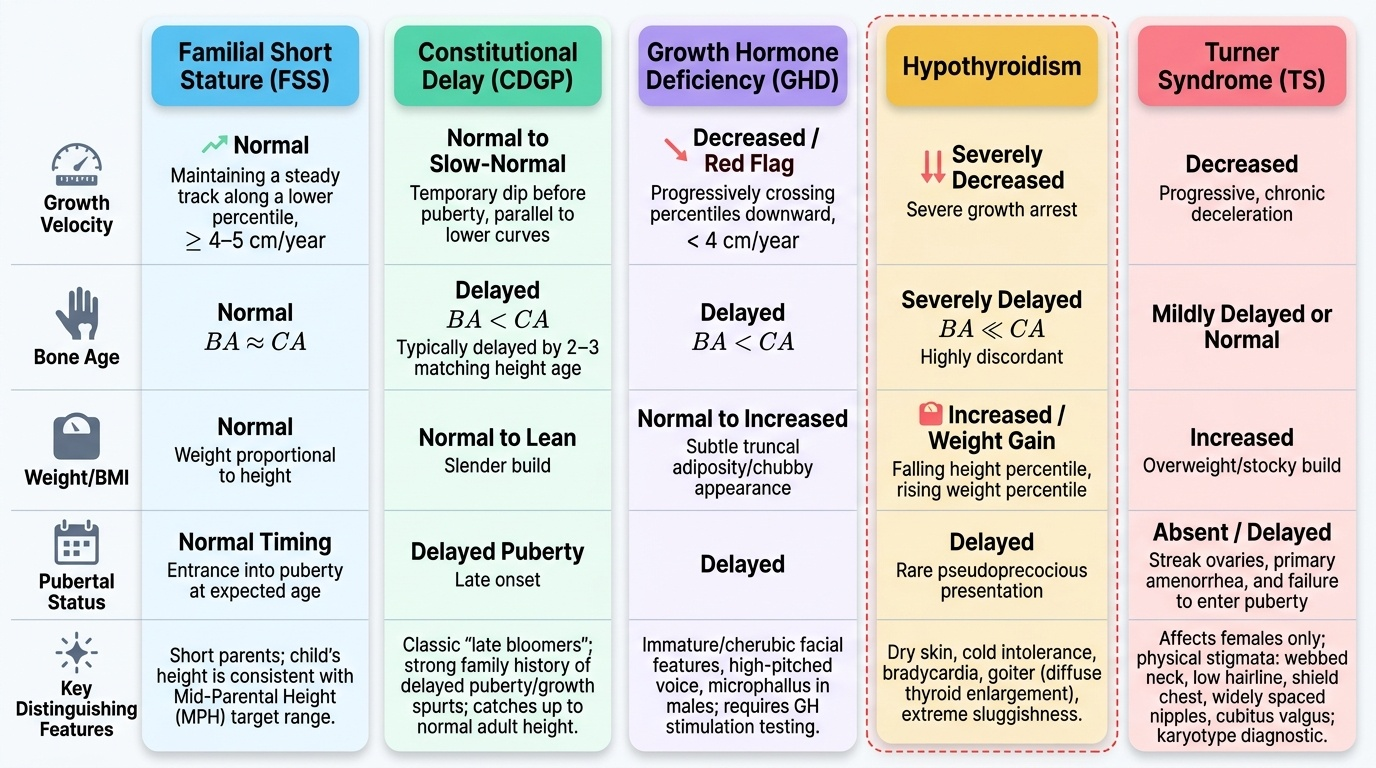
Familial short stature (FSS) is the most common cause of short stature. The child is short but growing at a normal velocity (5–7 cm/yr), has a bone age equal to chronological age, falls within or just below the MPH target range, and has short parents. Puberty occurs at the normal time, and the child reaches an adult height consistent with the family. No investigation or treatment is needed — reassurance and serial monitoring are appropriate.
Constitutional delay of growth and puberty (CDGP) is the second most common normal variant, particularly in boys. The child is short with a delayed bone age (typically 2–3 years behind chronological age), reduced growth velocity during childhood, but then a late pubertal growth spurt that brings them into the normal adult range. Typically there is a positive family history of 'late developer' (parent or uncle/aunt who grew late). Puberty is delayed. Crucially, the child's height is appropriate for their bone age, not their chronological age. CDGP is self-limiting but can cause significant psychological distress; in severe cases, low-dose sex steroids can be used to induce puberty under specialist supervision.
GH deficiency (GHD) presents with a consistently low growth velocity (<4–5 cm/yr), progressive centile crossing (usually apparent by age 3–4 years), delayed bone age, preserved body proportions, increased body fat (particularly truncal), and micropenis or undescended testes in boys with congenital GHD. Intelligence is normal. IGF-1 levels are low; GH stimulation tests (peak GH <10 mU/L on two provocative tests) confirm the diagnosis. MRI brain may reveal pituitary hypoplasia or a hypothalamic lesion.
Hypothyroidism in childhood typically presents with growth failure plus the classical features of hypothyroid state: weight gain, constipation, cold intolerance, dry skin, bradycardia, prolonged nausea, and goitre. Bone age is markedly delayed. TSH is elevated and free T4 is low. Importantly, hypothyroidism can present with no obvious classical features in school-age children — growth failure or declining academic performance may be the only early signs.
Turner syndrome (45,X monosomy, and its mosaic variants) is the most important chromosomal cause of short stature in girls. All girls with unexplained short stature and no obvious pathological cause should have a karyotype performed. Other features include webbed neck, low posterior hairline, shield chest, wide-carrying angle (cubitus valgus), cardiac defects (bicuspid aortic valve, coarctation), and primary amenorrhoea. Growth velocity is reduced throughout childhood; GH therapy is indicated and effective.
Chronic systemic disease — coeliac disease, inflammatory bowel disease, chronic renal failure, congenital heart disease, chronic respiratory disease — suppresses growth through a combination of malnutrition, inflammation, and in some cases steroid therapy. The systemic disease is usually apparent clinically, but subtle coeliac disease can present with growth failure as the only feature.
CLINICAL PEARL
The single most useful discriminating question in a child with short stature is: 'What was this child's growth velocity over the last 12 months?' A child with height on the 1st centile but a velocity of 6 cm/yr is almost certainly a normal variant. A child on the 15th centile but with a velocity of 3 cm/yr has a significant problem. Never accept a family's description of growth — measure it yourself, at least twice, separated by 6 months. And always examine for goitre: a school-age child with a goitre and growth failure has hypothyroidism until proven otherwise.
SELF-CHECK
An 8-year-old boy has height on the 3rd centile, bone age of 6 years, growth velocity of 5 cm/yr, delayed puberty, and a positive family history of late puberty in his father. His IGF-1 is at the lower end of normal for his chronological age but normal for his bone age. Which diagnosis is most likely?
A. GH deficiency
B. Constitutional delay of growth and puberty (CDGP)
C. Familial short stature
D. Hypothyroidism
Reveal Answer
Answer: B. Constitutional delay of growth and puberty (CDGP)
This is the classic CDGP pattern: delayed bone age (6 vs 8 years), normal growth velocity for bone age, delayed puberty, and positive family history of late development. IGF-1 is normal when interpreted against bone age (not chronological age) — a common error that leads to unnecessary GH stimulation testing. Familial short stature has bone age equal to chronological age. GHD has low growth velocity and lower IGF-1. Hypothyroidism would show weight gain, goitre, and other systemic features. CDGP requires reassurance, not treatment, in most cases.
Referral Decision-Making: Criteria, Urgency, and Communication
Having assessed and characterised the growth pattern, the final clinical skill is the referral decision: who to refer, when, and how. This decision should be systematic, not instinctive — it requires applying defined criteria rather than relying on clinical intuition alone. The purpose of a structured referral framework is twofold: it ensures that children who genuinely need specialist evaluation are not missed, and it protects families from unnecessary anxiety and cost when a child is growing normally within the expected range for their genetic background. The following referral criteria are based on IAP guidance and standard paediatric endocrinology practice in India. Meeting any one criterion from the 'absolute indications' list is sufficient to warrant referral; several together warrant urgent referral. Timing matters because most endocrine causes of growth failure are most effectively treated during the pre-pubertal window, before growth-plate fusion limits the response to therapy. A delayed referral can mean the difference between a child achieving near-normal adult height and being permanently short.
Absolute referral indications (refer all):
1. Height below 3rd centile AND growth velocity <4 cm/yr in a school-age child
2. Centile crossing — crossing ≥2 major centile lines downward over 12–18 months
3. Height significantly below mid-parental height target range (>8.5 cm below lower target)
4. Clinical features of GH deficiency (low velocity + truncal obesity + micropenis/undescended testis)
5. Clinical features of hypothyroidism (low velocity + weight gain + goitre ± bradycardia)
6. Any girl with unexplained short stature — karyotype to exclude Turner syndrome
7. Suspected chronic systemic disease causing growth failure
8. Tall stature with accelerated bone age or signs of precocious puberty
Observation with monitoring (not immediate referral if ALL criteria met):
1. Height below 3rd centile but growth velocity is normal (≥5 cm/yr)
2. MPH target range is consistent with current height
3. Bone age is appropriate for height age
4. No systemic or dysmorphic features
5. Family history of short stature or constitutional delay confirmed
In this scenario, review in 6 months with repeat measurement and reassess velocity.
What to include in the referral letter:
• Current and at least two previous height and weight measurements with dates
• Calculated growth velocity
• Mother's and father's heights with computed MPH and target range
• Pubertal stage (Tanner staging)
• Bone age result if available
• Thyroid function and IGF-1 results if already sent
• Brief summary of systemic features, medications (especially steroids), chronic illness
• Family history of short stature, late puberty, endocrine disease
Counselling the family: Explain that you are referring because the pattern of growth warrants specialist evaluation — not because there is necessarily something seriously wrong. Avoid premature diagnosis-labelling ('he probably has a hormone problem') which causes unnecessary anxiety. Explain that the specialist will likely repeat measurements, perform blood tests, and possibly an X-ray of the wrist. Reassure that most causes — if found — are treatable, especially when identified before puberty.
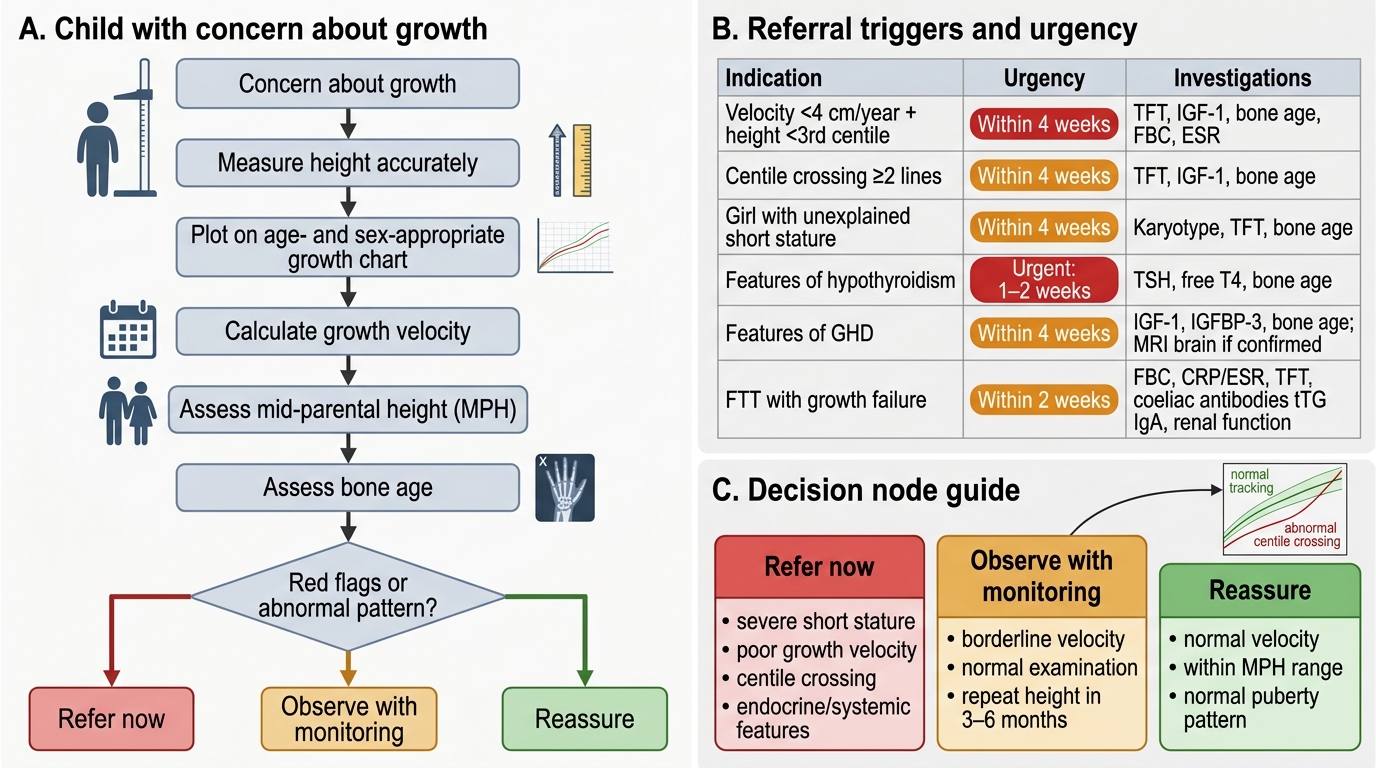
Algorithm for Assessing Growth Concern in a Child
| Indication | Urgency | Investigations to send with referral |
|---|---|---|
| Velocity <4 cm/yr + height <3rd centile | Within 4 weeks | TFT, IGF-1, bone age, FBC, ESR |
| Centile crossing ≥2 lines | Within 4 weeks | TFT, IGF-1, bone age |
| Girl with unexplained short stature | Within 4 weeks | Karyotype, TFT, bone age |
| Features of hypothyroidism | Urgent (1–2 weeks) | TFT (TSH + free T4), bone age |
| Features of GHD | Within 4 weeks | IGF-1, IGFBP-3, bone age, MRI brain if confirmed |
| FTT with growth failure | Within 2 weeks | FBC, CRP/ESR, TFT, coeliac antibodies (tTG IgA), renal function |
| Normal variant (FSS/CDGP) | Routine or observe | None required; review in 6 months |
Self-Assessment: Consolidating Growth Deviation Skills
This section consolidates the full PE-skills arc through a self-directed case review exercise. The aim is to apply the structured approach — measurement, velocity, MPH, pattern recognition, referral decision — to a scenario that integrates the key clinical distinctions covered in this module.
Provided image
Case for self-assessment: Ajay is a 12-year-old boy whose parents are concerned that he is not growing. His height today is 138 cm; a school record from 2 years ago shows 132 cm. His father is 165 cm and his mother is 152 cm. On examination, he is prepubertal (Tanner stage 1). His skin is dry, he is slightly overweight, and he has a subtle, smooth, diffuse thyroid enlargement. His bone age X-ray (which you organised last week) shows a bone age of 9 years.
Work through the following questions before revealing the explanations:
1. What is his growth velocity, and is it a red flag?
2. What is the mid-parental height and target range, and where does he fall?
3. What pattern does the combination of low velocity + delayed bone age + weight gain + goitre suggest?
4. Which investigation result do you most need before the next step?
5. Is this a refer-now, refer-soon, or observe scenario, and why?
Self-assessment answers:
1. Growth velocity: (138 − 132) ÷ 2 years = 3 cm/yr — well below the 4–5 cm/yr red-flag threshold. This is a significant red flag.
2. MPH: (165 + 152 + 13) ÷ 2 = 165 cm; target range = 165 ± 8.5 = 156.5–173.5 cm. At 138 cm currently he is below where he should be, but we are comparing to an adult target — the key is that his velocity is flagged.
3. The combination of low growth velocity, delayed bone age (9 vs 12 years), weight gain, dry skin, prepubertal at 12, and goitre is the classic triad of acquired hypothyroidism in a school-age child.
4. Thyroid function tests (TSH and free T4) — a raised TSH with low fT4 confirms primary hypothyroidism. Starting levothyroxine treatment will correct growth failure if initiated promptly.
5. This is a refer urgently (1–2 weeks) scenario — clinical hypothyroidism is a treatable cause of growth failure and delay in treatment means further bone-age advancement and irreversible stature loss.
- Growth velocity <4–5 cm/yr = always investigate regardless of centile position
- Bone age delayed + weight gain + goitre = hypothyroidism until proven otherwise
- Refer urgently for suspected hypothyroidism — treatment reverses growth failure
SELF-CHECK
A 9-year-old girl is referred for short stature. Her height is on the 5th centile, growth velocity is 5.5 cm/yr, bone age equals chronological age, and her mother's height is on the 8th centile. No dysmorphic features. What is the most appropriate management?
A. Refer urgently for GH stimulation testing
B. Request karyotype to exclude Turner syndrome
C. Reassure and review in 6 months with serial growth measurements
D. Start levothyroxine empirically
Reveal Answer
Answer: C. Reassure and review in 6 months with serial growth measurements
This child has the hallmarks of familial short stature (FSS): height consistent with maternal height (5th centile mother, 5th centile child), normal growth velocity (5.5 cm/yr), bone age equal to chronological age, and no dysmorphic features or systemic signs. FSS is a normal variant requiring reassurance and serial monitoring, not investigation or treatment. Turner syndrome (option B) should be considered in girls with unexplained short stature, but here the family history fully accounts for her stature. GH testing and levothyroxine are not indicated in the absence of velocity or clinical red flags.