Page 10 of 20
PE30.6 | Puberty Disorders — SDL Guide
Learning Objectives
- Define precocious puberty and delayed puberty with the correct age thresholds for boys and girls
- Perform Sexual Maturity Rating (Tanner staging) for breast development and genital/pubic hair
- Distinguish GnRH-dependent (central) from GnRH-independent (peripheral) precocious puberty
- Outline the diagnostic investigations for abnormal pubertal timing and indications for referral
INSTRUCTIONS
Puberty is one of the most transformative biological events of childhood — and disorders of its timing carry major consequences: short adult stature, psychological distress, underlying pathology (brain tumour, ovarian cyst, gonadal failure). The Sexual Maturity Rating (SMR, also called Tanner staging) is the universal clinical tool for documenting pubertal progress, and every paediatrician must be able to perform and interpret it accurately. This module walks you through the definitions, examination technique, differential diagnosis, and management of the two major timing disorders.
References
- Ghai Essential Pediatrics, 9th edition, Ch 17 (Endocrinology) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 578–580 (Puberty Disorders) (textbook)
- IAP Consensus on Management of Precocious Puberty 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-year-old girl is brought by her alarmed mother: 'She has started growing breasts and has a few pubic hairs — she's only 6!' On examination, you confirm Tanner breast stage II–III, sparse pubic hair, and the child appears taller than expected for age. There is no acne, no vaginal bleeding. Her mother wants to know if something is wrong. You know the answer begins with a systematic clinical assessment — Tanner staging, growth chart review, bone age — and that the cause determines whether this child needs urgent brain imaging or reassurance. Getting this right matters: if this is central precocious puberty and you miss a brain tumour, the consequences are irreversible.
WHY THIS MATTERS
Disorders of pubertal timing — both too early and too late — are among the most common endocrine referrals in paediatric practice. Precocious puberty (PP) affects approximately 1 in 5,000–10,000 children; the great majority are girls with idiopathic central PP, but boys with PP more often have an identifiable cause (CNS pathology in approximately 50% of cases). Delayed puberty is most often constitutional but can signal hypogonadism, systemic disease, or a CNS tumour. The Sexual Maturity Rating (SMR/Tanner scale) is the foundation of the clinical assessment — it allows you to objectively document and communicate the stage of development, compare it to age norms, and make referral decisions. This skill is tested in OSCEs and is a basic clinical competency for any doctor who sees adolescents.
RECALL
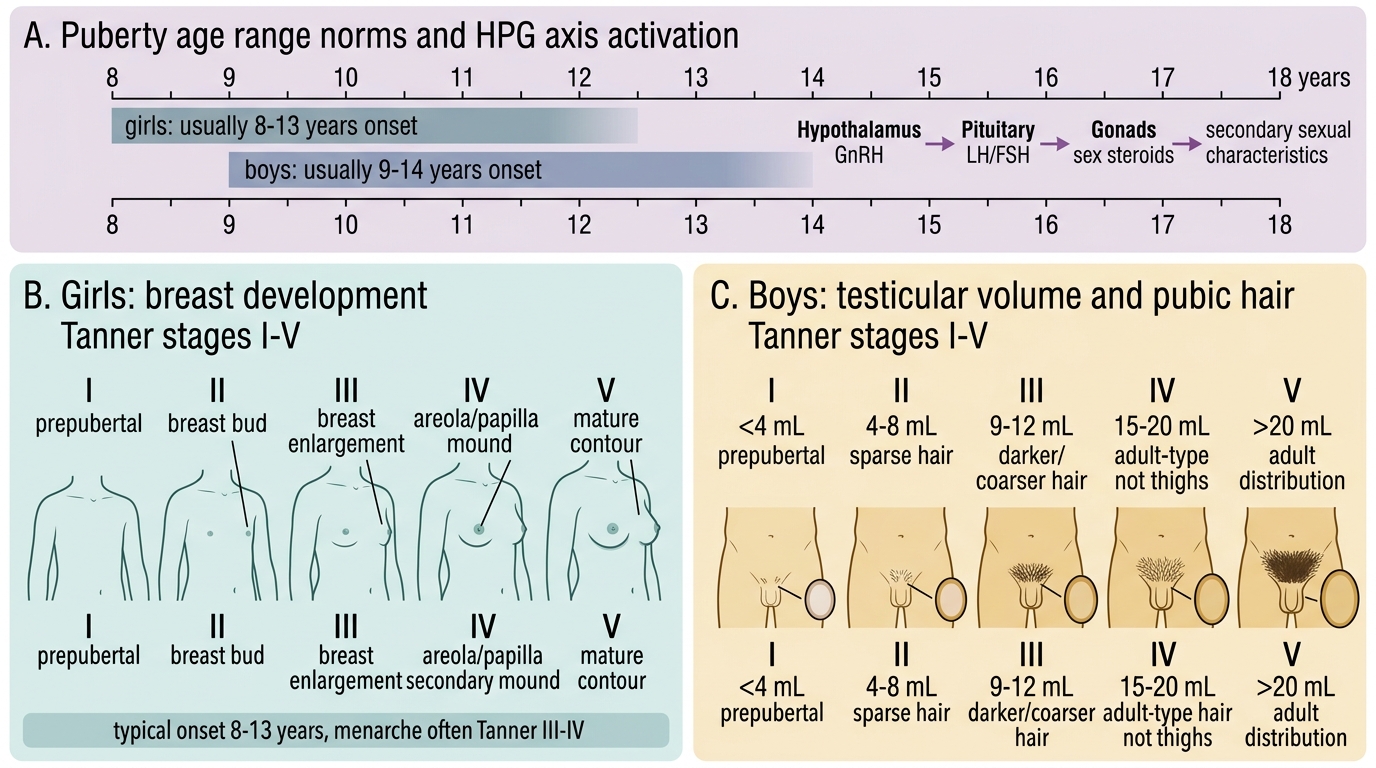
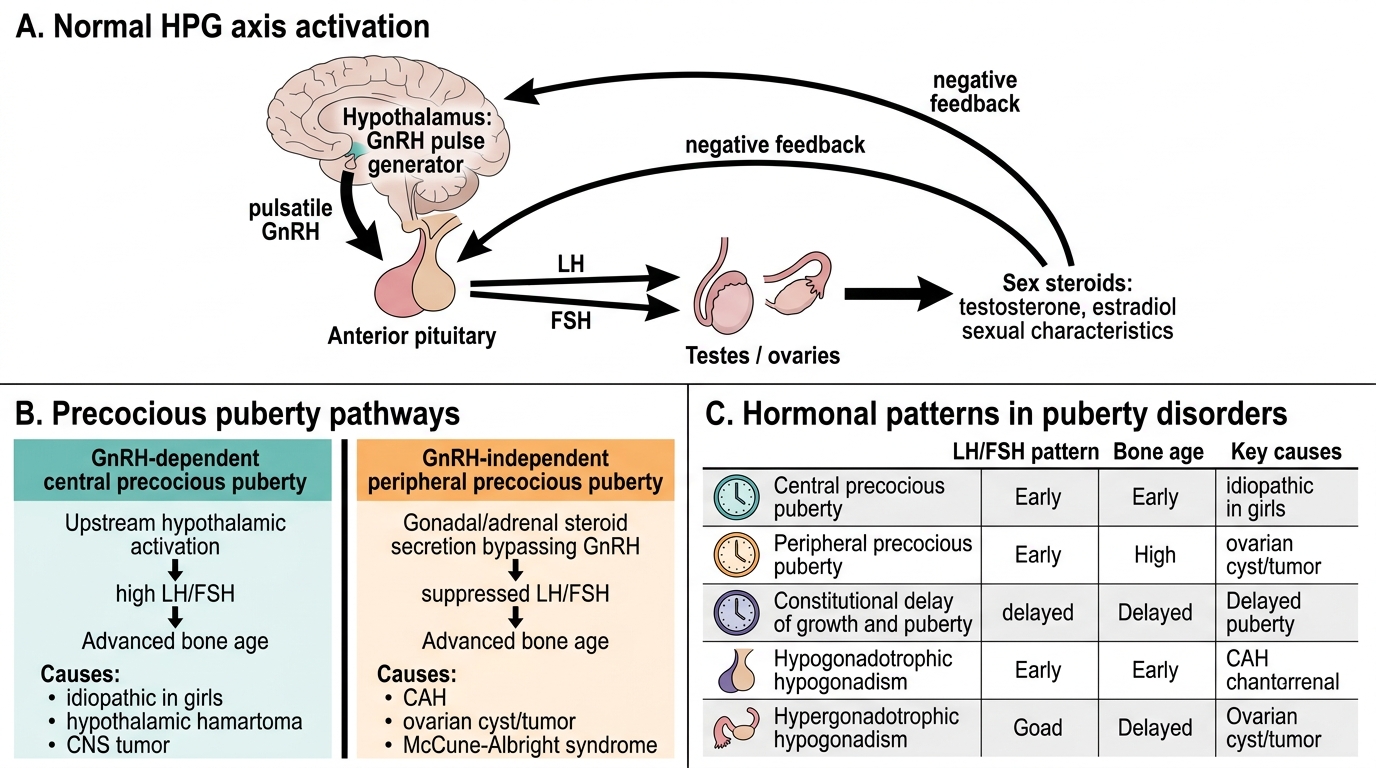
Before proceeding, recall the normal physiology of puberty from your basic sciences: Puberty is initiated when the hypothalamic GnRH pulse generator — which is suppressed in mid-childhood — reactivates, releasing GnRH in pulses that stimulate the pituitary to secrete LH and FSH. LH and FSH act on the gonads to produce sex steroids: estradiol in girls (breast development, uterine growth, female fat distribution), testosterone in boys (testicular enlargement, voice change, phallus growth, muscle mass). In girls, the first sign of puberty is thelarche (breast development); in boys, the first sign is testicular enlargement (gonadal volume >4 mL). Recall also adrenarche: the adrenal glands independently begin producing androgens (DHEAS) at 6–8 years, causing pubic and axillary hair and mild apocrine sweating (pubarche) — this is independent of the HPG axis and does not indicate true puberty. Recall that bone age reflects maturity, not age, and is read from a left hand/wrist radiograph.
Clinical Presentation: Recognising Abnormal Pubertal Timing
The clinical presentation of puberty disorders is anchored in age and the sequence of pubertal changes, assessed using the Sexual Maturity Rating (SMR), also called Tanner staging. The SMR documents the development of breasts and pubic hair in girls (stages I–V for each) and testicular volume with pubic hair in boys (stages I–V), providing an objective, reproducible, and universally used measure of pubertal progress.
Precocious puberty (PP) is defined as the onset of pubertal changes before the age of 8 years in girls and 9 years in boys. The child and family typically present with the unexpected appearance of breasts or pubic hair in a young girl, or testicular enlargement, pubic hair, and voice change in a young boy. The child may be noticeably taller than classmates (advanced bone age), have body odour, or display emotional changes. Girls with central PP (GnRH-dependent) develop in the correct sequence: thelarche first, then pubarche, then menarche. Girls with peripheral PP (GnRH-independent) may have isolated vaginal bleeding without breast development, or a McCune-Albright triad (café-au-lait spots + fibrous dysplasia + precocious puberty). Boys with PP always need brain MRI — the cause is identified in about 50% of cases (hypothalamic hamartoma, CNS tumour, hydrocephalus).
Delayed puberty is defined as absence of breast development by age 13 years in girls or absence of testicular enlargement (volume <4 mL) by age 14 years in boys. Presentation is a teenager who appears younger than peers, may be shorter, and is often distressed by the difference. Boys are more commonly referred than girls because the social visibility of pubertal delay is greater. The most common cause is constitutional delay of growth and puberty (CDGP) — the child is developmentally 'normal but late', with a family history of late puberty, bone age matching developmental rather than chronological age, and no underlying disease.
Sexual Maturity Rating: Tanner Stages I-V
Pathophysiology and Aetiology
The pathophysiology of puberty disorders reflects the specific level of the HPG axis at which regulation is disrupted. Understanding this is essential for classifying the cause and choosing the investigation.
Precocious puberty — classification by HPG axis level:
GnRH-dependent (central/true) PP: The entire HPG axis is prematurely activated. The hypothalamic GnRH pulse generator fires early, stimulating LH and FSH, which in turn stimulate the gonads. This is the commonest form in girls (usually idiopathic, >80%) and must be investigated in boys (50% have a CNS cause). LH and FSH are elevated (pubertal range); sex steroids are gonadal in origin. Bone age is advanced because sex steroids accelerate growth plate closure — the child is tall now but may be short as an adult if untreated. Causes: hypothalamic hamartoma (the most common identified cause in both sexes), astrocytoma/optic glioma, craniopharyngioma, neurofibromatosis, prior CNS infection/radiation, hydrocephalus.
GnRH-independent (peripheral) PP: Sex steroids are produced autonomously, without HPG axis activation. LH and FSH are LOW (suppressed by the high peripheral sex steroids). Causes in girls: ovarian follicular cysts, ovarian/adrenal tumour, McCune-Albright syndrome (activating GNAS mutation → autonomous ovarian estrogen production + café-au-lait spots + fibrous dysplasia), exogenous oestrogen. Causes in boys: CAH (excess androgens from adrenal — important differential), testicular tumour (Leydig cell tumour), HCG-secreting tumour (hepatoblastoma, germinoma), exogenous androgens. In CAH the bone age is very advanced, androgen levels are high but LH/FSH are suppressed.
Delayed puberty — classification:
The most useful classification separates by gonadotrophin levels:
• Constitutional delay of growth and puberty (CDGP): Commonest cause (~60–70%); bone age delayed; LH/FSH normal for pubertal stage (not elevated); karyotype normal; positive family history; no underlying disease. These children eventually progress normally — just later.
• Hypogonadotrophic hypogonadism (central): Pituitary or hypothalamic failure — low LH/FSH despite delayed puberty. Causes: Kallmann syndrome (GnRH deficiency + anosmia), hypopituitarism, craniopharyngioma, chronic illness (malnutrition, chronic renal disease), hypothyroidism, excessive exercise (female athlete triad).
• Hypergonadotrophic hypogonadism (primary gonadal failure): The gonads fail to respond to LH/FSH — LH/FSH are HIGH (the pituitary is trying to stimulate an unresponsive gonad). Causes: Turner syndrome (45,X — girls: short stature, streak gonads, webbed neck), Klinefelter syndrome (47,XXY — boys: tall, small testes, gynecomastia), gonadal dysgenesis, chemotherapy/radiation damage.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
HPG Axis Activation and Puberty Disorders
| Type | LH/FSH | Bone Age | Key causes |
|---|---|---|---|
| Central (GnRH-dep) PP | Elevated (pubertal) | Advanced | Idiopathic (girls), hypothalamic hamartoma, CNS tumour |
| Peripheral (GnRH-indep) PP | Low (suppressed) | Advanced | CAH, ovarian cyst/tumour, McCune-Albright |
| CDGP (delayed) | Normal for stage | Delayed | Constitutional (family history) |
| Hypogonadotrophic | Low | Delayed | Kallmann, malnutrition, hypopituitarism |
| Hypergonadotrophic | High | Delayed | Turner (45,X), Klinefelter (47,XXY), radiation |
SELF-CHECK
A 7-year-old girl has breast development (Tanner stage II) and pubic hair (Tanner stage II). Her LH is 8 IU/L (elevated, pubertal) and FSH is 6 IU/L. Bone age is 10 years. What is the MOST likely diagnosis?
A. GnRH-independent (peripheral) precocious puberty from an ovarian cyst
B. Constitutional delay of puberty
C. GnRH-dependent (central) precocious puberty
D. Premature adrenarche only
Reveal Answer
Answer: C. GnRH-dependent (central) precocious puberty
Elevated LH and FSH (pubertal range) + complete thelarche + pubarche + advanced bone age in a 7-year-old girl = central (GnRH-dependent) precocious puberty, where the entire HPG axis has been prematurely activated. In peripheral PP, LH/FSH would be suppressed (low) because the autonomous sex-steroid production suppresses the HPG axis. Premature adrenarche causes only pubic hair (pubarche) without thelarche and LH/FSH are not elevated. Constitutional delay of puberty would present as delayed, not early, development.
Diagnosis, Investigation, and Sexual Maturity Rating (SMR)
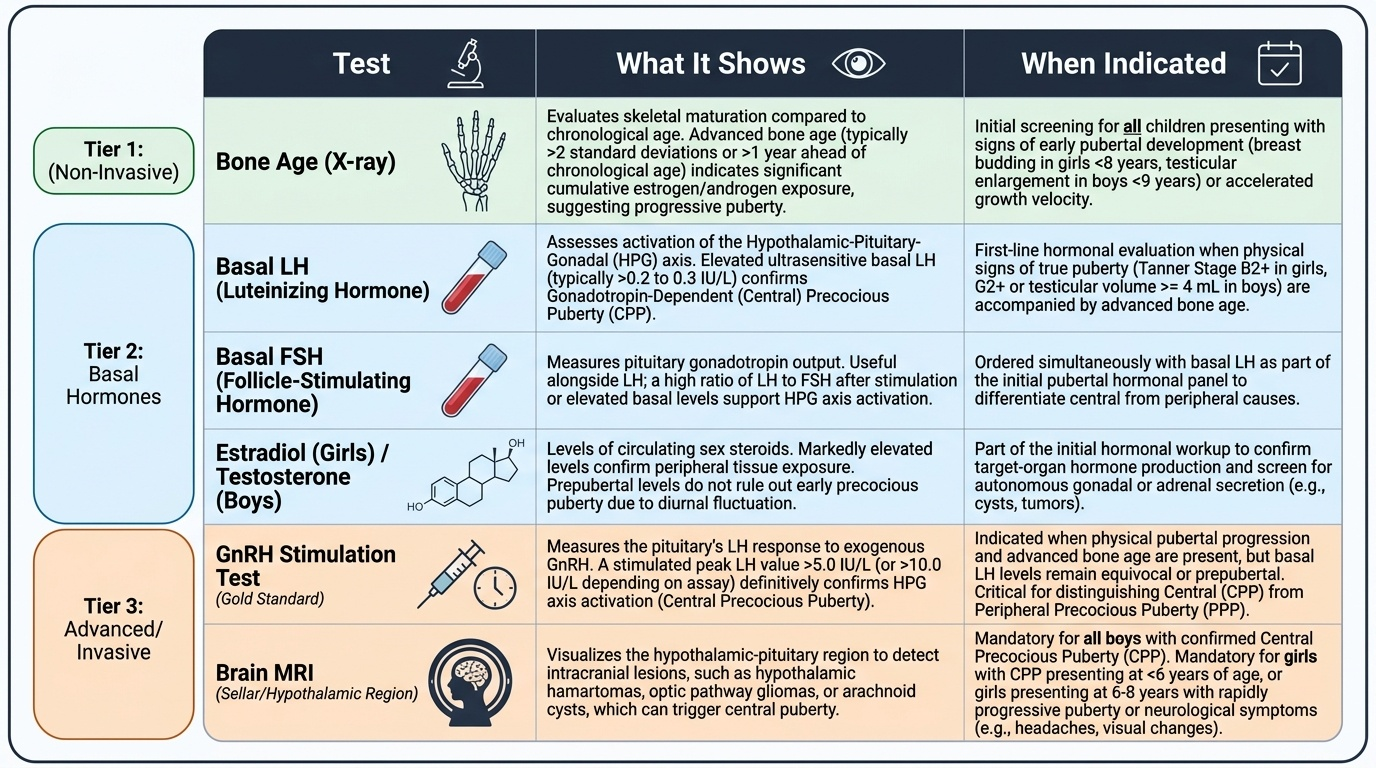
The diagnostic approach to puberty disorders begins at the bedside with the Sexual Maturity Rating (SMR) assessment, proceeds to growth chart and bone-age evaluation, and then to targeted laboratory and imaging investigations based on the clinical picture. The SMR was developed by James Tanner and is the gold standard for documenting pubertal progress worldwide. The clinical and biochemical investigations are deliberately layered: starting with the non-invasive (growth chart, bone age), progressing through hormonal markers (LH, FSH, sex steroids), and reserving the more invasive or expensive tests (GnRH stimulation, brain MRI) for cases where the baseline findings raise sufficient concern. This proportionate approach prevents over-investigation of simple constitutional delay while ensuring that a genuine CNS tumour or gonadal failure is not missed. The SMR is the anchor of the physical examination — without it, you cannot determine whether puberty is truly precocious, truly delayed, or simply at the edge of normal.
Provided image
Performing SMR (Tanner staging) in practice:
In girls:
• Breast development (B1–B5): B1 = flat (prepubertal); B2 = breast bud (small mound, first sign of puberty); B3 = breast enlarges, no contour separation; B4 = secondary mound of areola and papilla; B5 = adult breast
• Pubic hair (PH1–PH5): PH1 = none; PH2 = sparse, slightly pigmented, straight hair along labia; PH3 = darker, curlier, more; PH4 = adult type, less quantity; PH5 = adult quantity, medial thigh spread
In boys:
• Genitalia (G1–G5): G1 = prepubertal (testicular volume <4 mL); G2 = testicular enlargement (4–6 mL, first sign); G3 = lengthening of phallus; G4 = increased breadth, glans development; G5 = adult size
• Pubic hair: same PH1–PH5 scale
• Testicular volume measured with a Prader orchidometer (a string of oval beads from 1–25 mL)
The growth chart is essential: PP children are tall for age (advanced bone age accelerates growth early), while delayed puberty children are short for age with delayed bone age. Bone age (left hand/wrist radiograph, Greulich-Pyle atlas): advanced >2 SD = PP; delayed = CDGP or hypogonadism.
Investigations for precocious puberty:
• Serum LH and FSH: elevated (pubertal) = central PP; suppressed = peripheral PP
• Serum estradiol (girls) or testosterone (boys)
• GnRH stimulation test: give GnRH analogue → peak LH >5 IU/L = pubertal response = central PP confirmed
• Serum 17-OHP (if CAH suspected in virilised child)
• Brain MRI — mandatory in boys with PP and in any child with neurological symptoms; in girls, recommended especially if <6 years at onset or atypical features
• Pelvic/abdominal USS: ovarian cysts, adrenal tumours
Investigations for delayed puberty:
• LH, FSH: low or normal = CDGP or central hypogonadism; elevated = primary gonadal failure
• Karyotype if gonadal failure suspected (Turner, Klinefelter)
• Thyroid function, prolactin, IGF-1 (pituitary screen)
• Brain MRI if central cause suspected (Kallmann, craniopharyngioma)
• Bone age: delayed but will catch up = CDGP