Page 2 of 32
PE31.1 | Childhood Tuberculosis Clinical Spectrum — SDL Guide (Part 2)
Extrapulmonary Tuberculosis
Extrapulmonary TB (EPTB) accounts for approximately 20–30% of childhood TB in India and is proportionally more common in younger children. It arises from haematogenous spread or direct lymphatic extension from the primary complex. The major forms are:
1. Peripheral TB lymphadenitis (TBLN): The most common form of EPTB in children. Cervical lymph nodes (posterior triangle, submandibular) are most frequently affected, reflecting lymphatic drainage from the primary focus in the lung apex or direct tonsil/pharyngeal seeding. Nodes are initially firm, discrete, and non-tender — gradually they coalesce, undergo central caseation, and may perforate the deep fascia to form a collar-stud abscess (dumbbell abscess): central caseation → deep abscess → perforation of deep cervical fascia → subcutaneous abscess pointing through the skin. The overlying skin becomes thinned ('cold abscess'). Diagnosis by FNAC (caseous material, epithelioid granulomas, AFB) or excision biopsy.
2. Tuberculous meningitis (TBM): The most severe form of childhood TB, almost exclusively due to haematogenous dissemination. Most common in children under 5 years. The MRC (Medical Research Council) staging grades severity:
• Stage I: alert, oriented, no neurological deficit — best prognosis
• Stage II: altered consciousness, focal neurological signs (cranial nerve palsies VI, III, VII)
• Stage III: coma, severe neurological deficits, hemiplegia — worst prognosis
The child presents with an insidious onset of fever, headache, irritability, vomiting, and neck rigidity. A late presentation shows seizures, cranial nerve palsies, and stupor. Hydrocephalus (communicating type) is a common and serious complication. CSF: lymphocytic pleocytosis (100–500 cells), elevated protein, low glucose (CSF:blood glucose <0.5), and a delicate 'cobweb' clot on standing. AFB smear is positive in only 10–40%.
3. Abdominal tuberculosis: Involves the ileocaecal region (most common site, reflecting lymphoid tissue abundance), mesenteric lymph nodes, peritoneum, and occasionally solid organs. Presents with fever, abdominal pain, alternating constipation/diarrhoea, a palpable mass in the right iliac fossa, and ascites (straw-coloured, exudate, lymphocyte-dominant, ADA elevated). Complications include intestinal obstruction, perforation, and fistula.
4. Osteoarticular TB (Pott's disease): M. tuberculosis seeds the vertebral bodies by haematogenous spread, preferentially involving the lower thoracic and thoracolumbar vertebrae (richest blood supply). Anterior disc-space infection leads to vertebral body destruction and anterior wedge collapse → gibbus deformity (acute kyphotic angulation). Cold paravertebral abscess can track along fascial planes to present as a fluctuant psoas abscess in the groin. Neurological compromise (paraplegia = Pott's paraplegia) results from cord compression by abscess, granulation tissue, or vertebral debris — a spinal emergency.
| Site | Key Clinical Features | Characteristic Complication |
|---|---|---|
| Cervical lymph nodes | Matted firm nodes, cold abscess | Collar-stud abscess, sinus |
| Meninges (TBM) | Fever, headache, neck rigidity, CN palsies | Hydrocephalus, herniation |
| Ileocaecal/peritoneal | RIF mass, ascites, diarrhoea | Obstruction, perforation |
| Lower thoracic vertebrae (Pott's) | Back pain, gibbus, psoas abscess | Pott's paraplegia |
| Pericardium | Fever, muffled sounds, pulsus paradoxus | Constrictive pericarditis |
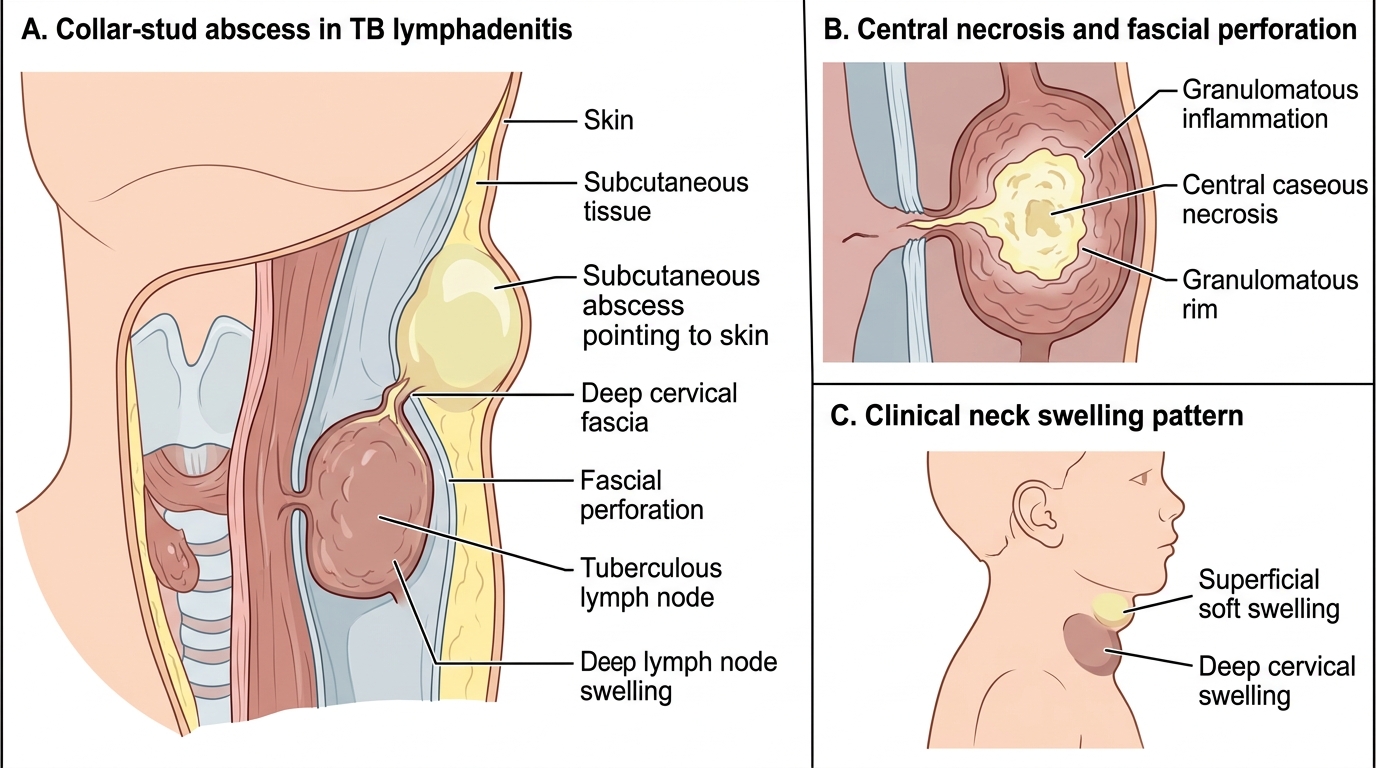
TB Lymphadenitis: Collar-Stud Abscess Formation
CLINICAL PEARL
The three key differences between childhood and adult TB:
1. Children are paucibacillary — their disease is driven less by bacterial load and more by the host immune response to infection; they are rarely infectious to others (except adolescents with cavitary disease).
2. The lymph node component dominates — hilar and mediastinal lymphadenopathy is far more prominent than the parenchymal focus in children, and lymph-node compression is the cause of many paediatric complications (collapse, obstructive hyperinflation).
3. Dissemination is the primary danger — children under 5 have an immature CMI and can rapidly progress from primary complex to miliary TB or TBM; this is the reason BCG vaccination at birth (NIS) is so critical — it reduces the risk of these severe disseminated forms by ~80%.
SELF-CHECK
A 4-year-old boy presents with 3 weeks of fever and neck swelling. Examination shows a right posterior cervical lymph node (3 × 2 cm) that is fluctuant, with a second superficial soft swelling in the skin above it. This appearance is MOST consistent with:
A. Pyogenic cervical lymphadenitis
B. Reactive lymphadenopathy from upper respiratory infection
C. Collar-stud abscess due to TB lymphadenitis
D. Non-Hodgkin lymphoma
Reveal Answer
Answer: C. Collar-stud abscess due to TB lymphadenitis
A collar-stud (dumbbell) abscess is pathognomonic of TB lymphadenitis: the deep caseous abscess perforates the deep fascia to create a secondary subcutaneous component, appearing as two connected fluctuant swellings separated by the fascial plane. Pyogenic lymphadenitis is acutely painful, hot, and erythematous with a shorter duration. Reactive lymphadenopathy is not fluctuant. Lymphoma nodes are firm, non-tender, and rubbery without abscess formation.
Complications and Risk Factors
The complications of childhood tuberculosis arise from three mechanisms: direct tissue destruction by the granulomatous process, pressure effects of enlarging lymph nodes on adjacent structures, and haematogenous dissemination with seeding of distant organs. Complications are more frequent and more severe in younger children and in those with co-morbidities, particularly malnutrition and HIV infection. Because the paediatric primary complex centres on hilar lymph nodes rather than parenchymal cavitation, a distinctive and age-specific set of complications emerges that is rarely seen in adult TB — airway compression, obstructive collapse, and hypersensitivity-driven pleural effusion. Understanding each complication in terms of its underlying pathological mechanism allows the clinician to anticipate risk, monitor for early signs, and intervene before clinical deterioration becomes irreversible damage.
Pulmonary complications:
• Obstructive collapse/hyperinflation — enlarged hilar nodes compress a bronchus; the classic radiological sign is the 'peanut' shape (lymph-node mass with adjacent collapse)
• Bronchial stenosis and bronchiectasis — late sequelae of healed TB with scar contracture
• Empyema — secondary infection of a TB pleural effusion
• Haemoptysis — rare in children; more common in adolescents with cavitary disease
Disseminated complications:
• Miliary TB — bilateral haematogenous seeding of lungs and other organs (liver, spleen, bone marrow); high mortality without treatment
• TBM — the most feared complication; neurological sequelae (hydrocephalus, deafness, cortical blindness, motor deficits) are permanent in survivors of Stage II/III disease
• Pott's paraplegia — spinal cord compression by paravertebral abscess or vertebral collapse
Factors determining severity:
| Risk Factor | Mechanism | Effect |
|---|---|---|
| Age <2 years | Immature CMI, small bronchial lumen | Rapid progression, miliary/TBM |
| Malnutrition (SAM) | Impaired macrophage and T-cell function | Progression to active disease |
| HIV co-infection | CD4+ T-cell depletion | Rapid dissemination, drug resistance |
| Measles | Transient immunosuppression | TB activation in endemic areas |
| No BCG | Absent innate protection | Increased risk miliary/TBM |
| Close household contact | High inoculum, repeated exposure | Higher infection and disease risk |
Immune reconstitution inflammatory syndrome (IRIS) can occur when HIV-infected children start antiretroviral therapy (ART) during TB treatment — a paradoxical worsening of TB symptoms due to immune recovery. This is managed by continuing both treatments; steroids may be needed for life-threatening IRIS.
With prompt, adequate treatment (NTEP-recommended regimens), the majority of children with uncomplicated pulmonary TB recover completely. However, miliary TB and TBM carry mortality of 15–30% even with treatment, and surviving Stage III TBM frequently has permanent neurological deficits. Early diagnosis and treatment initiation are therefore the most powerful determinants of outcome in childhood TB.
SELF-CHECK
Which of the following combinations of features is MOST characteristic of miliary tuberculosis in a 1-year-old child?
A. Right hilar lymphadenopathy with a right lower lobe infiltrate
B. Bilateral 1–2 mm nodular opacities uniformly distributed throughout both lung fields
C. Unilateral pleural effusion with lymphocytic exudate
D. Anterior wedge collapse of a thoracic vertebra with paravertebral shadow
Reveal Answer
Answer: B. Bilateral 1–2 mm nodular opacities uniformly distributed throughout both lung fields
Miliary TB results from haematogenous dissemination producing uniformly distributed millet-seed-sized (1–2 mm) nodular opacities bilaterally on CXR — the defining radiological pattern. Option A describes the primary complex. Option C describes primary tuberculous pleural effusion. Option D describes Pott's disease (vertebral TB with paravertebral abscess).
Self-Assessment
The following self-assessment questions are designed to test your ability to synthesise knowledge across the entire clinical spectrum of childhood TB — from the molecular pathogenesis of the primary complex through to the recognition and prognostication of disseminated disease. Work through each question using the framework from this module: epidemiology and risk, pathogenesis, pulmonary forms, extrapulmonary forms, and complications. Where a clinical scenario is presented, apply the structured approach — identify the syndrome, recall the underlying pathogenesis, reason through the differential, and state your conclusion with supporting evidence. Practising this reasoning pattern now will prepare you for the NMC competency-based assessments that test integration across knowledge domains, not isolated recall. Answers should draw on Ghai, Nelson, and IAP guidelines rather than approximation.
- A 3-year-old with a TB contact presents with fever and right hilar lymphadenopathy on CXR. Explain the pathogenesis of this radiological finding and list the complications that may ensue if the lymph node continues to enlarge.
- Compare and contrast pulmonary and extrapulmonary TB in terms of frequency in different age groups, paucibacillary nature, and risk of infectivity.
- List five risk factors that increase the probability of a child progressing from primary TB infection to active TB disease, and explain the biological mechanism for each.
- A 2-year-old presents with 2 weeks of fever, increasing irritability, and vomiting. On examination she has neck rigidity. CSF examination: 300 cells (lymphocytes), protein 120 mg/dL, glucose 20 mg/dL (blood glucose 80 mg/dL). Apply MRC staging to this presentation and predict the likely complications.
- Why does BCG vaccination at birth significantly reduce miliary TB and TBM in infants but provide less protection against pulmonary TB in older children?