Page 13 of 32
PE31.10 | Exanthematous Illnesses — SDL Guide
Learning Objectives
- Recognise the distinctive prodrome and rash morphology of common childhood exanthematous illnesses including measles, rubella, chickenpox, roseola, erythema infectiosum, hand-foot-mouth disease, and scarlet fever
- Explain the pathogenesis linking viral or bacterial infection to fever and skin eruption
- Identify clinically important complications including SSPE, congenital rubella syndrome, and varicella secondary infections
- Describe the management of each exanthem including specific therapies (vitamin A for measles, acyclovir for varicella) and prevention through vaccination
INSTRUCTIONS
Exanthematous illnesses — fevers with rashes — are among the most visually distinctive diagnoses in paediatrics. Despite effective vaccines, measles still causes preventable deaths in under-immunised populations, and chickenpox can be life-threatening in immunocompromised children. This module equips you to recognise each exanthem at the bedside, avoid dangerous look-alike misdiagnoses, counsel families on complications, and apply the National Immunization Schedule effectively.
References
- Ghai Essential Pediatrics, 9th ed, Ch 10 — Infectious Diseases (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 267-275 — Viral Exanthems (textbook)
- WHO Measles and Rubella Surveillance and Immunization Guidelines, 2023 (guideline)
- IAP Immunization Timetable and National Immunization Schedule, India 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy from a rural community presents with three days of high fever, runny nose, red eyes, and a harsh cough. Today his mother noticed small white spots inside his mouth, and a red rash that began behind his ears and is now spreading down his face and neck. In the waiting room, you also see a 7-year-old with scattered fluid-filled blisters on her trunk — some fresh and clear, others crusted — alongside a feverish 2-year-old with painful ulcers in her mouth and small blisters on her palms and soles. Three children, three different exanthems, one busy clinic. Can you tell them apart?
WHY THIS MATTERS
Exanthematous illnesses remain a major cause of fever with rash in Indian children, especially in communities with incomplete vaccination coverage. Measles causes more than 100,000 deaths per year globally — mainly from preventable complications like pneumonia and encephalitis. Missing a case of measles in a clinical setting can spark an outbreak; missing congenital rubella can devastate an unborn child's development. Conversely, overcalling chickenpox can delay recognition of a drug eruption or dengue rash. The ability to accurately diagnose these conditions, counsel about complications, and implement appropriate public health responses is a core competency for every practising physician in India.
RECALL
Before proceeding, retrieve your foundational knowledge: from Pathology/Microbiology, recall that viruses causing exanthems replicate at the site of entry (respiratory tract), enter the bloodstream (primary viraemia), and seed skin and other organs (secondary viraemia) — the rash marks this systemic immune response. From Anatomy, recall rash morphology terms: a macule is a flat colour change; a papule is a raised solid lesion <1 cm; a vesicle is a fluid-filled blister <1 cm; a pustule is a pus-filled blister. From the National Immunization Schedule, recall that MMR is given at 9–12 months and boosted at 16–24 months, protecting against measles, mumps, and rubella. Varicella vaccine is recommended at 15 months as a two-dose schedule by IAP.
Clinical Presentation and Recognition of Exanthematous Illnesses
Exanthematous illnesses are unified by fever preceding or accompanying a skin eruption, but each exanthem has a distinctive signature that allows clinical differentiation at the bedside. The sequence of prodrome, rash onset, rash morphology, and distribution pattern constitutes the clinical fingerprint of each disease.
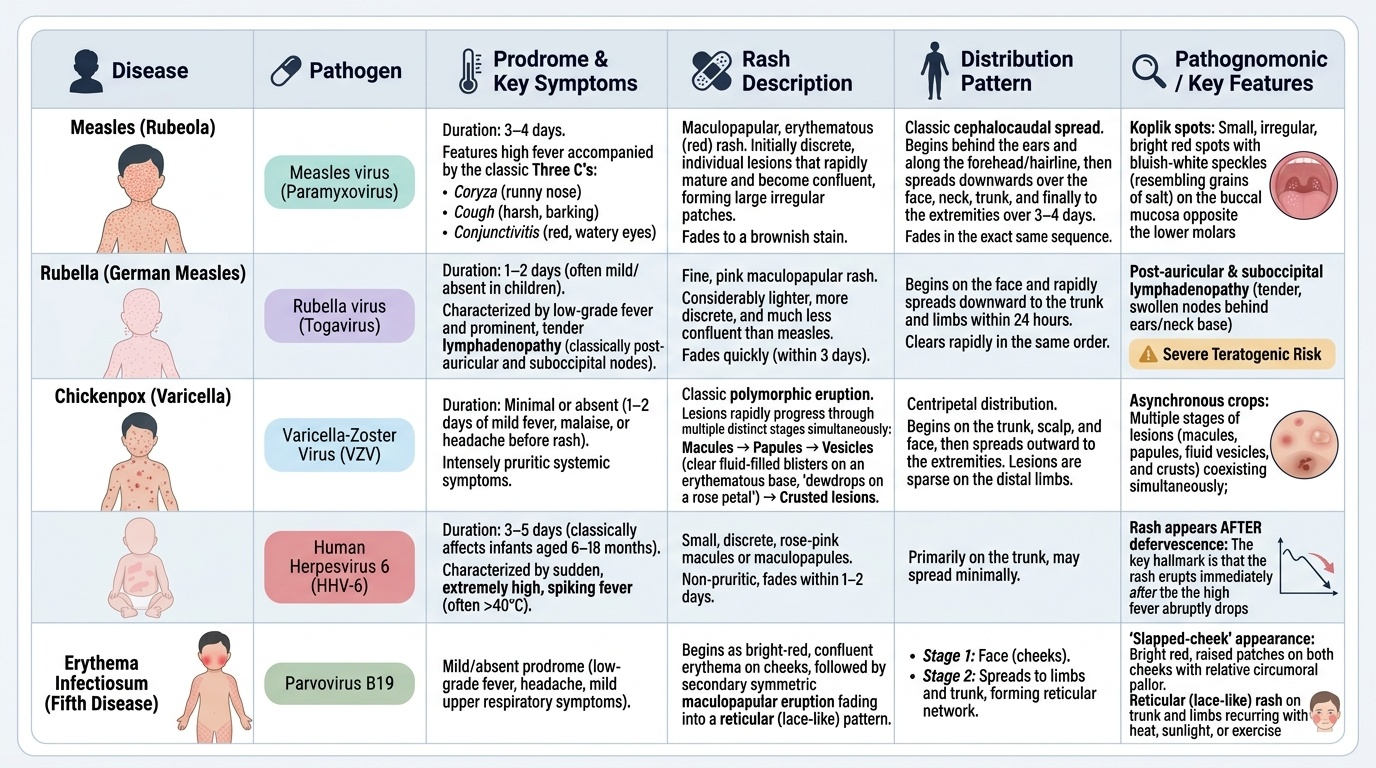
Provided image
Measles (rubeola) begins with a 3–4-day prodrome of the three C's: coryza (runny nose), cough (harsh, barking), and conjunctivitis (red, watery eyes), accompanied by high fever. The pathognomonic sign — Koplik spots — appears 1–2 days before the rash as white, grain-of-salt-like lesions on the buccal mucosa opposite the lower molars. The maculopapular rash then erupts behind the ears and on the forehead, spreading in a cephalocaudal (head-to-toe) direction over 3–4 days before fading in the same sequence. The child is most infectious during the prodromal phase and for 4 days after rash onset.
Rubella (German measles) is characterised by a milder prodrome of low-grade fever and lymphadenopathy — classically post-auricular and suboccipital nodes, which are enlarged and tender. The fine, pink maculopapular rash begins on the face and spreads downward within 24 hours, fading over 3 days ('3-day measles'). The rash is lighter and less confluent than measles, and the child is generally not very unwell — this mild presentation in children contrasts dangerously with its devastating teratogenic potential in early pregnancy.
Chickenpox (varicella) is recognisable by simultaneous crops of lesions at different stages — this polymorphic appearance (macules, papules, vesicles, and crusts coexisting) on the trunk and face is virtually diagnostic. The rash is intensely pruritic. New crops appear over 5–7 days; the child is infectious from 2 days before the rash appears until all lesions are crusted (typically 5–7 days after rash onset).
Roseola infantum (exanthem subitum, HHV-6) classically affects infants aged 6–18 months with 3–5 days of high, spiking fever — the child often appears remarkably well despite the high temperature. When the fever breaks, a blotchy, rose-pink maculopapular rash appears on the trunk and spreads briefly to the face and limbs. The key diagnostic clue is that the rash appears AFTER the fever resolves.
Erythema infectiosum (fifth disease, parvovirus B19) is recognised by the 'slapped-cheek' appearance — intense erythema of both cheeks, sparing the nasal bridge and perioral area. This is followed by a lacy, reticular ('fishnet') rash on the limbs and trunk that may recur with heat, exercise, or sun exposure for weeks. The child typically feels well by the time the rash appears.
Hand-foot-mouth disease (HFMD, coxsackievirus A16 most commonly) causes small, painful ulcers in the mouth (resembling aphthous ulcers) and vesicles on the palms, soles, and sometimes buttocks — the distribution is the diagnostic key. Fever is mild. Drooling and refusal to eat result from the oral pain.
Scarlet fever (Group A Streptococcus) follows pharyngitis with a fine, diffuse, erythematous rash described as 'sandpaper' texture — blanching on pressure. It begins on the trunk and spreads to the limbs, sparing the face (which shows circumoral pallor). Characteristic features include strawberry tongue (white coating with red papillae initially, becoming bright red by day 4–5) and Pastia lines (petechiae in skin folds — antecubital fossa, inguinal creases). The rash desquamates after 1–2 weeks.
SELF-CHECK
A 2-year-old has had high fever for 4 days. Today the fever has suddenly resolved, and a pink maculopapular rash has appeared on the trunk. She appears well and playful. Which diagnosis is MOST likely?
A. Measles
B. Roseola infantum (HHV-6)
C. Rubella
D. Erythema infectiosum
Reveal Answer
Answer: B. Roseola infantum (HHV-6)
Roseola infantum (HHV-6) classically presents in infants 6–18 months with high fever lasting 3–5 days, during which the child often appears well. The rash appears on the trunk AFTER the fever resolves — this post-febrile rash is pathognomonic. Measles has a prodrome of cough/coryza/conjunctivitis before the rash. Rubella is milder with post-auricular nodes. Erythema infectiosum (parvovirus B19) causes the 'slapped cheek' appearance.
Pathogenesis and Aetiology
Understanding the pathogenesis of exanthematous illnesses illuminates why each disease produces its characteristic clinical picture — the rash is not merely a surface phenomenon but a visible marker of viral or immune-mediated processes occurring throughout the body.
Measles is caused by a single-stranded RNA paramyxovirus transmitted by respiratory droplets — one of the most contagious pathogens known (basic reproduction number R₀ = 12–18). The virus enters via the respiratory mucosa, infects dendritic cells and alveolar macrophages, and spreads via primary viraemia to lymphoid tissue (causing lymphoproliferation and the characteristic cough). During secondary viraemia, the virus seeds the skin, causing the characteristic rash through two mechanisms: direct viral cytopathic effect on keratinocytes and the inflammatory immune response. Koplik spots represent necrotic foci in buccal mucosa caused by local viral replication before systemic spread. The measles virus causes profound immunosuppression for 2–3 years post-infection ('immune amnesia'), explaining the paradox that a child who has recovered from measles becomes more vulnerable to other infections.
Rubella virus (togavirus, genus Rubivirus) produces a mild exanthem in children through a similar viraemic mechanism. Its primary pathological impact is on the developing fetus, where it disrupts organogenesis during critical windows — the earlier the infection, the more severe and widespread the damage (congenital rubella syndrome).
Varicella-zoster virus (VZV, a herpesvirus) is transmitted by both respiratory droplets and direct contact with vesicle fluid. After primary replication in the nasopharynx, the virus infects T-lymphocytes, achieves viraemia, and seeds the skin — producing the characteristic crops of lesions as successive waves of viraemia deliver virus to different skin sites. VZV then establishes latency in the dorsal root ganglia and cranial nerve ganglia, where it may reactivate decades later as herpes zoster (shingles).
HHV-6 (roseola) infects CD4+ T-lymphocytes and monocytes. The prolonged high fever results from direct viral cytopathic effects and cytokine release (IL-1, IL-6, TNF). When the immune response clears the viraemia, the fever resolves — and the transient rash reflects the immune complex deposition rather than active viral replication in skin.
Parvovirus B19 (erythema infectiosum) infects erythroid progenitor cells expressing the P antigen (the viral receptor). In healthy individuals, the aplastic crisis is brief and self-limiting, but in those with haemolytic anaemia (sickle cell disease, spherocytosis), B19 infection causes aplastic crisis — sudden severe anaemia from red cell precursor destruction. The 'slapped cheek' rash and subsequent reticular rash are immune-complex mediated and appear when the patient is no longer infectious.
Coxsackievirus A16 (HFMD) is an enterovirus that replicates in the gut and spreads to the skin and oral mucosa via viraemia, causing the characteristic vesicular eruption on the palms, soles, and oral mucosa. The virus is shed in stool for weeks.
Scarlet fever (Group A Streptococcus, GAS) is caused by pyrogenic exotoxins (SPE-A, B, C) produced by streptococci in the throat. These exotoxins act as superantigens, non-specifically activating large numbers of T cells and driving massive cytokine release — causing the diffuse erythematous rash, fever, and systemic toxicity.
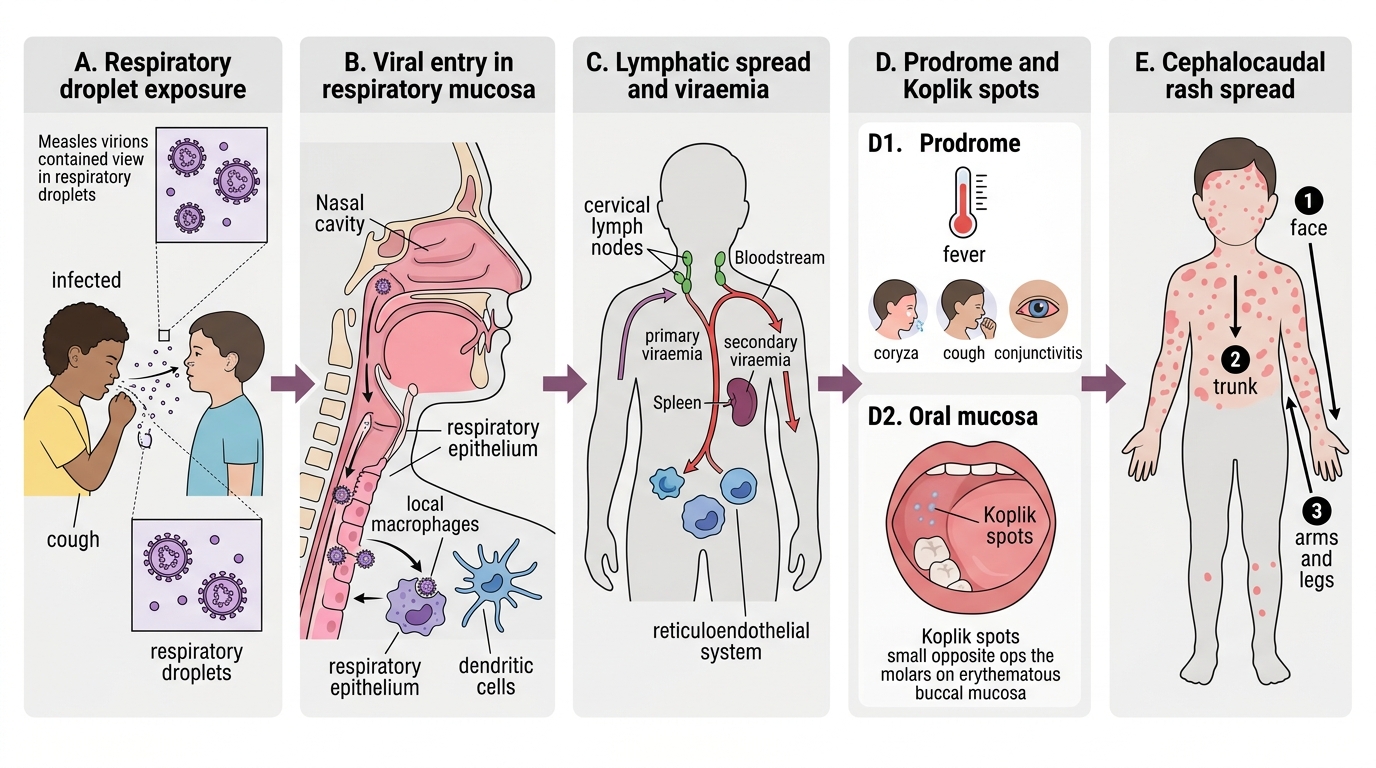
Measles Pathogenesis: From Droplet Entry to Koplik Spots and Rash
Diagnosis and Investigation
Most childhood exanthems are diagnosed clinically based on the combination of prodrome, rash morphology, and distribution — laboratory confirmation is reserved for atypical presentations, outbreak investigation, or clinical uncertainty.
For measles, clinical diagnosis is based on the triad of the three C's (coryza, cough, conjunctivitis) with fever, Koplik spots, and the characteristic cephalocaudal maculopapular rash. Laboratory confirmation for public health surveillance uses IgM serology (measles-specific IgM detectable from day 3 of rash for up to 4 weeks) or PCR of throat swab/urine. Koplik spots, though pathognomonic, are present only briefly and may be missed if not specifically sought. Complications are suggested by persistent or worsening symptoms after the rash appears.
For rubella, clinical diagnosis is supported by the combination of mild prodrome, post-auricular and suboccipital lymphadenopathy, and a rapidly fading maculopapular rash. Serological confirmation (rubella IgM or a 4-fold rise in IgG) is essential in pregnant women exposed to rubella and for congenital rubella diagnosis. Congenital rubella is confirmed by IgM in the neonate or viral isolation from throat/urine.
Chickenpox diagnosis is almost always clinical — the polymorphic rash (simultaneous crops at multiple stages) on the trunk is virtually pathognomonic. In atypical cases (immunocompromised, disseminated, or severe disease), Tzanck smear (shows multinucleated giant cells from vesicle base scrapings — not specific for VZV; also positive for HSV) or PCR of vesicle fluid confirms VZV. Blood counts may show relative lymphocytosis.
For roseola, the diagnosis is retrospective — the clinical pattern of high fever followed by post-febrile rash is sufficient. No routine laboratory testing is indicated in healthy children; the concern is that during the febrile phase (before the rash), the child may present as a fever-without-source, necessitating evaluation for meningitis in younger infants.
Erythema infectiosum is a clinical diagnosis in otherwise healthy children with the slapped-cheek rash and lacy reticular limb rash. In at-risk populations — pregnant women (risk of fetal hydrops from B19-induced fetal anaemia) and those with haemolytic anaemia (risk of aplastic crisis) — parvovirus B19 IgM/PCR is indicated.
HFMD is diagnosed clinically by the combination of fever, oral ulcers, and vesicles on palms/soles. Enterovirus PCR from stool, throat, or vesicle fluid is available but rarely necessary for typical cases.
Scarlet fever requires a throat swab for Group A Streptococcal culture or rapid antigen detection (RADT). ASO (antistreptolysin O) titres confirm recent streptococcal infection in post-streptococcal complications (rheumatic fever, glomerulonephritis).