Page 11 of 32
PE31.9 | Fever Approach — SDL Guide (Part 2)
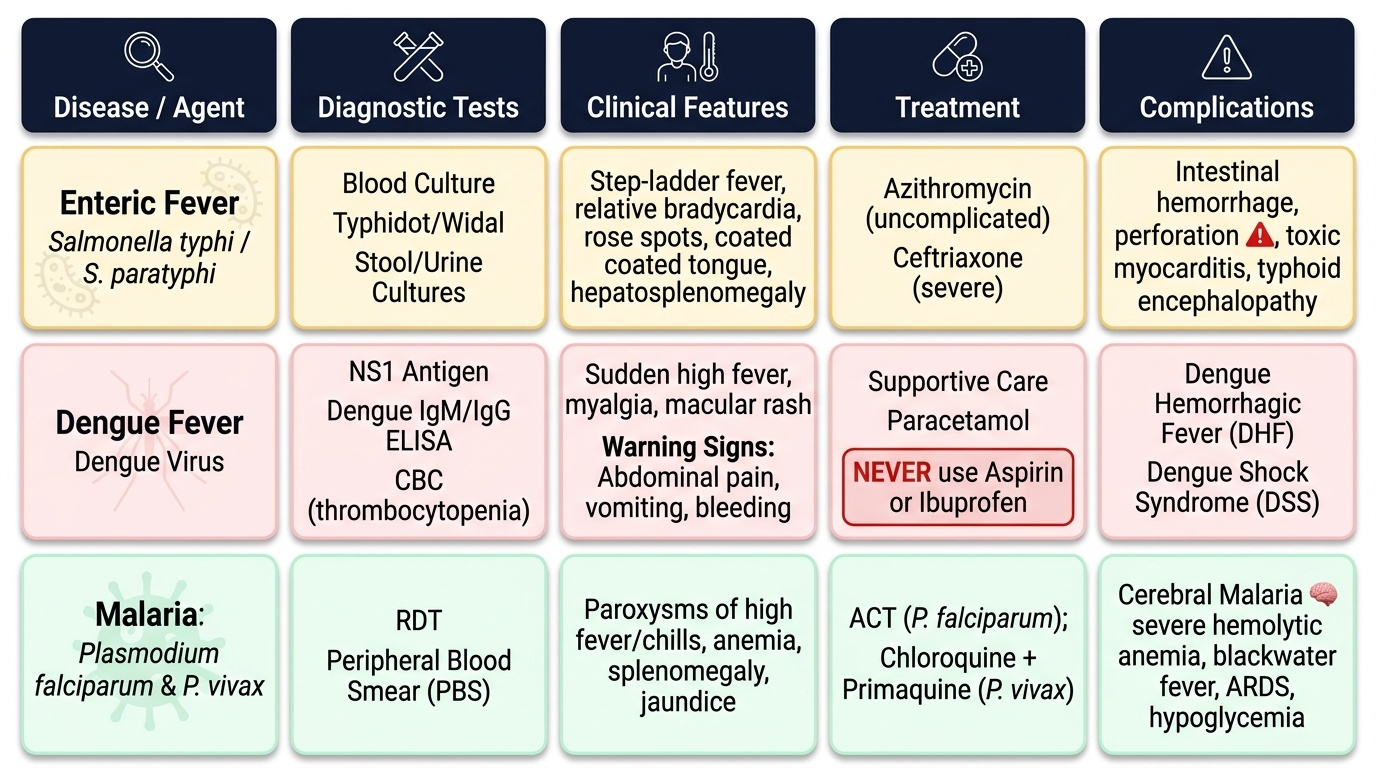
Management of Common Fever Causes
Management of fever in children follows two parallel and equally important tracks that must run simultaneously from the moment of diagnosis. The first track is symptomatic treatment — reducing the temperature to prevent febrile seizures and distress, and maintaining adequate hydration. The second track is cause-specific treatment directed at the underlying organism, guided by the diagnostic conclusions reached in the investigation step. Treating fever only with paracetamol, without identifying and targeting the causative organism, is inadequate and potentially dangerous care: it may temporarily make the child appear well while the underlying infection progresses to a life-threatening complication. In dengue, enteric fever, and severe malaria, the window for effective intervention is narrow, and symptomatic management alone buys time but does not treat the disease.
Provided image
Symptomatic management (all causes):
• Paracetamol (acetaminophen): 15 mg/kg/dose every 4–6 hours; maximum 5 doses/24 h; safe in most infections including dengue (NEVER aspirin or ibuprofen in dengue — risk of haemorrhage and Reye's syndrome). Paracetamol is the first-line antipyretic in all children.
• Tepid sponging: Lukewarm water sponging helps dissipate heat; cold water causes vasoconstriction and shivering which paradoxically increases core temperature — use only lukewarm water.
• Adequate hydration: Ensure adequate oral fluid intake; monitor urine output.
Enteric fever (Salmonella typhi):
Ceftriaxone 75 mg/kg/day IV (max 4 g/day) ×10–14 days is the current first-line treatment in hospitalised or severe cases. Azithromycin 10–20 mg/kg/day oral ×7 days is first-line for uncomplicated enteric fever, particularly with fluoroquinolone and ampicillin resistance now widespread in India. Chloramphenicol, ampicillin, and fluoroquinolones are used where sensitivity is confirmed. Complications to watch: intestinal haemorrhage (fresh rectal bleed, pallor), intestinal perforation (acute abdomen, peritonitis, septic shock — surgical emergency), toxic myocarditis, neurological complications (typhoid encephalopathy). Dexamethasone 3 mg/kg IV stat + 1 mg/kg 6-hourly × 8 doses is used for severe typhoid encephalopathy.
Dengue:
There is no antiviral treatment for dengue. Management is entirely supportive:
• Without warning signs (dengue fever): Oral hydration, paracetamol, rest; monitor daily CBC; return precautions (any warning sign → immediate return to hospital)
• With warning signs (dengue with warning signs): Hospitalise immediately; IV isotonic crystalloid (normal saline or Ringer's lactate); monitor haematocrit 4–6 hourly; do NOT over-hydrate (risk of pulmonary oedema); titrate fluids to haematocrit stabilisation and urine output ≥1 mL/kg/h
• Dengue shock syndrome (DSS): Rapid IV fluid bolus 10 mL/kg over 15–20 minutes; reassess and repeat if not improving; colloids (dextran 40 or starch) if haematocrit remains high after crystalloids
• Absolute contraindications in dengue: aspirin (anti-platelet + Reye's risk), NSAIDs (gastric bleeding + renal impairment), steroids (not indicated), prophylactic platelet transfusion (only for severe spontaneous bleeding or pre-procedure with platelet <20,000)
Malaria:
• P. falciparum (uncomplicated): Artemisinin-based Combination Therapy (ACT) — artesunate + sulfadoxine-pyrimethamine (AS+SP) or artemether-lumefantrine per NVBDCP drug policy 2023 — is the standard first-line treatment. Weight-based dosing; full 3-day course essential to prevent resistance.
• Severe/cerebral P. falciparum: IV artesunate (preferred over IV quinine per WHO 2015); manage in ICU; monitor blood glucose (hypoglycaemia), haematocrit (transfusion if severe anaemia), seizures, pulmonary oedema.
• P. vivax: Chloroquine for blood-stage (25 mg base/kg over 3 days) + Primaquine (0.25 mg/kg/day × 14 days) to eliminate the hepatic hypnozoite (dormant stage that causes relapse). Primaquine is contraindicated in G6PD deficiency (haemolytic crisis) — test G6PD before prescribing.
FUO management: Empirical treatment should generally be avoided in FUO; treat only when a diagnosis is established. Exceptions: empirical anti-TB therapy when TB is strongly suspected but unconfirmed; empirical antimalarial if smear is repeatedly negative but endemic exposure is certain. Empirical antibiotics for bacterial FUO require a clear diagnostic hypothesis.
SELF-CHECK
A 9-year-old girl has 6 days of fever with relative bradycardia (pulse 72 bpm despite temperature 40°C), rose spots on the abdomen, and soft abdomen with mild distension. Blood culture is pending. The MOST appropriate immediate management is:
A. Empirical azithromycin oral and discharge with follow-up
B. IV ceftriaxone 75 mg/kg/day; admit and monitor for intestinal perforation
C. IV chloramphenicol with close monitoring
D. Paracetamol and rehydration only; await culture results before antibiotics
Reveal Answer
Answer: B. IV ceftriaxone 75 mg/kg/day; admit and monitor for intestinal perforation
This child has clinical enteric fever (step-ladder fever, relative bradycardia despite high temperature — a classic feature of typhoid, rose spots on the abdomen). She is hospitalised with a potentially severe case. The current standard for moderate-severe enteric fever requiring hospitalisation is IV ceftriaxone 75 mg/kg/day for 10–14 days, initiated empirically before culture results. She must be monitored closely for intestinal haemorrhage and perforation — the two most dangerous complications. Discharging on oral azithromycin alone is insufficient for a hospitalised child with fever >5 days and abdominal findings. Awaiting culture before antibiotics delays necessary treatment.
Self-Assessment
The following case-based self-assessment questions integrate the fever approach framework from this module — covering etiopathogenesis, clinical features, investigation selection, and management of fever in children, as required by PE31.9. Each case is representative of real clinical presentations in the Indian paediatric context. Work through the questions using the structured fever approach: identify the fever pattern, apply the clinical decision rules, select the targeted investigation, and state the cause-specific management including key precautions. Pay particular attention to the dengue warning signs (there are 7 — all must be recalled by name), malaria species identification by peripheral smear morphology (the features that distinguish falciparum from vivax are high-yield for examinations and have direct treatment implications), and the specific drug contraindications in dengue that are the most common prescribing error in this disease.
- A 6-year-old child has 7 days of fever with leucopenia, thrombocytopenia (platelets 55,000), haematocrit rising from 34% to 42% over 24 hours, and vomiting. List all applicable dengue warning signs, state the WHO dengue classification, and outline the fluid management strategy.
- A 4-year-old returning from a forest area has intermittent fever with chills every 48 hours. Peripheral smear shows enlarged erythrocytes with Schüffner's dots and large amoeboid trophozoites. Name the species, state the appropriate NVBDCP treatment, and explain why primaquine is given and what precaution is required before prescribing it.
- Define FUO. A 10-year-old has had fever >38.3°C for 3 weeks without a diagnosis after standard investigations. List 5 causes under each category: infectious, autoimmune, and malignant.
- Explain the mechanism of fever using the pyrogen cascade and describe precisely how paracetamol reduces temperature without killing the pathogen.
- Compare the diagnostic value of Widal test versus blood culture in enteric fever. Explain why a single positive Widal titre is insufficient for diagnosis.