Page 19 of 32
PE31.12 | Typhoid — SDL Guide
Learning Objectives
- Describe the clinical progression of typhoid fever by week — stepladder fever, relative bradycardia, rose spots, and systemic features — and recognise the clinical picture of enteric fever
- Explain the pathogenesis of Salmonella Typhi infection from faeco-oral ingestion through Peyer's patch invasion to bacteraemia
- Critically evaluate the role of blood culture (gold standard) versus the Widal test (unreliable in endemic areas) in diagnosis
- Identify the serious complications of typhoid — especially intestinal perforation in the third week — and describe their management
- Select appropriate antibiotic therapy (ceftriaxone for severe/complicated; azithromycin for uncomplicated) and explain prevention through vaccination and safe water/food practices
INSTRUCTIONS
Typhoid (enteric fever) remains one of the most prevalent and clinically challenging febrile illnesses in children in India, causing an estimated 1–6 million cases annually in the country. Its systemic presentation — prolonged fever, abdominal symptoms, and the risk of life-threatening intestinal perforation — makes early diagnosis and appropriate antibiotic selection critical. The Widal test, widely used in India, is notoriously unreliable in endemic populations; understanding why, and knowing when to trust clinical judgment over a laboratory number, is a hallmark of the competent clinician.
References
- Ghai Essential Pediatrics, 9th ed, Ch 10 — Enteric Fever (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 214 — Salmonella Infections (textbook)
- IAP Standard Treatment Guidelines — Typhoid Fever in Children (guideline)
- WHO Position Paper on Typhoid Vaccines, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old girl is brought to your clinic with fever for 10 days. Her mother says the fever has been getting higher each day and does not come down completely, even with paracetamol. Today the child has a headache, feels very tired, and has had loose stools for two days. On examination, her temperature is 39.8°C but her pulse is only 78/min — slower than you would expect for such a high fever. Her abdomen is mildly distended with diffuse tenderness. You notice a faint pinkish rash of a few small spots on her trunk. The Widal test you ordered last week came back positive at 1:80 O and 1:80 H. Is this typhoid — and does the Widal test confirm it?
WHY THIS MATTERS
Typhoid fever affects millions of Indian children every year, disproportionately impacting communities with inadequate sanitation and unsafe drinking water. The prolonged fever, systemic toxaemia, and risk of intestinal perforation make it a clinical emergency when complications supervene. Across India, clinicians must navigate the unreliability of the Widal test — which generates false positives in endemic populations — and the emergence of multidrug-resistant (MDR) Salmonella Typhi strains that render older antibiotics ineffective. The introduction of the Typhoid Conjugate Vaccine (TCV) in the National Immunization Schedule represents a significant public health advance; understanding its role alongside clinical management is essential for the paediatrician.
RECALL
Before proceeding, recall the following: from Microbiology, Salmonella Typhi is a gram-negative, non-spore-forming, facultatively anaerobic rod; it belongs to the Enterobacteriaceae family and is an obligate human pathogen (no animal reservoir for S. Typhi, unlike non-typhoidal Salmonella). It possesses O (lipopolysaccharide), H (flagellar), and Vi (capsular virulence) antigens — these underpin the Widal test and vaccine immunology. From Anatomy, recall Peyer's patches — lymphoid aggregates in the terminal ileum's submucosal layer that serve as portals of entry for S. Typhi. From your general medicine learning, recall that normal heart rate increases by approximately 10–15 beats per minute for every 1°C rise in body temperature — relative bradycardia means the pulse is slower than this expected rise, an important sign in typhoid.
Clinical Presentation of Typhoid (Enteric Fever)
Typhoid fever is a systemic illness that evolves through characteristic weekly stages, each reflecting different phases of the infection's pathophysiology. Recognising the stage of illness at presentation helps the clinician predict complications and choose investigations and management appropriately.
Week 1 — Onset and rising fever:
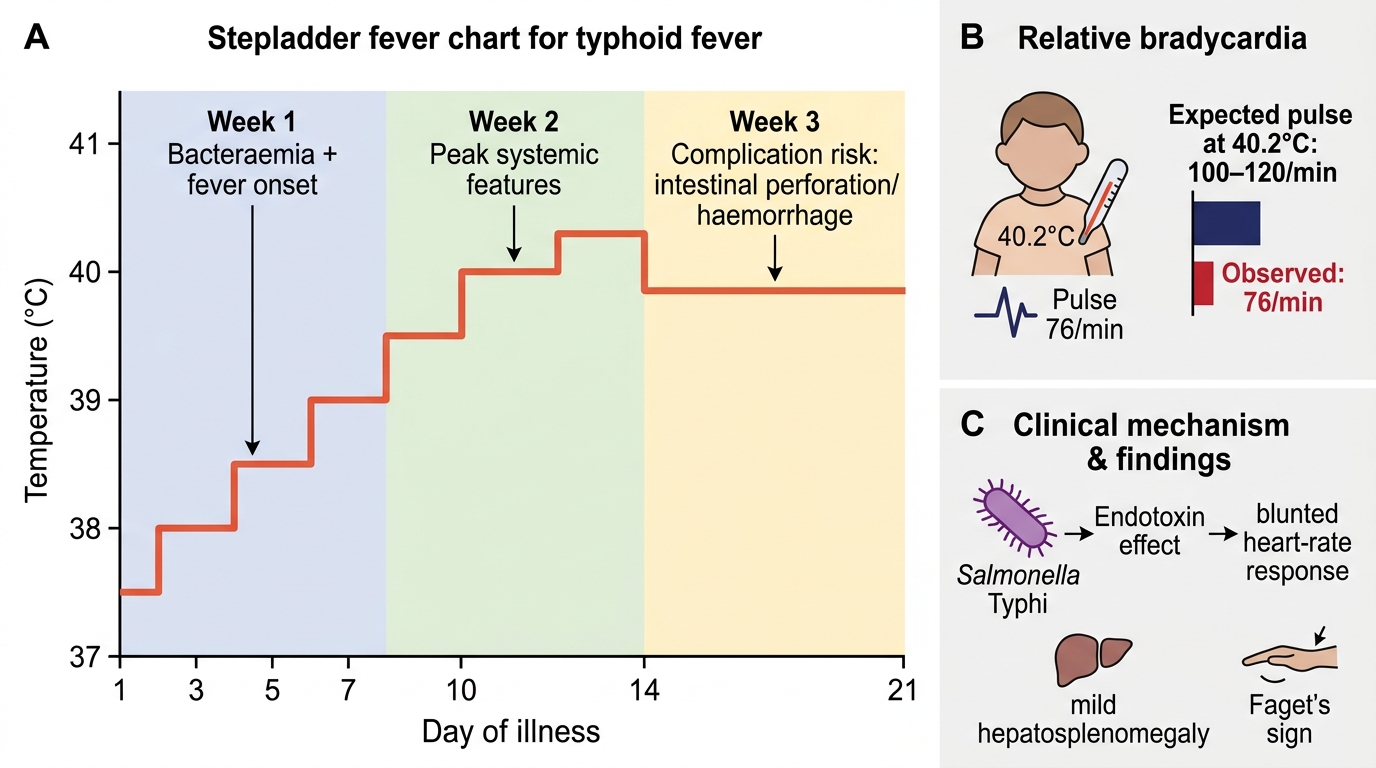
The illness begins insidiously with progressively worsening fever that rises 0.5–1°C each day without returning fully to baseline — the classic stepladder fever pattern. The child complains of headache, malaise, myalgia, and anorexia. Initially constipation is more common than diarrhoea (opposite to most gut infections). The fever is accompanied by a coated tongue and mild abdominal distension. Relative bradycardia (Faget's sign) — the pulse rate being lower than expected for the degree of fever — is a characteristic but inconstant finding (present in about 30–40% of cases).
Week 2 — Peak systemic toxaemia:
Fever is sustained and high (39–40°C). The child appears more unwell: lethargic, anorexic, and may be confused in severe cases (typhoid encephalopathy or 'typhoid state'). Hepatosplenomegaly is detectable in most children. Rose spots — faint, salmon-pink, blanching, macular spots 2–4 mm in diameter — appear on the lower trunk and abdomen in approximately 10–20% of patients; they are transient (lasting 3–5 days), subtle, and easily missed, especially in dark-skinned individuals. Diarrhoea (often 'pea-soup' stools) may now appear as the small bowel is extensively involved.
Week 3 — Complication period:
In untreated or inadequately treated cases, the third week carries the highest risk of intestinal perforation and haemorrhage (from necrosis of Peyer's patches) and the risk of relapse. The fever may begin to defervese spontaneously, but this is also when perforation risk peaks. Any sudden worsening of abdominal pain, distension, or the appearance of peritoneal signs in a child with typhoid should immediately raise the suspicion of perforation.
Paediatric considerations: Children, especially those under 5 years, often present atypically — fever may be the only feature, the stepladder pattern may not be apparent, and the child may present with febrile seizures, hepatitis, or an acute septic picture without the classic systemic features. Typhoid in young children carries higher complication rates.
Stepladder Fever and Faget's Sign in Typhoid
SELF-CHECK
A 10-year-old has had fever for 12 days with a stepladder pattern. His temperature today is 40.2°C but his pulse rate is 76/min. Abdominal examination reveals mild hepatosplenomegaly. Which clinical finding is most characteristic of typhoid fever, and what is its eponymous name?
A. High fever with tachycardia — Osler's triad
B. Fever with a pulse rate lower than expected for the temperature — Faget's sign (relative bradycardia)
C. Fever with hepatosplenomegaly — Weil's disease
D. Stepladder fever with constipation — Trousseau's sign
Reveal Answer
Answer: B. Fever with a pulse rate lower than expected for the temperature — Faget's sign (relative bradycardia)
Relative bradycardia (Faget's sign) is a characteristic finding in typhoid: the pulse rate is lower than expected for the degree of fever. Normally, heart rate increases by approximately 10–15 bpm per 1°C rise in temperature; in typhoid, the vagal-stimulating effect of Salmonella lipopolysaccharide (endotoxin) blunts this response, resulting in a slower-than-expected pulse. At 40.2°C, the expected pulse would be 100–120/min; finding 76/min is a significant relative bradycardia. While not universally present (found in ~30–40% of cases), it is a useful supporting clinical sign when present.
Pathogenesis and Aetiology
The pathogenesis of typhoid fever follows a precise sequence from ingestion to systemic bacteraemia, and each step helps explain the clinical features and their timing throughout the illness.
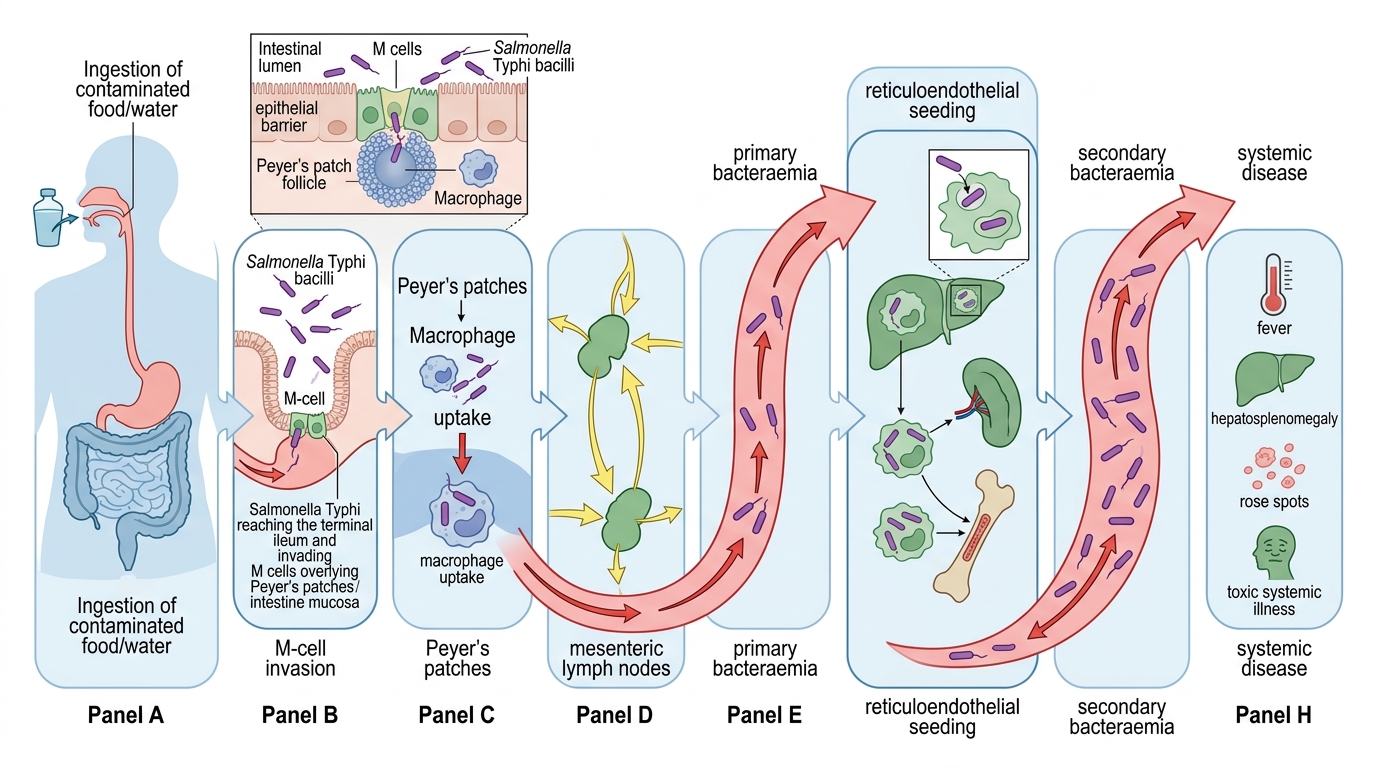
Transmission and inoculum: Salmonella Typhi is transmitted exclusively via the faeco-oral route — contaminated water, food, or direct hand-to-mouth contact with infected material. The infective dose is relatively low (as few as 10³–10⁶ organisms), and S. Typhi can survive in water, ice cream, shellfish, and vegetables for weeks. Unlike non-typhoidal Salmonella, S. Typhi has no animal reservoir — humans are the sole source of infection. Chronic carriers (particularly those with biliary disease) are an important reservoir, excreting the organism in stool or urine for over 1 year after acute infection.
Intestinal invasion and primary bacteraemia: After surviving gastric acid (aided by its Vi antigen, which inhibits complement activation and phagocytosis), S. Typhi reaches the small intestine, where it is selectively taken up by M cells (specialised antigen-sampling epithelial cells) overlying Peyer's patches in the terminal ileum. Within Peyer's patches, S. Typhi is engulfed by macrophages but resists intracellular killing (using the type III secretion system to manipulate the phagosome environment). This begins the incubation period of 7–14 days during which the bacteria multiply silently in mesenteric lymph nodes — explaining the absence of symptoms at this stage.
Secondary bacteraemia and systemic dissemination: The bacteria then spill into the thoracic duct and enter the bloodstream — primary bacteraemia — and seed the reticuloendothelial system (liver, spleen, bone marrow). After a period of intracellular multiplication, a massive secondary bacteraemia occurs, which corresponds to the onset of clinical illness: fever, headache, and systemic toxaemia. The lipopolysaccharide (LPS/endotoxin) of S. Typhi drives the systemic inflammatory response responsible for the fever, hepatosplenomegaly, and relative bradycardia.
Peyer's patch pathology and complications: The ongoing infection causes progressive hyperplasia (week 1) → necrosis (week 2) → sloughing (week 3) of Peyer's patches in the terminal ileum. In week 3, the denuded patches may ulcerate through the bowel wall, causing intestinal perforation and peritonitis, or erode blood vessels causing intestinal haemorrhage. The rose spots on the trunk represent embolic foci of S. Typhi bacteria in the skin's capillaries — each spot is a tiny area of dermal bacteraemia.
Pathogenesis of Salmonella Typhi
Diagnosis and Investigation
Accurate diagnosis of typhoid requires understanding the performance characteristics of available tests — particularly why the Widal test, while widely used in India, is not reliable as the sole basis for diagnosis in endemic settings. The gold standard is blood culture, and clinical judgment must drive management decisions when laboratory results are equivocal. A central principle in typhoid diagnosis is that no single test — positive or negative — should be used in isolation. The clinical picture (week of illness, fever pattern, hepatosplenomegaly, leucopenia, rose spots) remains the foundation; investigations confirm or refine the diagnosis. In a district hospital setting where laboratory infrastructure is limited, a well-reasoned clinical diagnosis supported by a consistent blood count and epidemiological context is sufficient to initiate treatment without waiting for bacteriological confirmation.
Blood culture — the gold standard:
Blood culture is the most specific diagnostic test for typhoid. Sensitivity is highest in the first week of illness (60–80%) when bacteraemia is at its peak, and falls thereafter as the bacteria become sequestered in macrophages. Key points:
- Collect at least 5–10 mL of blood (larger volumes increase yield in children)
- Two to three sets from different sites maximise sensitivity
- Culture on MacConkey agar and blood agar; S. Typhi produces characteristic non-lactose-fermenting colonies
- Culture report takes 3–5 days; antibiotic sensitivity testing follows
- A negative blood culture does NOT exclude typhoid (false negatives common if antibiotics have been started, or disease is >1 week old)
Widal test — significant limitations in endemic areas:
The Widal test measures agglutinating antibodies against S. Typhi O (somatic, lipopolysaccharide) and H (flagellar) antigens. In non-endemic populations, a fourfold rise in titre between acute and convalescent sera, or a single titre of ≥1:160 (O) or ≥1:160 (H), is considered significant. However, in endemic populations like India, the Widal test is notoriously unreliable:
- Background titres are elevated in many healthy individuals (prior exposure or subclinical infection)
- Cross-reactions with other Salmonella species, malaria, dengue, hepatitis, and other febrile illnesses produce false positives
- Prior typhoid vaccination raises H titres without active infection
- Titres may not rise until week 2–3 of illness, missing early disease
- The IAP and most infectious disease experts recommend NOT relying on a single Widal test for diagnosis; it should be interpreted only in clinical context
Alternative laboratory tests:
- Bone marrow culture: highest sensitivity (>90%) even after antibiotic treatment; invasive, reserved for clinically suspected typhoid with repeatedly negative blood cultures
- Typhidot (typhoid-specific IgM/IgG ELISA): more specific than Widal for acute infection; IgM positivity suggests active infection; limitations with cross-reactivity persist
- Tube Widal or card Widal: card (rapid) format is less reliable than standard tube Widal
- Blood counts: characteristically show leucopenia (WBC 2,000–6,000/µL) with relative lymphocytosis — a helpful supporting finding (differentiates from pyogenic bacterial infections which cause leucocytosis)
- Liver enzymes: often mildly elevated (2–3× normal) in typhoid hepatitis
- Stool and urine cultures become positive later in the illness but are less sensitive than blood culture