Page 22 of 32
PE31.13 | Vector Borne Fever — SDL Guide
Learning Objectives
- Differentiate dengue, chikungunya, malaria, and scrub typhus at the bedside based on fever pattern, clinical signs, and vector history
- Identify dengue warning signs (WHO 2009) and recognise severe dengue requiring urgent fluid resuscitation
- Select appropriate diagnostic tests by day of illness for dengue (NS1 vs IgM), and by clinical context for malaria (blood smear/RDT) and scrub typhus
- Prescribe evidence-based treatment: dengue fluid management without aspirin/NSAIDs; ACT for falciparum malaria; chloroquine + primaquine (after G6PD testing) for vivax; doxycycline for scrub typhus
- Counsel on vector control measures for Aedes and Anopheles mosquitoes
INSTRUCTIONS
Vector-borne fevers are among the most common causes of febrile illness in Indian children, collectively responsible for millions of cases annually. Dengue alone causes an estimated 33 million symptomatic infections per year in India; malaria remains a leading cause of paediatric mortality in tribal and forest-dwelling communities; and scrub typhus is an under-recognised cause of fever with rash that responds dramatically to doxycycline if diagnosed. The ability to distinguish these diseases clinically, order the right test at the right time, and avoid dangerous medications (aspirin in dengue; primaquine in G6PD deficiency) is a fundamental paediatric competency.
References
- Ghai Essential Pediatrics, 9th ed, Ch 10 — Vector-Borne Diseases (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 272 — Dengue; Ch 246 — Malaria (textbook)
- WHO Dengue Guidelines for Diagnosis, Treatment, Prevention and Control, 2009 (guideline)
- National Drug Policy for Malaria, NVBDCP, India, 2023 (guideline)
- IAP Standard Treatment Guidelines — Dengue Fever in Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Four children arrive at your paediatric OPD in monsoon season. The first — a 9-year-old — has had 5 days of high fever, severe headache, and eye pain; today she has abdominal pain and has vomited three times. Her platelet count is 45,000/µL and rising haematocrit. The second — a 7-year-old — has joint pains so severe he refuses to walk; his knees and ankles are swollen and tender; fever started 4 days ago. The third — a 5-year-old from a forest area — has spiking fever every 2 days, shaking chills, and a large spleen. The fourth — an 8-year-old — has fever, headache, and a painless black scab on her axilla that she says appeared before the fever. Same monsoon, same district, four completely different diseases. The treatment for each is different — and giving the wrong drug can be fatal.
WHY THIS MATTERS
Vector-borne fevers account for a substantial proportion of febrile illness admissions in India's tertiary and district hospitals, particularly during and after the monsoon season when vector populations peak. Dengue is now endemic in urban and semi-urban India across all states; malaria disproportionately affects children in tribal belts, forest areas, and high-transmission districts; chikungunya epidemics arise periodically in coastal and urban areas; and scrub typhus is an increasingly recognised cause of fever of unknown origin in northern and peninsular India. Misdiagnosis carries real danger: giving aspirin or NSAIDs to a dengue patient can precipitate haemorrhage; giving primaquine to a G6PD-deficient child can cause life-threatening haemolytic anaemia; missing scrub typhus means withholding a curative antibiotic. Accurate diagnosis and appropriate management of vector-borne fevers is not just a clinical skill — it is a public health imperative.
RECALL
Before proceeding, recall the following foundational knowledge: from Microbiology, recall that dengue virus is a flavivirus with four serotypes (DENV 1–4), and that infection with one serotype produces lifetime immunity to that serotype but may worsen a subsequent infection with a different serotype (antibody-dependent enhancement). Recall that Plasmodium completes its sexual cycle in the Anopheles mosquito (sporogony) and its asexual cycle in the human host (schizogony — first in the liver, then in red blood cells). From Biochemistry, recall that G6PD deficiency is an X-linked enzyme deficiency that causes haemolytic anaemia when the red cell is exposed to oxidative stress — primaquine is a potent oxidant and must never be given without G6PD testing. From Pharmacology, recall that artemisinin derivatives (artesunate, artemether) act on all stages of the erythrocytic cycle of Plasmodium and have the fastest parasite-clearance rate of any antimalarial.
Clinical Presentation of Vector-Borne Fevers
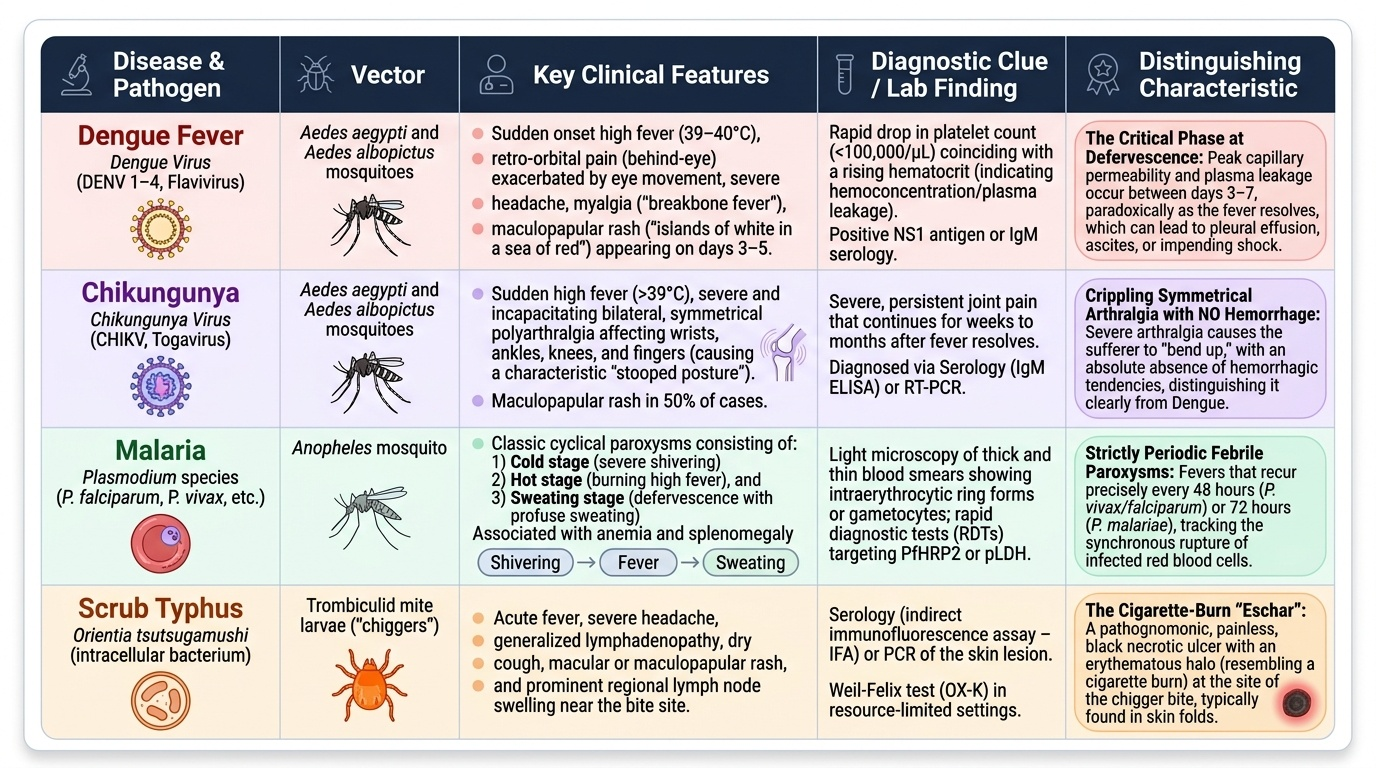
Vector-borne fevers share the feature of an acute febrile illness following a vector exposure, but each disease carries a distinctive clinical fingerprint that allows bedside differentiation when carefully sought. The combination of fever pattern, associated symptoms, skin findings, joint involvement, and haematological clues makes differentiation possible without waiting for laboratory results in most typical presentations.
Provided image
Dengue fever presents with sudden-onset high fever (often 39–40°C), severe headache, retro-orbital (behind-eye) pain exacerbated by eye movement, myalgia, and arthralgia — giving rise to the name 'breakbone fever'. The fever follows a saddle-back pattern in some cases: 2–3 days of high fever, a brief defervescence, then a second febrile period. A maculopapular rash ('islands of white in a sea of red') may appear on days 3–5 as the fever is resolving. The critical phase occurs at defervescence (days 3–7 of illness) when plasma leakage from capillary permeability reaches its peak — paradoxically, the child appears to be improving while internal fluid is shifting into third spaces. WHO 2009 warning signs that predict severe dengue include: abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation (ascites, pleural effusion), mucosal bleeding, lethargy or restlessness, liver enlargement >2 cm, and a rising haematocrit with rapid fall in platelet count. Any ONE of these signs demands urgent assessment and may indicate impending shock.
Chikungunya is characterised by the sudden onset of high fever and incapacitating joint pain — the name derives from a Makonde language word meaning 'that which bends up' (referring to the stooped posture of sufferers). Unlike dengue, the arthralgia in chikungunya is typically symmetrical, polyarticular, affecting the wrists, ankles, knees, and fingers, and may be so severe the child refuses to walk or use their hands. The fever is typically high (>39°C) and abates within 3–4 days; the joint pain, however, can persist for weeks to months after the fever resolves. A maculopapular rash appears in ~50% of patients. Haemorrhage is NOT a feature of chikungunya (distinguishing it from dengue).
Malaria presents differently depending on the species and the child's immune status. A classic malaria paroxysm consists of three stages: cold (shaking chills, rigor), hot (high fever, headache), and sweating (profuse diaphoresis, defervescence). The periodicity of paroxysms reflects the synchrony of RBC rupture: every 48 hours for P. falciparum and P. vivax (tertian), every 72 hours for P. malariae (quartan). However, in children — particularly non-immune children with P. falciparum — fever is often continuous or irregular rather than classically periodic. Splenomegaly is a hallmark of repeated malaria infections. Severe malaria (predominantly P. falciparum) presents with cerebral malaria (altered consciousness, convulsions), severe anaemia (Hb <5 g/dL), respiratory distress, hypoglycaemia, or jaundice.
Scrub typhus is caused by Orientia tsutsugamushi transmitted through the bite of larval trombiculid mites (chiggers) in scrub/bushland. The characteristic — and pathognomonic — feature is the eschar: a painless, black, necrotic skin lesion at the site of the mite bite, with surrounding erythema. The eschar precedes the fever by several days and is found in the groin, axilla, neck, or behind the ear in most but not all cases (absent in 30–50% of cases — do not exclude the diagnosis if no eschar is found). The fever is high, sustained, and accompanied by headache, myalgia, and a diffuse maculopapular rash on the trunk by days 5–7 of illness. Regional lymphadenopathy is prominent near the eschar.
SELF-CHECK
A 10-year-old presents on day 5 of fever that is now defervescing. She has abdominal pain, has vomited 3 times today, and you notice her liver is palpable 3 cm below the costal margin. Her haematocrit has risen from 35% to 42% over the past 24 hours, and her platelet count has fallen from 120,000 to 48,000/µL. What is the clinical significance of these findings?
A. These are expected findings of dengue recovery — discharge home with paracetamol and follow-up in 48 hours
B. These are dengue WARNING SIGNS (abdominal pain, persistent vomiting, hepatomegaly >2cm, rising haematocrit with falling platelets) — admit urgently for monitoring and IV fluid management
C. These suggest scrub typhus — start doxycycline immediately
D. The liver enlargement suggests malaria — order a peripheral blood smear
Reveal Answer
Answer: B. These are dengue WARNING SIGNS (abdominal pain, persistent vomiting, hepatomegaly >2cm, rising haematocrit with falling platelets) — admit urgently for monitoring and IV fluid management
This child has multiple dengue warning signs (WHO 2009): persistent vomiting, abdominal pain/tenderness, liver enlargement >2 cm, rising haematocrit (35→42% = 20% rise, indicating plasma leakage), and rapidly falling platelets. Warning signs occur during the critical phase at defervescence (days 3–7) when plasma leakage is maximal — the child appears to improve (fever falling) while entering the most dangerous stage. Any ONE warning sign mandates hospital admission, close monitoring, and judicious IV fluid management to replace leaked plasma. Discharging this child would risk missing dengue shock syndrome.
Pathogenesis and Aetiology
The pathogenesis of vector-borne fevers illustrates how radically different mechanisms — antibody-mediated immune enhancement, intracellular obligate parasitism, and rickettsial endothelial invasion — can all produce the common final presentation of fever, and yet each produces a distinct disease requiring a completely different treatment approach.
Dengue pathogenesis — immune-mediated plasma leakage:
Dengue virus (flavivirus, DENV 1–4) is inoculated by the day-biting Aedes aegypti mosquito. The virus replicates in dendritic cells and macrophages, then spreads via viraemia. The central pathophysiological event in severe dengue is increased vascular permeability — the capillaries become 'leaky' and plasma (not red blood cells) escapes into the pleural cavity, peritoneal cavity, and interstitium. This plasma leakage explains: rising haematocrit (more RBCs per unit volume as plasma volume falls), hypoalbuminaemia, pleural effusions, and ascites. In secondary dengue infection (different serotype than the first), pre-existing cross-reactive antibodies from the first infection bind but fail to neutralise the new serotype — instead they form immune complexes that enhance viral entry into macrophages (antibody-dependent enhancement, ADE). This causes a greater viraemia and a more intense cytokine storm, explaining why secondary dengue is typically more severe than primary infection. Thrombocytopaenia results from: bone marrow suppression by the virus, platelet consumption by immune complexes, and destruction of virus-coated platelets by the immune system.
Malaria pathogenesis — erythrocyte destruction and cytokine storm:
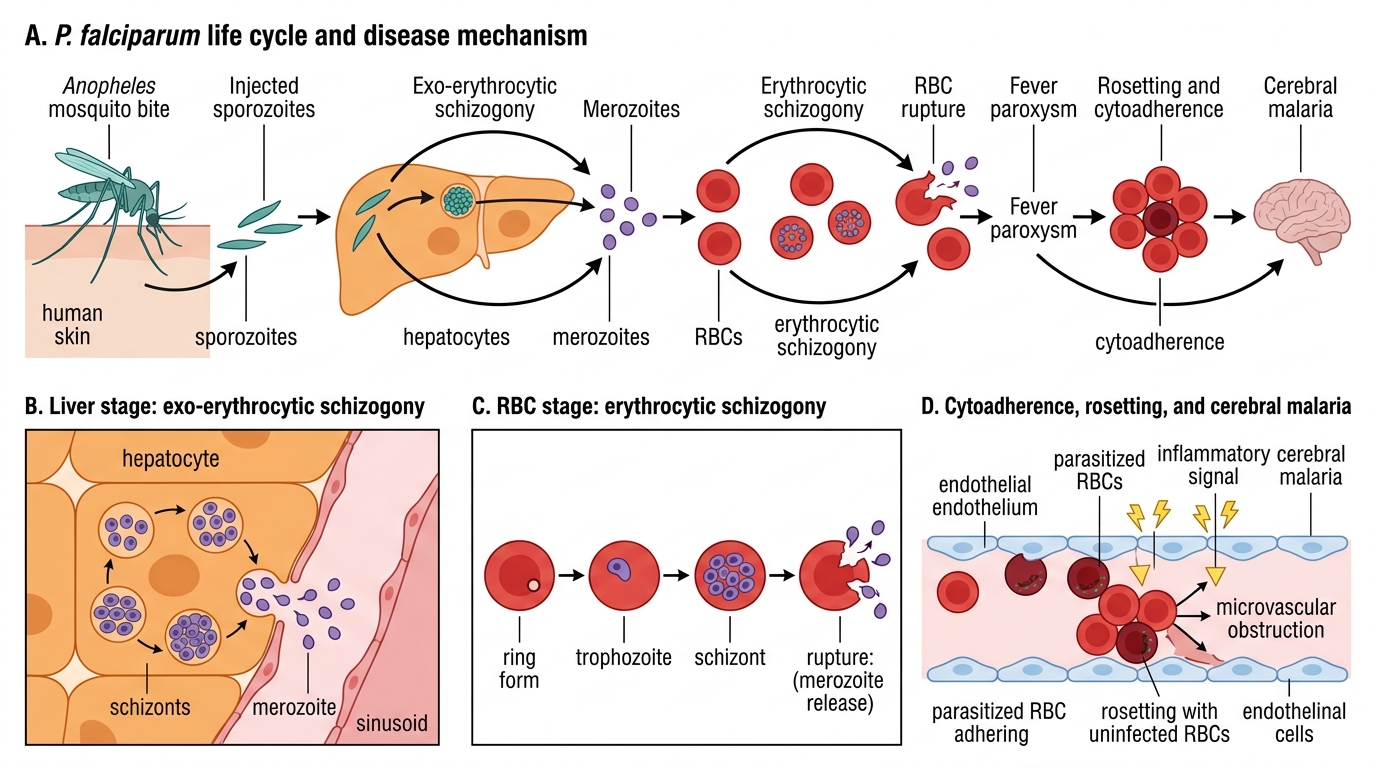
After an Anopheles mosquito bite, sporozoites travel to the liver where they undergo exo-erythrocytic schizogony — multiplying silently in hepatocytes for 7–30 days (this is the incubation period). P. vivax and P. ovale form hypnozoites in the liver — dormant forms that can reactivate weeks to months later, causing relapse. Merozoites released from the liver invade red blood cells and undergo erythrocytic schizogony: ring → trophozoite → schizont → merozoite release (rupturing the RBC) → fever paroxysm. The fever is caused by pyrogens (GPI toxin, haemozoin) released when RBCs rupture. P. falciparum causes severe disease through unique mechanisms: cytoadherence (infected RBCs adhere to capillary endothelium, causing microvascular obstruction — this underlies cerebral malaria) and rosetting (infected RBCs bind normal RBCs in clusters, reducing microvascular flow).
Chikungunya pathogenesis — direct viral joint inflammation:
Chikungunya alphavirus replicates in fibroblasts and synovial cells, causing direct inflammatory arthritis. Unlike dengue, the virus directly invades joint tissues, explaining why joint pain persists long after viraemia resolves. No significant plasma leakage or haemorrhage occurs.
Scrub typhus pathogenesis — endothelial invasion:
Orientia tsutsugamushi is an obligate intracellular gram-negative coccobacillus. After mite-bite inoculation, it replicates in the endothelial cells of small vessels, causing perivasculitis (inflammation around blood vessels). This explains the rash (vasculitis), headache (cerebral vasculitis), and in severe cases, myocarditis and ARDS (alveolar capillary endothelial damage). The eschar at the bite site represents focal skin necrosis at the site of primary mite inoculation.
Plasmodium falciparum Life Cycle and Pathogenesis
Diagnosis and Investigation
Accurate and timely investigation is critical for vector-borne fevers because the window for specific tests often depends on the day of illness, the test chosen must match the clinical phase, and several tests have significant limitations that must be understood to avoid diagnostic error or false reassurance from a negative result. A systematic approach — choosing the right test at the right time — prevents both over-investigation and missed diagnoses. The clinician must resist the reflexive impulse to order every available test simultaneously; instead, the day of fever and the clinical picture should narrow the initial investigation to the most informative test at that moment. For dengue: NS1 if the child has been febrile for fewer than five days, IgM if fever has lasted longer. For malaria: a peripheral blood smear or RDT based on geographic and exposure risk. For scrub typhus: the diagnosis is clinical — supported by serology but not dependent on it. The failure to understand these testing windows is responsible for a large proportion of both missed diagnoses and unnecessary repeat testing.
Dengue diagnosis:
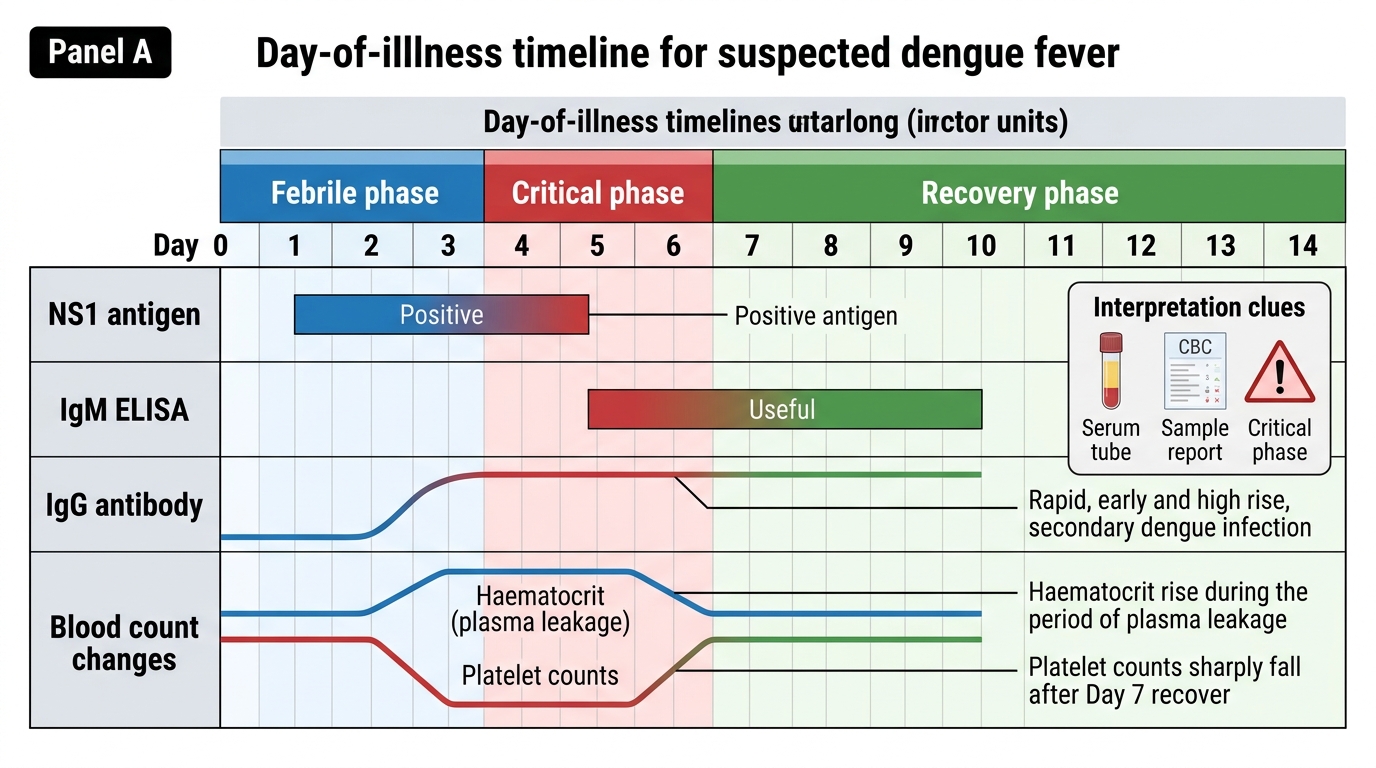
Dengue diagnostic testing is guided by the day of fever:
- Days 1–5 (acute febrile phase): NS1 (Non-Structural protein 1) antigen detection — present in blood from the first day of fever, highly specific for dengue, sensitivity ~80–90% in the first 5 days; falls rapidly after day 5
- Day 5 onwards (defervescence and beyond): IgM antibody detection by ELISA — appears from day 5; IgG detectable in secondary infection (from day 3, often very high titre)
- Dengue IgM/IgG rapid card test: widely available but variable specificity; false positives from other flaviviruses (Zika, Japanese encephalitis), chikungunya cross-reaction
- Blood count hallmarks: rising haematocrit (haemoconcentration from plasma leakage), thrombocytopaenia (platelet count falling to <100,000/µL, sometimes <20,000/µL), and leucopenia. These trends are more clinically useful than absolute values — the DIRECTION of change (rising Hct, falling platelets) signals worsening.
- Do NOT use blood count alone for diagnosis — leucopenia and thrombocytopenia also occur in other febrile illnesses
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Dengue Diagnostic Tests by Day of Illness
Malaria diagnosis:
- Peripheral blood smear (thick + thin film): the gold standard — identifies the species, estimates parasite density, and guides treatment decisions. A negative smear does NOT exclude malaria in a child with a convincing clinical picture — repeat smears every 12–24 hours for 3 days if suspicion is high
- Rapid Diagnostic Test (RDT): detects Plasmodium antigens (HRP-2 for P. falciparum; pLDH for all species); available at point-of-care; does not quantify parasite density or reliably detect P. malariae/P. ovale
- Blood count: anaemia (normocytic, haemolytic), leucopenia or normal leucocyte count, thrombocytopenia
- Hypoglycaemia: always check blood glucose in malaria, especially in children — hypoglycaemia from quinine-stimulated insulin release or increased glucose consumption by parasite is common and correctable
Chikungunya diagnosis:
- Clinical diagnosis in the appropriate epidemiological context (outbreak, Aedes exposure)
- Confirmation: CHIKV-specific IgM ELISA (positive from day 5) or PCR (positive in first 5 days of viraemia)
- No specific blood count hallmark; mild thrombocytopenia may occur
Scrub typhus diagnosis:
- Clinical diagnosis: fever + eschar + rash + lymphadenopathy in an appropriate geographic/exposure context
- Weil-Felix test (OXK antigen): positive in scrub typhus; insensitive and non-specific — should not be the sole diagnostic criterion
- IgM ELISA or Immunofluorescence assay (IFA) for Orientia tsutsugamushi: the reference standard for confirmation
- Peripheral smear for inclusion bodies in leukocytes: not routinely useful
- Blood count: leucopenia or normal WBC, elevated liver enzymes, thrombocytopenia in severe cases