Page 5 of 14
PE14.2 | Organophosphorus Poisoning — SDL Guide (Part 2)
Diagnosis and Investigations
The diagnosis of organophosphorus poisoning is primarily clinical, based on a history of pesticide exposure combined with the characteristic cholinergic toxidrome. No investigation result should delay starting antidote therapy — treatment is initiated on clinical suspicion and the diagnosis confirmed subsequently. The characteristic smell of organophosphates (garlic-like or musty odour on the breath and clothing) adds to the bedside diagnosis.
History: Establish the type, route, and approximate quantity of pesticide exposure; the time elapsed since exposure (critical for PAM eligibility); whether vomiting occurred; and any pre-hospital treatment. Ask about the location where the child was found and the containers present. If possible, bring the container to the hospital for identification of the specific compound.
Clinical examination — the key diagnostic features:
- Miosis (bilateral pinpoint pupils) — highly characteristic; assess in a well-lit room
- Profuse secretions: salivation, lacrimation, bronchial secretions
- Bradycardia and hypotension
- Wheeze and crepitations on chest auscultation
- Muscle fasciculations — look carefully at the limbs and abdominal wall
- Altered consciousness, seizures
Investigations:
- Plasma (serum) cholinesterase activity: Reduced in OP poisoning; <50% of normal indicates significant poisoning. The test confirms the diagnosis but does not change immediate management. Note: plasma cholinesterase is less specific than red blood cell (RBC) cholinesterase, which is a closer proxy for synaptic AChE activity.
- ABG (arterial blood gas): Assess oxygenation, ventilation, and acid-base status — hypoxaemia and respiratory acidosis indicate respiratory failure
- Chest X-ray: May show pulmonary oedema (non-cardiogenic, from bronchial hypersecretions) or aspiration
- ECG: QTc prolongation and bradyarrhythmias
- Blood glucose: Hypoglycaemia can occur
- Renal function, electrolytes: for monitoring and guiding fluid therapy
Differential diagnosis of miosis + altered consciousness: Other causes of miosis include pontine haemorrhage, opioid overdose, and clonidine toxicity — distinguish by the full cholinergic context (secretions, fasciculations, bradycardia all point to OP poisoning).
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
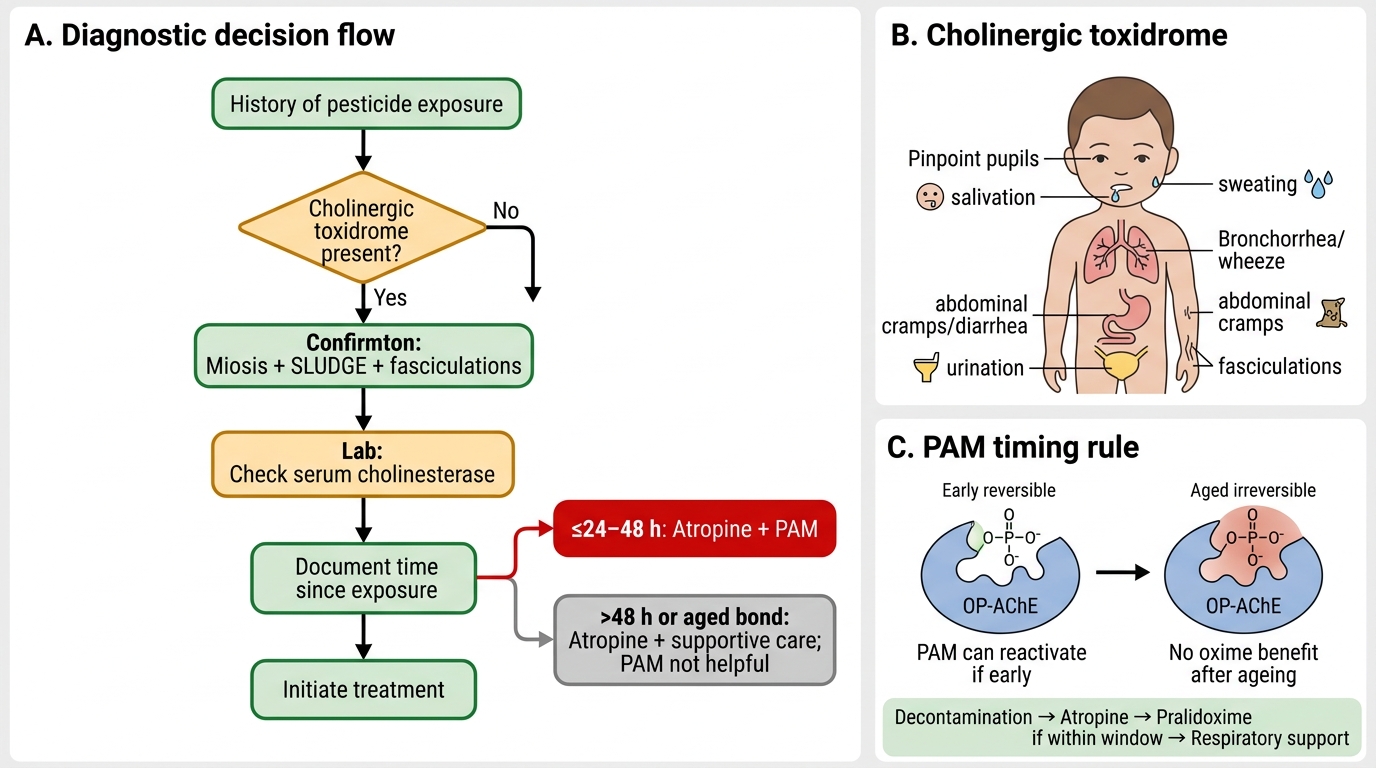
Organophosphorus Poisoning: Diagnosis and PAM Timing
CLINICAL PEARL
The PAM timing window is a hard clinical rule, not a guideline. Pralidoxime (PAM) must be started within 24–48 hours of organophosphorus exposure. Once the OP-AChE bond 'ages' (undergoes irreversible structural change), no oxime can reactivate the enzyme. The body must then synthesise fresh AChE — a process taking days to weeks. A child presenting 3 days after exposure still needs intensive atropine therapy (for muscarinic symptoms) but PAM will not help. Conversely, a child who presents within hours should receive PAM immediately alongside atropine — delaying PAM to 'wait and see' wastes the window. Document the time of exposure on every OP poisoning chart. Never give PAM alone — atropine must always accompany it.
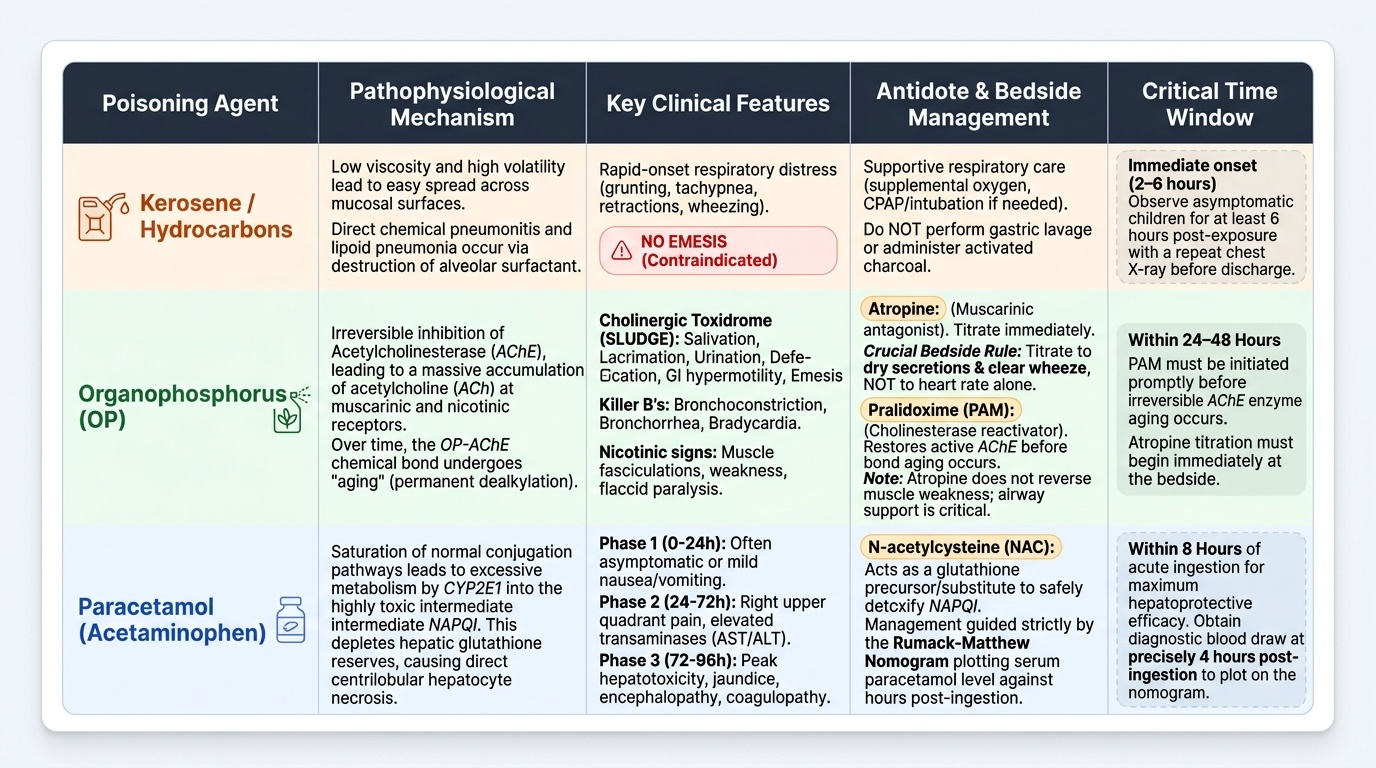
Management: Atropine, Pralidoxime, and Supportive Care
Management of organophosphorus poisoning follows a structured sequence: decontamination to stop ongoing absorption, antidote therapy with atropine and pralidoxime (each targeting a distinct mechanism), and intensive supportive care for respiratory failure. The two antidotes are complementary — not alternatives — and must be used together when the exposure is within the 24–48 hour PAM window. This sequence must be initiated simultaneously rather than serially: while one team member decontaminates, another establishes IV access and begins atropine titration. Delay in atropine risks death from bronchospasm, hypersecretions, or bradycardia; delay in PAM wastes the cholinesterase reactivation window. The management framework is entirely logical once the mechanisms are understood — atropine counters the muscarinic receptor overstimulation at the effector organs, while PAM targets the enzyme itself. Neither alone is sufficient for severe poisoning, and the airway remains the overriding priority throughout.
Provided image
Step 1 — Decontamination (remove the source):
- Remove contaminated clothing and wash all exposed skin thoroughly with soap and water — dermal absorption continues as long as the compound remains on the skin
- Healthcare workers must wear gloves and protective clothing during decontamination to prevent secondary contamination
- For recent ingestion within 1 hour in an alert child: consider cautious gastric lavage (with airway protection) — this is one of the rare situations where gastric lavage may be beneficial if the airway is protected. Activated charcoal 1 g/kg may be given after lavage in an alert child who can protect the airway.
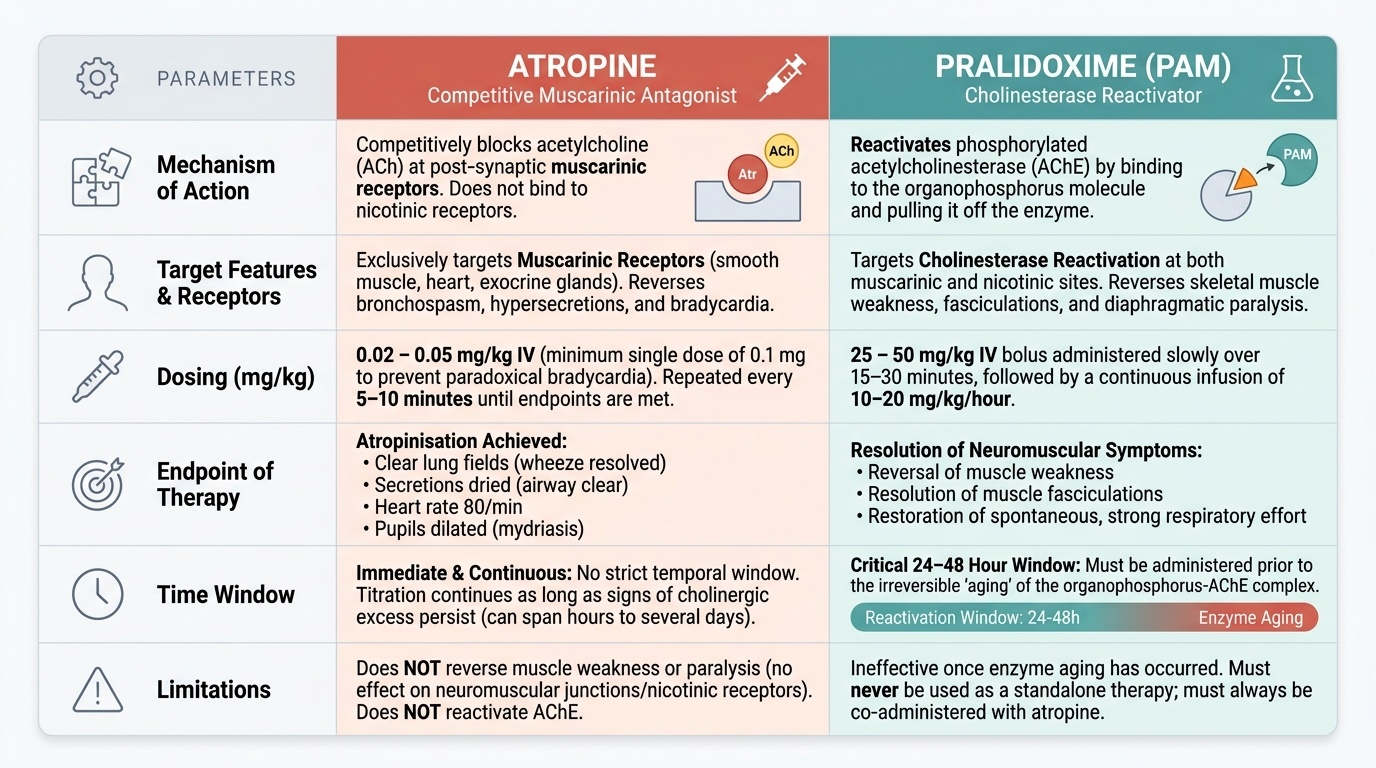
Step 2 — Atropine (titrate to atropinisation endpoint):
- Atropine is a competitive muscarinic antagonist — it blocks muscarinic receptors but has NO effect on nicotinic (NMJ) effects
- Initial dose in children: 0.02–0.05 mg/kg IV (minimum dose 0.1 mg to avoid paradoxical bradycardia from stimulation of cardiac vagal muscarinic receptors at very low doses)
- Repeat every 5–10 minutes until atropinised: endpoint = secretions dry, wheeze cleared, heart rate >80/min, pupils dilated
- No maximum dose — in severe poisoning, hundreds of mg may be required over hours to days
- Atropine does NOT reverse muscle weakness or paralysis (nicotinic effects) and does NOT reactivate AChE
Step 3 — Pralidoxime / PAM (reactivate AChE — within 24–48 h only):
- Pralidoxime is an oxime that displaces the organophosphate from the AChE active site, restoring enzyme function
- Effective ONLY within 24–48 hours of exposure — after the OP-AChE bond ages, the bond is irreversible and PAM has no efficacy
- Paediatric dose: 25–50 mg/kg IV over 15–30 minutes, then maintenance infusion 10–20 mg/kg/hour
- PAM reverses BOTH muscarinic and nicotinic effects (by restoring AChE function), making it broader than atropine
- Continue until the child no longer requires atropine and serum cholinesterase is recovering
Step 4 — Supportive care:
- Airway: Suction secretions; intubate and ventilate if respiratory failure (SpO2 <90%, increasing work of breathing, worsening coma)
- Seizures: Benzodiazepines (diazepam 0.2–0.3 mg/kg IV or midazolam 0.1 mg/kg IV/intranasal); phenobarbitone if refractory
- IV fluids: Maintain perfusion; avoid fluid overload (risk of pulmonary oedema)
- Monitor: ECG (QTc), cholinesterase levels, SpO2, hourly urine output
- Intermediate syndrome: 24–96 hours after acute phase, a proximal muscle weakness syndrome may develop — requires continued ventilatory support
SELF-CHECK
A child is brought with OP poisoning 56 hours after the alleged exposure. She has severe muscarinic features and respiratory distress. Her parents insist on 'the full treatment.' Regarding pralidoxime (PAM), what is the correct action?
A. Give PAM at double dose to overcome the ageing of cholinesterase
B. PAM is still effective up to 72 hours — give the standard dose
C. PAM is likely ineffective beyond 24–48 hours due to irreversible ageing of the OP-AChE bond; focus on atropine and supportive care
D. PAM is contraindicated if atropine has already been given
Reveal Answer
Answer: C. PAM is likely ineffective beyond 24–48 hours due to irreversible ageing of the OP-AChE bond; focus on atropine and supportive care
The organophosphate-AChE bond undergoes irreversible 'ageing' within 24–48 hours of exposure (compound-dependent). Beyond this window, pralidoxime cannot reactivate cholinesterase regardless of dose. The child at 56 hours is almost certainly beyond the PAM window. Management should focus on intensive atropine titration to control muscarinic symptoms, airway support, and mechanical ventilation if needed. Atropine is always indicated regardless of time since exposure and has no maximum dose limit in OP poisoning.
Self-Assessment: Organophosphorus Poisoning
Use these questions to verify that your understanding of organophosphorus poisoning is clinically actionable — not merely recalled for examinations. The key decision-making framework is: recognise the cholinergic toxidrome, immediately titrate atropine to secretion dryness (no fixed dose limit), administer PAM within the 24–48 hour window alongside atropine, support the airway if respiratory muscles fail, and use benzodiazepines for seizures. These are the decisions that save lives at the bedside. OP poisoning tests are consistently high-yield in paediatrics examinations precisely because they encapsulate core pharmacology (receptor selectivity, enzyme kinetics, antidote mechanisms), clinical reasoning under time pressure, and an understanding of how molecular events translate into bedside observations. Ensure you can move fluently between the molecular level (ageing of the OP-AChE bond) and the clinical level (when to stop PAM, when to keep escalating atropine) without compartmentalising the two.
Provided image
Key concepts to explain without reference:
1. What is the SLUDGE mnemonic and what receptor type does each feature arise from?
2. Why does atropine not treat muscle weakness or paralysis in OP poisoning?
3. What is the molecular basis of the PAM timing window?
4. What is the atropinisation endpoint, and why is 'heart rate >80' alone an insufficient measure?
5. What is intermediate syndrome and when does it occur?
Self-check questions:
Q1: A 5-year-old with OP poisoning is receiving atropine. His heart rate is now 102/min but he still has bilateral wheeze and audible secretions. Should atropine be stopped?
→ No. Heart rate alone is not the atropinisation endpoint. Atropine continues until secretions dry and wheeze clears. Tachycardia at this stage reflects incomplete atropinisation, not toxicity.
Q2: PAM is described as a 'cholinesterase reactivator.' What exactly does it reactivate, and why does it fail after 48 hours?
→ PAM breaks the phosphate-serine bond between the OP compound and the AChE active site, freeing the enzyme to function again. After 24–48 hours, this bond undergoes a structural change ('ageing') that makes it resistant to displacement by any oxime.
Q3: Name three features that confirm a cholinergic toxidrome rather than another cause of altered consciousness.
→ Miosis + bronchospasm/hypersecretion + muscle fasciculations (any three from: miosis, salivation, lacrimation, bronchospasm, bradycardia, fasciculations).