Page 2 of 9
PE32.1 | Child Health Ethics and Medicolegal Practice — SDL Guide (Part 2)
Legal Framework: POCSO, JJ Act, and Child Rights
India's child protection legislative architecture has been substantially modernised in the past two decades, and physicians must understand the key statutes that directly impose duties on healthcare providers.
Provided image
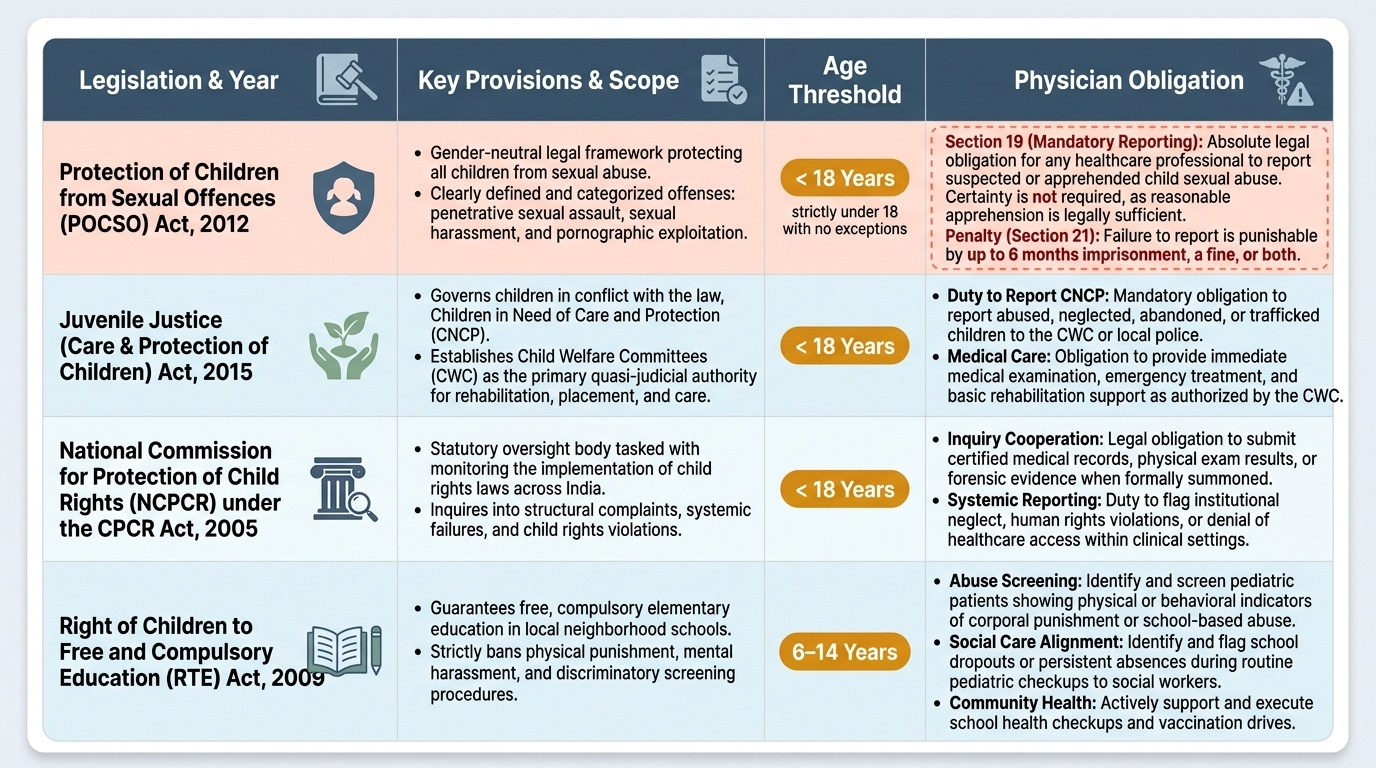
The Protection of Children from Sexual Offences (POCSO) Act 2012 is the centrepiece legislation for child sexual abuse in India. It defines a child as any person below 18 years of age — this threshold has no exceptions. The Act is gender-neutral and covers all categories of sexual offences: penetrative sexual assault, sexual assault, sexual harassment, and use of a child for pornography. Crucially for physicians, Section 19 imposes a mandatory reporting obligation on ANY person — including doctors, nurses, and healthcare staff — who has knowledge or apprehension that a sexual offence against a child has been committed or is being committed. Failure to report is an offence under Section 21, punishable with imprisonment up to 6 months, a fine, or both. The physician need not be certain that abuse occurred; reasonable apprehension is sufficient to trigger the duty. Reports are made to the Special Juvenile Police Unit (SJPU) or local police.
The Juvenile Justice (Care and Protection of Children) Act 2015 replaced the earlier JJ Act of 2000. It defines two categories of children requiring state intervention: children in conflict with the law (offenders) and children in need of care and protection (CNCP) — including children who are abused, neglected, trafficked, or at risk. The Child Welfare Committee (CWC) is the first-line quasi-judicial body responsible for CNCP under the JJ Act 2015. The CWC has the authority to order placement, rehabilitation, and medical care for children. Healthcare providers who encounter a child in need of care and protection are obligated to report to the CWC or police.
The United Nations Convention on the Rights of the Child (UNCRC), ratified by India in 1992, establishes the international framework for child rights across four clusters: survival, development, protection, and participation. While not directly enforceable as Indian domestic law, the UNCRC informs constitutional interpretations under Articles 14, 15, and 21 and underpins child-specific legislation. Its Article 3 (best interests), Article 12 (child's right to be heard), and Article 19 (protection from violence) are particularly relevant to medical practice.
Additional relevant statutes include:
• Right to Education (RTE) Act 2009, Section 17: prohibits corporal punishment and mental harassment of children in schools — paediatricians may encounter and document such injuries.
• Child Labour (Prohibition and Regulation) Amendment Act 2016: prohibits employment of children below 14 years in any occupation; 14–18 year olds prohibited from hazardous occupations.
• Protection of Children from Female Genital Mutilation (FGM): while no specific statute exists, FGM constitutes child abuse under IPC and POCSO.
• National Commission for Protection of Child Rights (NCPCR): established under the Commissions for Protection of Child Rights Act 2005; monitors child rights enforcement and can investigate complaints.
Child Abuse, Neglect, and Medicolegal Recognition
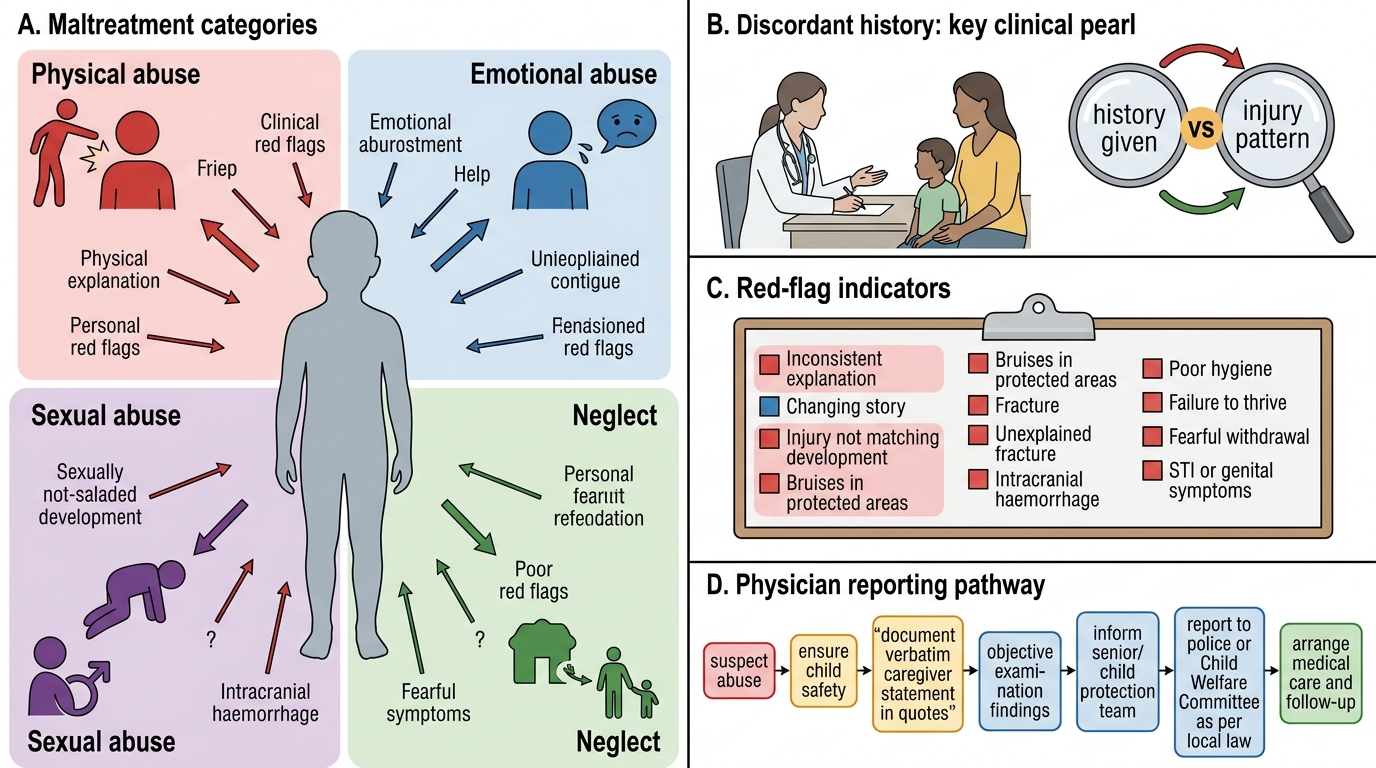
Child maltreatment encompasses four categories, all of which may present to a paediatrician and all of which carry medicolegal implications. Recognising abuse requires a combination of pattern recognition, a high index of suspicion, and careful documentation — not a single pathognomonic finding.
Physical abuse refers to non-accidental infliction of physical injury on a child. The cardinal red flags are injuries that: (a) do not fit the history offered, (b) are in unusual locations (back, buttocks, ears, face, torso — versus accidental injuries on shins, forehead, elbows), (c) show different stages of healing (multiple bruises of different ages = repeated injuries), (d) have a characteristic pattern (loop-shaped bruises = belt; cigarette burns; bite marks), or (e) are severe relative to the developmental ability of the child (e.g. a bruised 2-month-old who cannot yet roll over cannot 'fall'). Skeletal survey X-rays may reveal multiple metaphyseal fractures or posterior rib fractures, which are highly specific for non-accidental injury in infants.
Emotional abuse — chronic psychological maltreatment, exposure to domestic violence, or deliberate humiliation — is the most under-recognised category. Clinical indicators include persistent low self-esteem, extreme behavioural problems, failure to thrive without organic cause, developmental regression, and fearful reactions to specific adults. It rarely presents as a single incident; the physician notices a pattern over time.
Child sexual abuse (CSA) may be disclosed by a child directly, but more often presents with non-specific symptoms: unexplained genital or anal injury, recurrent urinary tract infections, sexually inappropriate behaviour, or sudden behavioural changes. Under the POCSO Act 2012, ANY disclosure or reasonable suspicion triggers mandatory reporting. Medical examination of a child for CSA must be done by a trained examiner; examination alone is often normal (consistent with abuse — absence of injury does not rule out CSA). The physician documents findings objectively and avoids prejudicial language.
Neglect — failure to provide adequate food, shelter, clothing, medical care, or supervision — is the most common category globally and in India. It presents as malnutrition (often SAM: weight-for-height < −3 SD or MUAC <11.5 cm in children 6–59 months), developmental delay, missed immunisations, untreated infections, and poor hygiene. Distinguishing neglect from poverty requires careful history and contextual assessment; poverty alone does not constitute neglect, but poverty compounded by absence of adequate parental care does.
The physician's duty on encountering suspected abuse is clear and legally framed:
1. Stabilise the child medically — child's safety is the immediate priority.
2. Document findings meticulously — accurate, objective, time-stamped, with body diagrams if available.
3. Report immediately — under POCSO Section 19 (for sexual abuse) or JJ Act 2015 (for all abuse/neglect categories) to the police or CWC.
4. Do NOT confront the suspected perpetrator directly or warn them before reporting.
5. Do NOT promise the child or family confidentiality that you cannot ethically keep.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
Child Maltreatment: Red Flags and Reporting Pathway
CLINICAL PEARL
Clinical Pearl — The Discordant History: The single most reliable indicator of non-accidental injury in paediatric practice is a history that does not match the injury pattern. When parents or caregivers change their story on re-questioning, when the mechanism described cannot physically produce the injury found, or when the developmental age of the child precludes the alleged self-injury, abuse must be suspected. Document the exact words used by the caregiver (in quotes, verbatim) in the medical record — this becomes critical evidence. Never record your interpretation instead of the caregiver's actual statement. For any child under 2 years of age presenting with unexplained bruises, fractures, or intracranial haemorrhage, non-accidental injury must be excluded as a priority before any other diagnosis is entertained.
SELF-CHECK
A paediatrician examines a 4-year-old boy brought in by his mother with a bruise on his lower back. The mother says he fell from a chair. The bruise is in a location inconsistent with accidental injury. What is the MOST important immediate action?
A. Ask the father separately to reconcile the discrepancy before taking any action
B. Discharge the child with advice to avoid falls and review in 2 weeks
C. Document the examination findings objectively and report to the police or Child Welfare Committee as suspected non-accidental injury
D. Perform a skeletal survey X-ray and discharge the child if the survey is normal
Reveal Answer
Answer: C. Document the examination findings objectively and report to the police or Child Welfare Committee as suspected non-accidental injury
When a clinical finding is inconsistent with the offered history, the physician's duty under the JJ Act 2015 and general child protection principles is to report suspected abuse to the police or CWC. This is mandatory and does not require certainty — reasonable suspicion suffices. Option A (confronting/questioning family) is dangerous as it may alert a perpetrator and does not protect the child. Option B (discharge) is inappropriate and could endanger the child. Option D (skeletal survey alone and discharge if normal) is insufficient because a normal skeletal survey does not exclude abuse, and the child must not be discharged to a potentially abusive environment without a safety assessment.
Confidentiality, Socio-Cultural Issues, and Vulnerable Paediatric Situations
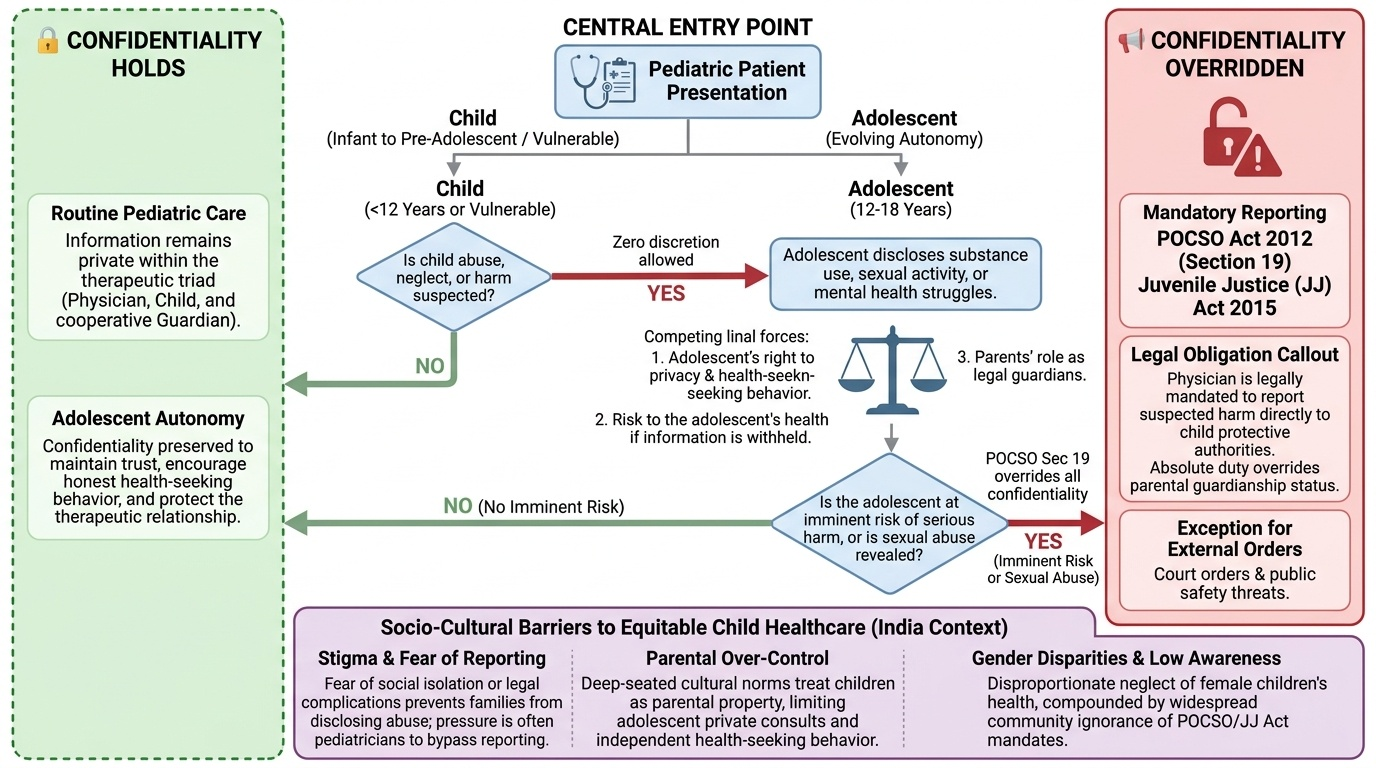
Medical confidentiality — the obligation to keep patient information private — applies in paediatric care but with important modifications. In adult medicine, confidentiality is nearly absolute (with exceptions for public safety and court orders). In paediatric practice, the best interests of the child and the duty to protect vulnerable persons create recognised exceptions.
Provided image
The most important exception is child abuse and neglect: the physician's duty to report suspected harm to a child to protective authorities overrides the general duty of confidentiality. This is not a discretionary decision — it is a legal obligation under POCSO Act 2012 (Section 19) and the JJ Act 2015. It applies even when the abuser is a parent who is simultaneously the child's legal guardian. Physicians must understand that in child protection, reporting is both ethically required and legally mandated.
A second complexity arises in adolescent confidentiality. An adolescent who discloses substance use, sexual activity, or mental health struggles to a physician may be exercising evolving autonomy. The physician must balance: (a) the adolescent's right to privacy and health-seeking behaviour, (b) the risk to the adolescent's health if the information is not acted upon, and (c) the parents' role as legal guardians. The general principle is: if the adolescent is not at imminent risk of serious harm, their confidentiality should be respected to preserve the therapeutic relationship. However, if the adolescent reveals they are being sexually abused (even if they ask for confidentiality), POCSO Section 19 mandates reporting regardless.
Socio-cultural barriers to child healthcare in India are clinically significant and ethically complex:
- Gender bias: preference for male children affects access to nutrition, vaccination, and medical care for girls. Paediatricians who work in communities with documented gender bias have a professional obligation to advocate for equitable care and report concerning patterns.
- Harmful traditional practices: practices such as female genital mutilation (FGM, associated with certain communities), traditional bone-setting causing growth-plate injuries, or withholding colostrum (believing it is harmful) cause direct physical harm. These must be recognised, documented, and reported where they constitute abuse.
- Vaccine hesitancy: religious or cultural objections to vaccination present a conflict between parental autonomy and the child's right to preventive health protection. The ethical approach is to engage empathetically, provide accurate information, counter misinformation respectfully, and document the counselling. Where refusal creates serious risk (e.g. refusal of neonatal BCG or pentavalent vaccination in areas of high disease burden), involving a senior colleague or medical superintendent may be appropriate. Legal compulsion of vaccination does not currently exist in Indian law except in specific outbreak contexts (under the Epidemic Diseases Act 1897).
- Resource allocation and justice: in resource-limited settings, the physician may face allocation dilemmas — one PICU bed available, two critically ill children. Utilitarian, egalitarian, and clinical-urgency frameworks guide these decisions; transparent institutional policies reduce ad-hoc bias.
- Disability and child rights: the Rights of Persons with Disabilities Act 2016 guarantees equal rights to children with disabilities, including the right to inclusive education, accessible healthcare, and protection from discrimination. Paediatricians have a duty to advocate for children with disabilities and ensure that treatment decisions are not made on ableist grounds.