Page 4 of 17
PE3.4 | Child Developmental Unit Visit — SDL Guide
Learning Objectives
- Describe the composition and roles of the multidisciplinary team in a Child Developmental Unit (CDU)
- Explain the referral criteria and workflow of a CDU visit from intake to management plan
- Observe the functioning of a CDU and identify the tools, techniques, and team interactions involved in developmental assessment
- Reflect on the experience of observing a CDU visit and its implications for clinical practice
INSTRUCTIONS
The Child Developmental Unit (CDU) is where the theoretical knowledge of developmental paediatrics becomes visible in real clinical practice. As a final-year student, you are required to observe a CDU visit as part of your competency PE3.4. This module prepares you to make the most of that observation — understanding who you will see, what they are doing and why, and how to translate what you observe into meaningful clinical learning. Most developmental diagnoses are made through careful observation and standardised testing, not blood tests or scans, which makes the CDU visit a uniquely important learning opportunity.
References
- Ghai Essential Pediatrics, 9th ed., Ch 18 (Developmental Paediatrics — CDU structure and team) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 38 (Assessment of developmental competence) (textbook)
- IAP Guidelines on Developmental Delay: Multidisciplinary Team Approach, 2022 (guideline)
- Rashtriya Bal Swasthya Karyakram (RBSK): District Early Intervention Centres operational guidelines, MoHFW India (programme)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You arrive at the Child Developmental Unit on a Tuesday morning. In the waiting area sit five families: a mother with a 2-year-old who isn't walking yet; a father with a 4-year-old who has just been told may have autism; a grandmother with a child who has Down syndrome coming for his quarterly review. Inside, a physiotherapist is coaxing a child to crawl across a foam mat while a speech therapist sits opposite a toddler with picture cards, counting how many words the child will attempt. A psychologist is talking quietly with parents in a side room. A developmental paediatrician reviews notes before a team case conference. You are about to observe all of this — but do you know what you're looking for, and why?
WHY THIS MATTERS
Understanding how a Child Developmental Unit (CDU) functions is important for every clinician, not only developmental paediatricians. In your future career — whether in general practice, community health, or any clinical specialty — you will encounter children whose developmental concerns have gone unrecognised, or whose families are navigating a complex system of referrals and therapies. Knowing what a CDU does, what it can offer, and how to refer appropriately will make you a more effective advocate for your patients. Equally, witnessing the multi-professional collaboration at a CDU provides a model for team-based care that applies far beyond paediatrics — the CDU is one of the clearest examples in medicine of a team where no single professional can do the job alone.
RECALL
Before this observation visit, consolidate your background knowledge:
• Global developmental delay (GDD): delay in ≥2 domains in a child <5 years; intellectual disability (ID): IQ <70 + adaptive deficits, onset before 18 years.
• Developmental regression: loss of previously acquired skills — always pathological, always urgent.
• Assessment tools: DASII (Indian norm-referenced, ages 0–30 months); DDST-II (screening, 0–6 years); Vineland Adaptive Behavior Scales (adaptive functioning).
• Treatable causes to never miss: congenital hypothyroidism (screen with TSH/T4), PKU (screen with phenylalanine), hearing loss (BERA), lead toxicity (blood lead level).
• Key principle: early intervention works — the earlier therapy begins, the greater the neuroplasticity benefit.
Clinical Indication and Relevance of CDU
A Child Developmental Unit (CDU) is a specialised multidisciplinary outpatient service that provides comprehensive assessment, diagnosis, and management planning for children with suspected or confirmed developmental delay and related neurodevelopmental disorders. The CDU is the clinical setting where a range of specialists come together — in one visit — to evaluate a child from multiple perspectives simultaneously, avoiding the fragmented care that results from sequential single-discipline referrals spread across many months and many departments. The central design philosophy of a CDU is that the whole child cannot be understood by any one professional alone: the physiotherapist sees how the child moves, the speech therapist hears how the child communicates, the psychologist measures how the child thinks, and the developmental paediatrician synthesises all of these into a coherent clinical picture. This integrated assessment model produces a more accurate diagnosis, a more comprehensive management plan, and a far better family experience than the alternative of waiting months for separate appointments in separate departments.
Children are referred to a CDU when a developmental concern has been identified through primary care, RBSK screening, immunisation visits, antenatal history (e.g., known chromosomal abnormality), or parental concern. Common referral indications include:
• Global developmental delay or failure to attain age-appropriate milestones
• Language delay (isolated expressive, receptive, or combined)
• Motor delay or suspected cerebral palsy
• Regression of previously acquired skills
• Autism spectrum disorder (ASD) screening positive
• Down syndrome or other chromosomal conditions (routine surveillance)
• Prematurity with developmental surveillance needs
• Suspected intellectual disability
• Behavioural concerns with developmental correlates (ADHD, ASD)
The clinical relevance of the CDU visit for a final-year student is twofold: first, it bridges the gap between classroom knowledge of developmental milestones and the reality of how assessment is conducted in a real child; second, it models the multidisciplinary, family-centred approach that is the evidence-based standard for managing developmental disorders.
IMDIA's (Indian Academy of Developmental Paediatrics) and IAP's position statements strongly endorse the CDU model as superior to sequential single-specialty referrals in terms of diagnostic accuracy, family experience, and time to intervention.
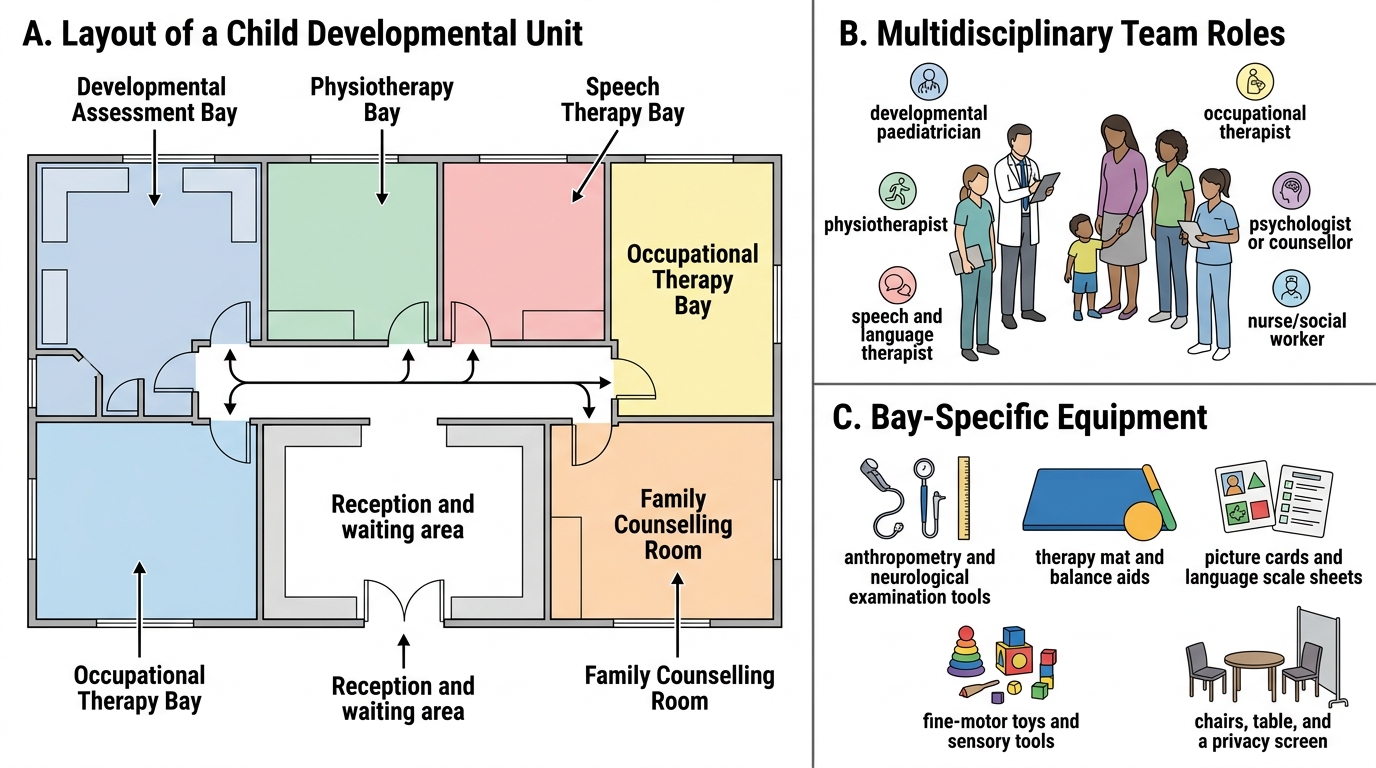
Layout and Function of a Child Developmental Unit
Anatomy of a CDU: Team, Space, and Equipment
Understanding who is in the room — and what each person is watching for — transforms passive observation into active learning. The core CDU team consists of specialists from at least five disciplines, and each brings a distinct lens to the same child.
The developmental paediatrician is the team leader. They conduct the medical and neurodevelopmental history, perform the physical examination including anthropometry and neurological assessment, integrate findings from all team members, and formulate the overall diagnosis and management plan. They also co-ordinate investigations and communicate the diagnosis to the family.
The physiotherapist assesses gross motor function — muscle tone, strength, balance, coordination, gait pattern, and functional mobility. They use standardised motor assessments such as the Gross Motor Function Measure (GMFM) for children with cerebral palsy.
The speech and language therapist evaluates receptive language (understanding), expressive language (production), articulation, fluency, and pragmatics (social use of language). For pre-verbal children, they assess pre-linguistic skills such as joint attention, pointing, and imitation. Tools include the Receptive-Expressive Emergent Language Scale (REEL) and standardised articulation tests.
The occupational therapist assesses fine motor skills, visual-motor integration, sensory processing, activities of daily living (self-feeding, dressing, toileting), and handwriting readiness. Tools include the Beery-Buktenica Developmental Test of Visual-Motor Integration.
The clinical psychologist conducts formal cognitive and adaptive behaviour assessments when intellectual disability is suspected. Tools include the Malin's Intelligence Scale for Indian Children (MISIC) (standardised for Indian children aged 6–15 years) and the Vineland Adaptive Behavior Scales. They also screen for ASD using the Childhood Autism Rating Scale (CARS) or Autism Diagnostic Observation Schedule (ADOS) when indicated.
The special educator observes learning-readiness, academic skill levels, and classroom behaviour; they contribute to individualized education plan (IEP) development.
The medical social worker assesses family circumstances, socioeconomic supports, and barriers to accessing therapy and schooling; they connect families to government entitlements under the RPWD Act 2016 and National Trust Act 1999.
The audiologist may be co-located or available for same-day BERA (Brainstem Evoked Response Audiometry) when hearing impairment is in the differential.
| CDU Team Member | Primary Focus | Key Tools |
|---|---|---|
| Developmental paediatrician | Medical history, neurology, diagnosis | DASII, DDST-II, neurological exam |
| Physiotherapist | Gross motor, tone, gait | GMFM, clinical observation |
| Speech-language therapist | Language, communication, feeding | REEL, articulation tests |
| Occupational therapist | Fine motor, ADL, sensory | Beery VMI, ADL assessment |
| Clinical psychologist | Cognition, adaptive behaviour, ASD | MISIC, Vineland, CARS/ADOS |
| Special educator | Learning readiness, academic skills | IEP assessment tools |
| Medical social worker | Family support, entitlements | Social assessment forms |
SELF-CHECK
During a CDU visit, which team member is MOST appropriate to formally assess whether a 5-year-old child meets diagnostic criteria for intellectual disability?
A. Developmental paediatrician
B. Clinical psychologist
C. Special educator
D. Occupational therapist
Reveal Answer
Answer: B. Clinical psychologist
The clinical psychologist administers standardised cognitive assessments (such as MISIC for Indian children) and adaptive behaviour scales (Vineland) to formally determine whether IQ <70 and adaptive deficits are present — the two required criteria for intellectual disability. The developmental paediatrician integrates these findings with the clinical picture to make the diagnosis, but the cognitive testing itself is performed by the psychologist.
CDU Assessment Process: What You Observe
A CDU visit follows a structured workflow that moves the child and family through a sequence of assessments, culminating in a multidisciplinary team case conference where findings are synthesised and a management plan is agreed. Understanding this workflow in advance allows you to observe meaningfully rather than simply watching unfamiliar activity.
Step 1 — Pre-visit preparation: The referral letter and previous records are reviewed. The developmental paediatrician notes the presenting concerns, relevant antenatal and perinatal history, and any prior investigations or therapy. A structured intake form is sent to parents ahead of the visit.
Step 2 — Parent/caregiver interview: The developmental paediatrician (often with the social worker present) takes a detailed history: developmental milestones, regression, family history, antenatal history, social circumstances. This is the single most information-rich step and typically takes 20–30 minutes.
Step 3 — Medical and neurological examination: Height, weight, head circumference plotted on WHO/Indian Academy of Pediatrics (IAP) growth charts. General examination for dysmorphic features, skin findings (tuberous sclerosis, neurofibromatosis). Neurological examination: tone, reflexes, cranial nerves, coordination, gait. Fundoscopy if indicated.
Step 4 — Formal developmental assessment: The developmental paediatrician (or psychologist) administers a standardised assessment — DASII for children under 30 months, or the appropriate age-band instrument. This involves structured play tasks, object manipulation, picture naming, imitation, and social interaction tasks. The child's responses are scored against normative data.
Step 5 — Therapy assessments (concurrent or sequential): While the developmental paediatrician reviews, the physiotherapist, speech therapist, and occupational therapist each spend 15–20 minutes with the child in their respective bays — observing movement patterns, communication attempts, fine motor tasks, and play skills.
Step 6 — Team case conference: All professionals gather (with parents, if a family-centred CDU) to share findings, reconcile observations, formulate a diagnosis (or differential), and agree a management plan. This is where the child is seen as a whole person, not just a collection of individual impairments.
Step 7 — Family feedback session: The developmental paediatrician and/or team lead explains the findings to the parents in plain language, outlines the diagnosis and its implications, introduces the therapy plan, and connects the family to relevant government entitlements. Written reports are provided.
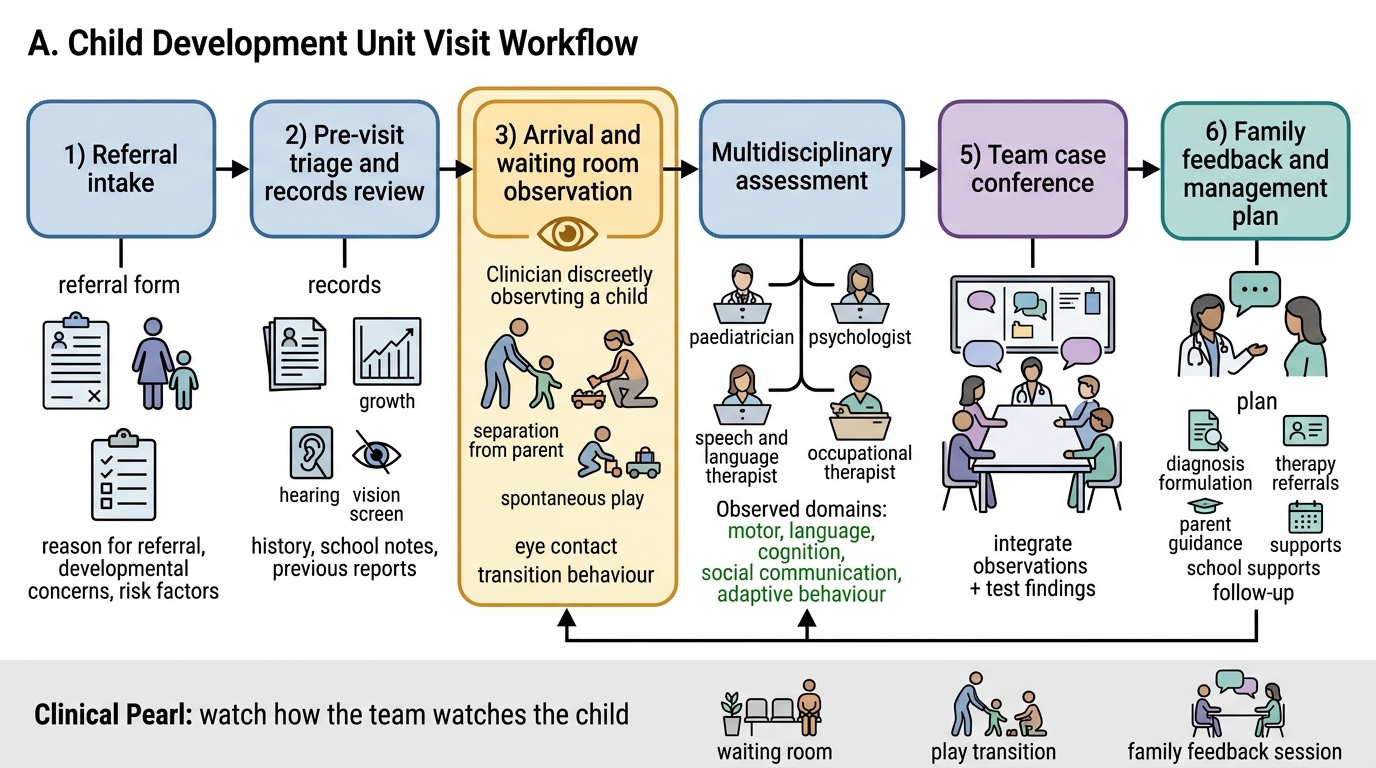
Child Development Unit Visit Workflow
CLINICAL PEARL
Watch how the team watches the child: During the CDU visit, the most important observation is not the child's formal test score — it is the child's spontaneous behaviour in the waiting room, during play transitions, and during the family feedback session. Children often show their most representative abilities (and difficulties) when they are unaware of being assessed. Experienced CDU clinicians gather critical data just by watching a child enter the room: how does the toddler separate from the parent, how does the child explore a new toy, does the child make eye contact with a stranger? Train yourself to notice these behaviours, and ask team members afterwards what they observed and why it mattered.