Page 4 of 17
PE5.2 | Breath Holding Spells — SDL Guide
Learning Objectives
- Describe the two types of breath-holding spells — cyanotic and pallid — including their triggers and the sequence of events.
- Explain the pathophysiological mechanisms underlying each type of breath-holding spell.
- Distinguish breath-holding spells from epileptic seizures and other causes of transient loss of consciousness in children.
- Outline the management of breath-holding spells, including the role of iron supplementation and parental counselling.
INSTRUCTIONS
Breath-holding spells are one of the most alarming presentations parents bring to a paediatrician, yet they are almost invariably benign. A 2-year-old who turns blue and loses consciousness after a temper tantrum is terrifying to witness, but if you understand the mechanism you will be able to reassure the family confidently and avoid unnecessary investigations. This module teaches you to recognise the two types, explain the mechanism to parents, and manage the rare cases that require intervention.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 (Behavioural Problems) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 609 (Breath-Holding Spells) (textbook)
- IAP Textbook of Pediatrics, 6th ed. — Behavioural Pediatrics (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the emergency department when a frantic mother rushes in carrying her 18-month-old daughter. 'She stopped breathing and went blue — I thought she was dying!' The mother explains that the child was crying after being refused a toy, let out a long cry, then went silent, turned blue, and became limp. The episode lasted about 30 seconds; the child is now fully awake and back to normal. On examination: no fever, no focal neurological signs, normal tone and reflexes. What has happened, what investigation — if any — is needed, and what will you tell this mother?
WHY THIS MATTERS
Breath-holding spells (BHS) affect an estimated 0.1–4.6% of children, making them one of the commonest paroxysmal events in the paediatric age group. They are almost invariably benign and self-limiting, yet they cause enormous parental anxiety and frequently trigger unnecessary investigations including ECG, EEG, and hospital admissions. The paediatrician's role is to make a confident clinical diagnosis from the history, to distinguish BHS from the important differentials (particularly epilepsy), and to provide accurate, reassuring counselling. Excessive investigation driven by parental anxiety or physician uncertainty leads to false labelling and potential harm. Understanding the precise mechanism of each type enables targeted management in the small subset where treatment is indicated.
RECALL
Before proceeding, recall:
• The vagal reflex: stimulation of cranial nerve X (vagus) causes slowing of the heart (bradycardia) and may cause transient asystole; this pathway is well developed and active in young children.
• Cerebral blood flow autoregulation: the brain requires continuous oxygen delivery; brief interruption of cardiac output or oxygenation leads to loss of consciousness within seconds.
• Iron-deficiency anaemia in children under 5: defined as Hb <11 g/dL (WHO); iron deficiency (even before frank anaemia) affects autonomic nervous system function.
• Epilepsy vs syncope: epileptic seizures originate from cortical electrical discharges and are usually not trigger-dependent; syncope (including BHS) is a brief circulatory interruption and is trigger-dependent.
Clinical Presentation of Breath Holding Spells
Breath-holding spells are paroxysmal events in young children characterised by an involuntary cessation of breathing following a specific trigger, leading to cyanosis or pallor and, in severe cases, transient loss of consciousness. Despite the dramatic appearance, they are involuntary — the child does not choose to hold their breath — and they are not epilepsy. They occur almost exclusively between the ages of 6 months and 5 years, with peak incidence at around 2 years. They are rare before 6 months of age. A positive family history is found in approximately 25–30% of cases, suggesting an autosomal dominant predisposition with variable penetrance.
Provided image
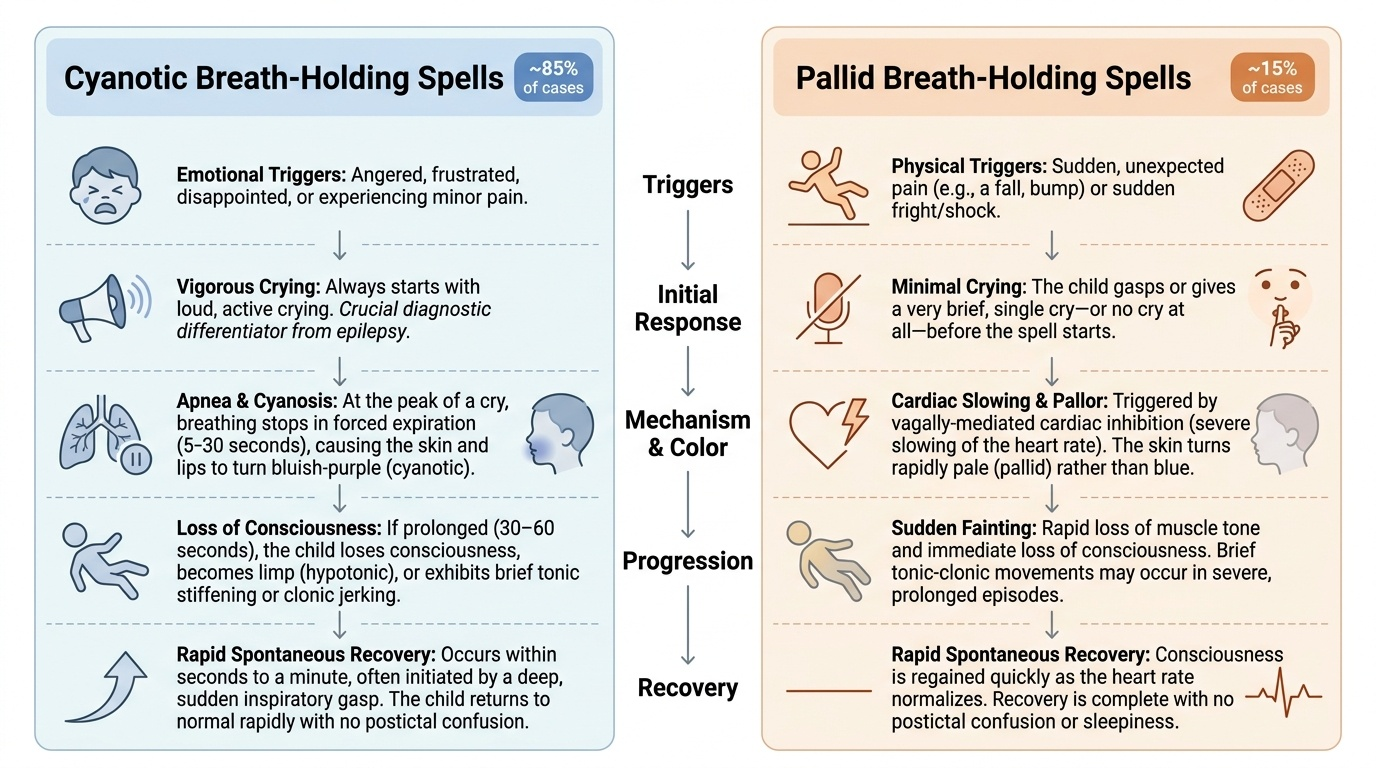
There are two distinct clinical types that the paediatrician must be able to identify from the history:
1. Cyanotic breath-holding spells (~85% of cases):
- Trigger: emotional — anger, frustration, disappointment, or minor pain, always preceded by crying.
- Sequence: The child begins crying loudly → at the peak of a cry, breathing stops in forced expiration → within 5–30 seconds the child turns blue (cyanotic) → if the spell is prolonged (>30–60 seconds), loss of consciousness occurs → the child may become limp (hypotonic) or, if more prolonged, develop a brief tonic stiffening or clonic jerking → the child recovers spontaneously within seconds to a minute, often with a deep inspiratory gasp → recovery is rapid with no postictal confusion.
- The spell is always preceded by crying — this distinguishes it from epileptic seizures.
2. Pallid breath-holding spells (~15% of cases):
- Trigger: sudden unexpected pain (a fall, a bump) or fright — the child may give only a brief cry or no cry at all before the spell.
- Sequence: minor injury or shock → brief or no cry → sudden loss of tone → pallor (not cyanosis) → loss of consciousness → brief tonic-clonic movements in severe cases → rapid spontaneous recovery.
- The mechanism here is vagally-mediated cardiac inhibition (see pathophysiology below), not respiratory.
Pathophysiology and Aetiology
The two types of breath-holding spells have distinct mechanisms, both of which result in the final common pathway of transient cerebral hypoxia and loss of consciousness. Understanding these mechanisms is essential for explaining the condition to parents and for guiding treatment decisions.
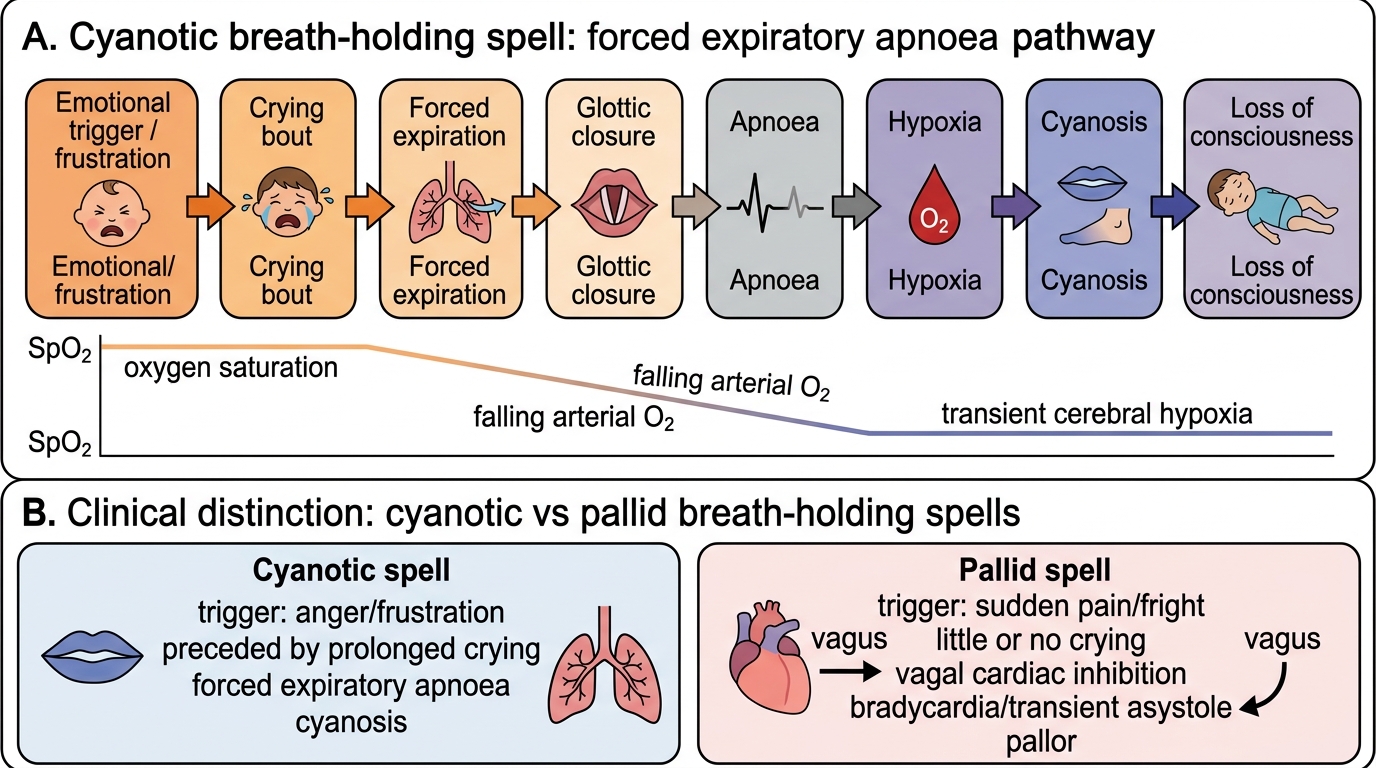
Cyanotic BHS — hypoxic mechanism:
An emotional stimulus (anger, frustration, pain) triggers a prolonged crying episode. At the height of the cry, the child exhales forcefully and then involuntarily holds the breath in the expiratory position. This is not a deliberate action — it is an involuntary reflex. Forced expiration raises intrathoracic pressure (Valsalva effect), reduces venous return to the heart, and decreases cardiac output. Simultaneously, the forced apnoea prevents fresh oxygenation of blood. The combination of reduced oxygen delivery and rising carbon dioxide causes progressive cerebral hypoxia. Within 20–30 seconds, the child becomes cyanotic; if the spell continues, cerebral hypoxia is sufficient to cause loss of consciousness and, in severe prolonged cases, brief anoxic seizures (tonic or tonic-clonic movements). These anoxic seizures are not epilepsy — they are a direct consequence of cerebral hypoxia and carry the same benign prognosis as the spell itself. The spell terminates by reflex gasping as the hypoxic/hypercapnic drive overcomes the breath-hold, restoring breathing and rapidly reversing cyanosis.
Pallid BHS — vagal mechanism:
A sudden unexpected stimulus (unexpected pain, cold water splash, a fright) activates the cardioinhibitory vagal reflex. Intense afferent vagal stimulation triggers efferent vagal output to the sinoatrial node, causing bradycardia or transient asystole. The sudden cessation of cardiac output produces cerebral hypoperfusion within 3–5 seconds, causing the child to go limp, pale, and unconscious. This is essentially a reflex syncope or reflex anoxic seizure. The ECG during a pallid spell shows the characteristic asystolic pause. Recovery is spontaneous as cardiac output resumes.
Role of iron deficiency:
Iron deficiency — even at the subclinical stage before frank anaemia — has been associated with increased frequency and severity of BHS. The proposed mechanism involves iron's role as a cofactor in dopamine synthesis; iron deficiency alters central dopaminergic and serotonergic tone, which affects autonomic regulation. Several randomised controlled trials (including those by Mocan and DiMario) have demonstrated that iron supplementation reduces the frequency of BHS in children with documented iron deficiency, independent of haemoglobin level. Checking for iron deficiency is therefore part of the evaluation of frequent or severe BHS.
Mechanism of Cyanotic Breath-Holding Spell
SELF-CHECK
An 18-month-old child is brought to the clinic after three episodes in the past month. Each episode begins when the child bumps his head or falls unexpectedly; he gives a brief cry, then suddenly goes pale and limp, losing consciousness for about 20 seconds before recovering. There is no cyanosis, no preceding temper tantrum, and recovery is prompt. What type of breath-holding spell is this, and what is the underlying mechanism?
A. Cyanotic breath-holding spell; mechanism is forced expiratory apnoea causing hypoxia
B. Pallid breath-holding spell; mechanism is vagally-mediated cardiac inhibition causing transient asystole
C. Absence epilepsy; mechanism is generalised cortical electrical discharge
D. Reflex anoxic seizure due to hypoglycaemia
Reveal Answer
Answer: B. Pallid breath-holding spell; mechanism is vagally-mediated cardiac inhibition causing transient asystole
Pallid breath-holding spells are triggered by sudden pain or fright, are characterised by pallor (not cyanosis), and are caused by intense vagal stimulation causing bradycardia or transient asystole. The absence of cyanosis, the minor injury trigger, the lack of preceding crying bout, and the rapid recovery all point to the pallid type. Cyanotic BHS requires preceding crying and shows cyanosis. Absence epilepsy has no trigger and no colour change. Hypoglycaemia does not cause sudden brief pallid episodes with immediate full recovery.
Diagnosis and Differential Diagnosis
Breath-holding spells are a clinical diagnosis based entirely on the history. No investigation is required to make the diagnosis when the history is typical. The key to confident diagnosis is eliciting the sequence of events with precision: trigger → cry → colour change → spell → recovery. A structured, systematic history that takes the parent step-by-step through a recent episode will, in most cases, yield a diagnosis within minutes. The paediatrician should resist the impulse to order investigations before completing this structured history, as the diagnosis is almost always apparent from the history alone. Investigations are reserved for atypical presentations, suspected iron deficiency, or cases where the differential diagnosis remains genuinely uncertain after a thorough history and examination.
A structured history should establish:
1. Trigger: Was there a precipitating emotional event (cyanotic) or sudden unexpected pain/shock (pallid)?
2. Cry: Did crying precede the colour change? (Always present in cyanotic; minimal or absent in pallid.)
3. Colour change: Blue/cyanotic or white/pallid?
4. Loss of consciousness: Did it occur? For how long?
5. Movements: Were there jerking movements? (Anoxic seizures in prolonged BHS are brief tonic or tonic-clonic; they are NOT epilepsy.)
6. Recovery: Was it rapid and complete, without prolonged drowsiness or confusion? (Postictal confusion suggests epilepsy.)
7. Age and frequency: Within the typical age range (6 months–5 years)? Family history of similar events?
Investigations are not required in typical cases. However, specific investigations are indicated when:
- Iron-deficiency anaemia is suspected: full blood count, serum ferritin, serum iron/TIBC.
- Pallid BHS with severe or very frequent events: ECG to document prolonged asystolic pause during a provoked episode (ocular compression test may trigger a pallid spell); Holter monitoring in selected cases.
- Atypical features (no trigger, prolonged episodes, postictal confusion, onset <6 months or >5 years): EEG to exclude epilepsy.
Key differentials and distinguishing features:
| Feature | Cyanotic BHS | Pallid BHS | Epileptic Seizure | Simple Syncope |
|---|---|---|---|---|
| Trigger | Emotional, crying | Pain/fright | Usually none | Postural, pain, heat |
| Preceding cry | Yes | Minimal/none | No | No |
| Colour | Cyanosis | Pallor | Variable | Pallor |
| EEG | Normal | Normal | Abnormal | Normal |
| ECG during episode | Normal | Asystolic pause | Normal | Bradycardia |
| Duration | <1 min | <30 sec | Variable (often >1 min) | <1 min |
| Postictal | No | No | Yes (confusion, sleep) | No |
| Age | 6 mo–5 yr | 6 mo–5 yr | Any | >5 yr usually |
| Prognosis | Resolves by 5–6 yr | Resolves by 5–6 yr | Requires treatment | Usually benign |
CLINICAL PEARL
The single most important diagnostic feature distinguishing a cyanotic BHS from an epileptic seizure is the sequence: CRY FIRST, then colour change, then spell. An epileptic seizure does not require a prior crying episode. When parents describe a child 'turning blue during a tantrum' — that is BHS, not epilepsy. Also: the brief tonic or clonic movements seen at the end of a prolonged BHS are anoxic seizures (a consequence of hypoxia) — they look like epilepsy but are not. Treating them as epilepsy with anti-seizure medications is incorrect and unnecessary. The EEG, if done between episodes, is completely normal in BHS.