Page 2 of 17
PE5.1 | Feeding Problems — SDL Guide (Part 2)
Management of Feeding Problems
Management of feeding problems is guided by the underlying category. For organic causes, treatment of the cause is primary; for behavioural and developmental problems, a structured behavioural and nutritional approach is used.
Provided image
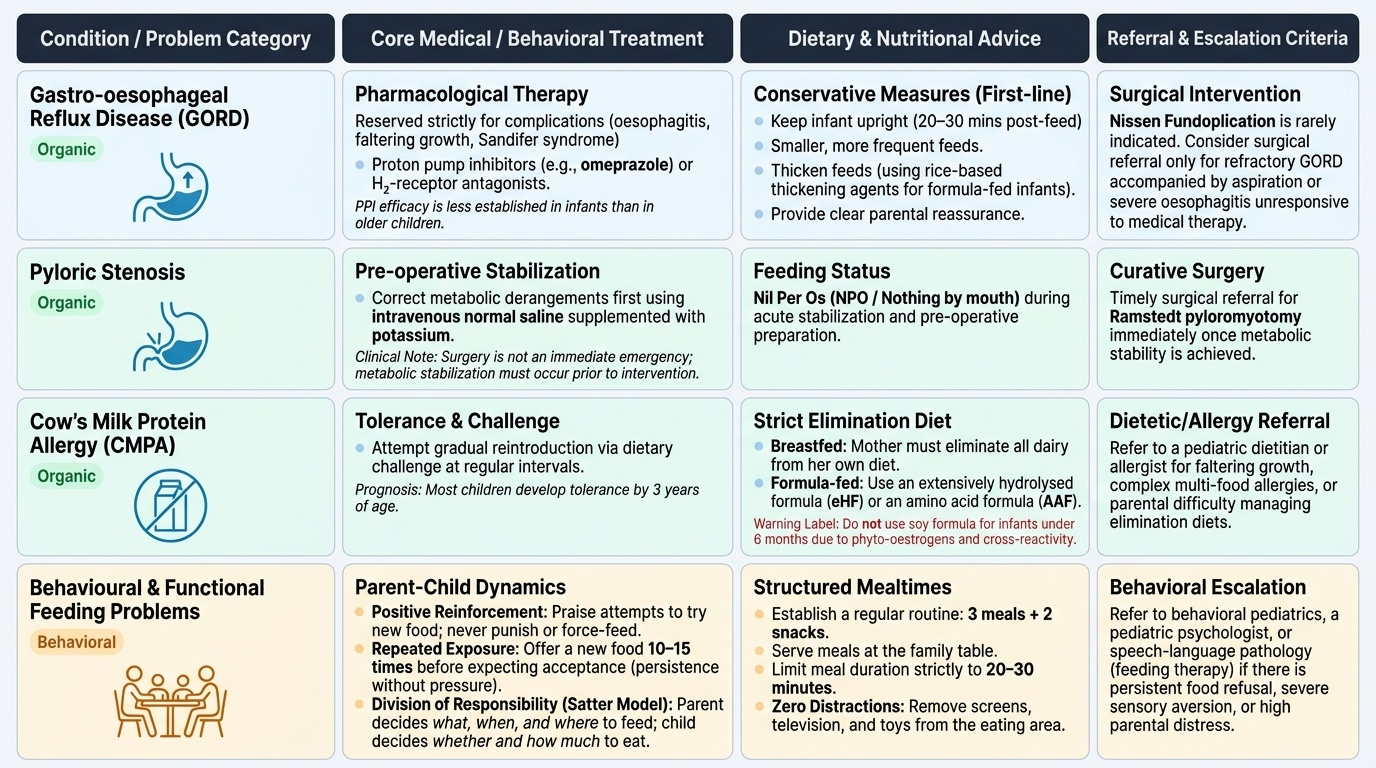
Organic causes — specific treatments:
GORD: Conservative measures are the first line and suffice for the majority of physiological GOR: reassure parents, thicken feeds (rice-based thickening agents for formula-fed infants), position upright after feeds for 20–30 minutes, smaller more frequent feeds. Pharmacological therapy (proton pump inhibitors such as omeprazole, or H₂-receptor antagonists) is reserved for GORD with complications (oesophagitis, faltering growth, Sandifer syndrome); note that PPI efficacy in infants is less established than in older children. Surgical fundoplication (Nissen) is rarely needed — considered only for refractory GORD with aspiration or severe oesophagitis unresponsive to medical therapy.
Pyloric stenosis: Surgical management — Ramstedt pyloromyotomy — is curative. Before surgery, metabolic derangements must be corrected with intravenous normal saline with potassium supplementation. Surgery is not an emergency (the metabolic derangement must be corrected first), but once stabilised, timely surgical referral is essential.
CMPA: Elimination of cow's milk protein from the diet is curative. In breastfed infants, the mother eliminates all dairy from her own diet; in formula-fed infants, an extensively hydrolysed formula (eHF) or amino acid formula (AAF) is used. Soy formula is not recommended for infants under 6 months due to phyto-oestrogens and possible cross-reactivity. Most children with CMPA develop tolerance by 3 years; reintroduction is attempted by dietary challenge at regular intervals.
Behavioural and functional feeding problems:
The foundation of management is parental education and modification of mealtime dynamics:
- Structured mealtimes: Regular mealtimes (3 meals + 2 snacks), at the family table, with a duration of 20–30 minutes; remove distractions (TV, screens).
- Positive reinforcement: Praise for any attempt to try a new food; never punish or force-feed.
- Repeated exposure: A new food may need to be offered 10–15 times before acceptance; parental persistence (without pressure) is key.
- Division of responsibility (Ellyn Satter model): The parent is responsible for what, when, and where food is offered; the child is responsible for whether and how much they eat. This reduces mealtime conflict.
- Avoid coercive or pressuring feeding strategies: Force-feeding, large distraction, and bargaining reinforce refusal and worsen the problem.
- Appetite regulation: Avoid grazing (constant snacking), excessive juice intake, and large milk volumes that suppress appetite for solid foods.
Nutritional rehabilitation: Children with documented nutritional deficiency require micronutrient supplementation and, in cases of SAM or MAM, structured rehabilitation per WHO/UNICEF protocols (F-75 and F-100 therapeutic milks for SAM; ready-to-use therapeutic food — RUTF — for community management).
Referral criteria: Refer to a paediatric dietitian for structured diet counselling; to a developmental paediatrician or occupational therapist specialising in feeding therapy if oral-motor or sensory processing issues are identified; to a paediatric surgeon for pyloric stenosis or structural anomalies; to a paediatric gastroenterologist for refractory GORD or suspected eosinophilic oesophagitis.
CLINICAL PEARL
Never force-feed a child. Force-feeding is a major risk factor for converting a transient feeding difficulty into a post-traumatic feeding disorder. At mealtimes, the child should feel in control — offer appropriate food, sit together, and accept that the child may eat less some days. Pressure and coercion increase cortisol, reduce appetite, and teach the child to associate eating with fear. The Ellyn Satter 'division of responsibility' framework — parent provides, child decides — is evidence-based and dramatically reduces mealtime conflict when families adopt it consistently. Also remember: a toddler's appetite is highly variable from day to day; a single day of poor eating is normal, not a feeding problem.
SELF-CHECK
A 10-month-old infant, exclusively breastfed, develops blood-streaked mucousy stools and poor weight gain at 4 months when formula supplementation was introduced. The mother stopped formula but the blood in stool recurred when she occasionally used it. The infant is otherwise well and has no vomiting or rash. The most appropriate management is:
A. Switch to soy-based formula
B. Maternal elimination of all dairy from diet and, if formula needed, use an extensively hydrolysed formula
C. Start oral omeprazole
D. Refer urgently for colonoscopy
Reveal Answer
Answer: B. Maternal elimination of all dairy from diet and, if formula needed, use an extensively hydrolysed formula
This presentation is classic for non-IgE-mediated cow's milk protein allergy (CMPA) — specifically allergic proctocolitis, characterised by blood-streaked stool in an otherwise well infant in response to CMP. Management: if breastfeeding, the mother eliminates all dairy; if formula supplementation is needed, an extensively hydrolysed formula (eHF) or amino acid formula (AAF) is used. Soy is not recommended under 6 months due to phyto-oestrogens and ~50% cross-reactivity. Omeprazole is for GORD. Urgent colonoscopy is not the first step in a well infant with classic CMPA.
Self-Assessment
Having worked through the clinical presentation, pathophysiology, diagnosis, and management of feeding problems, you are now ready to consolidate your understanding. The essential insight from this module is that most childhood feeding problems are behavioural rather than organic, and the most important clinical skill is distinguishing the minority with a treatable organic cause from the majority who require mealtime counselling and reassurance. Growth monitoring — using weight-for-height z-scores and MUAC — is your objective anchor throughout. Accurate classification into organic, behavioural, or developmental categories directs treatment efficiently and avoids unnecessary investigations in the majority of children. The specific organic diagnoses — GORD, pyloric stenosis, CMPA — each have distinctive features and targeted management that you should be able to apply in clinical scenarios. Use the points below as a revision checklist before attempting the self-assessment questions.
- Feeding problems are common (25–45% in normally developing children), with organic causes being a minority.
- The three categories are: organic (GORD, pyloric stenosis, CMPA, structural, neuromuscular), behavioural/functional, and developmental.
- Red flags requiring urgent evaluation: projectile/bilious vomiting, dysphagia, recurrent aspiration, blood in stool, faltering growth (>2 centile line drop).
- Pyloric stenosis: projectile non-bilious vomiting at 3–6 weeks, olive mass, hypochloraemic hypokalaemic metabolic alkalosis → ultrasound → Ramstedt pyloromyotomy after metabolic correction.
- CMPA management: maternal dairy elimination (if breastfed) or extensively hydrolysed/amino acid formula.
- Behavioural management: structured mealtimes, division of responsibility, repeated exposure, avoid force-feeding.
- SAM = WHZ < −3 SD OR MUAC <11.5 cm (6–59 months) OR bilateral pitting oedema.