Page 8 of 17
PE5.3 | Temper Tantrums and Pica — SDL Guide (Part 2)
Management
Management of both temper tantrums and pica requires addressing the underlying aetiology, providing education to parents, and implementing targeted behavioural or pharmacological strategies. The approach differs markedly between the two conditions: temper tantrums require no medical investigation and are managed entirely through parental guidance, while pica management is driven by the underlying cause identified on investigation. For both conditions, parental understanding and consistent application of the recommended approach are the determinants of success — the paediatrician's role is therefore educational as much as prescriptive.
Provided image
Management of temper tantrums:
The foundation is parental education about the developmental basis of tantrums — parents must understand that tantrums are normal, not manipulative, and that the child is genuinely overwhelmed rather than deliberately naughty. This reframing is essential before introducing specific strategies, as parents who view tantrums as deliberate provocation are more likely to respond with anger or capitulation, both of which worsen the behaviour pattern.
Key strategies:
- Positive attention and praise for good behaviour: Toddlers seek parental attention; provide ample praise when the child behaves well (positive reinforcement).
- Planned ignoring during the tantrum: Once a tantrum begins (with no risk of injury), the parent should calmly ignore it — no eye contact, no talking, no giving in. Attending to a tantrum (by comforting, scolding, or capitulating) reinforces it.
- Prevention: Keep a predictable routine; avoid known triggers (hunger, tiredness, over-stimulation); give advance warnings before transitions ('we are leaving in 5 minutes').
- Offer limited choices: 'Do you want the red cup or the blue cup?' — preserves the child's sense of autonomy within safe boundaries, reducing frustration-triggered tantrums.
- Consistent consequences: If a limit is set, it must be maintained — inconsistency is the most common reason tantrums escalate and persist.
- Time-out (for children ≥3 years): a brief, non-punitive removal from the situation (1 minute per year of age) used consistently for dangerous or highly disruptive behaviour.
- Never capitulate to a tantrum — giving the child what they want after a tantrum is the most powerful way to increase future tantrum frequency.
Referral to a developmental paediatrician or child psychologist is indicated if tantrums persist beyond 5 years, are associated with developmental delay, or are accompanied by self-injury.
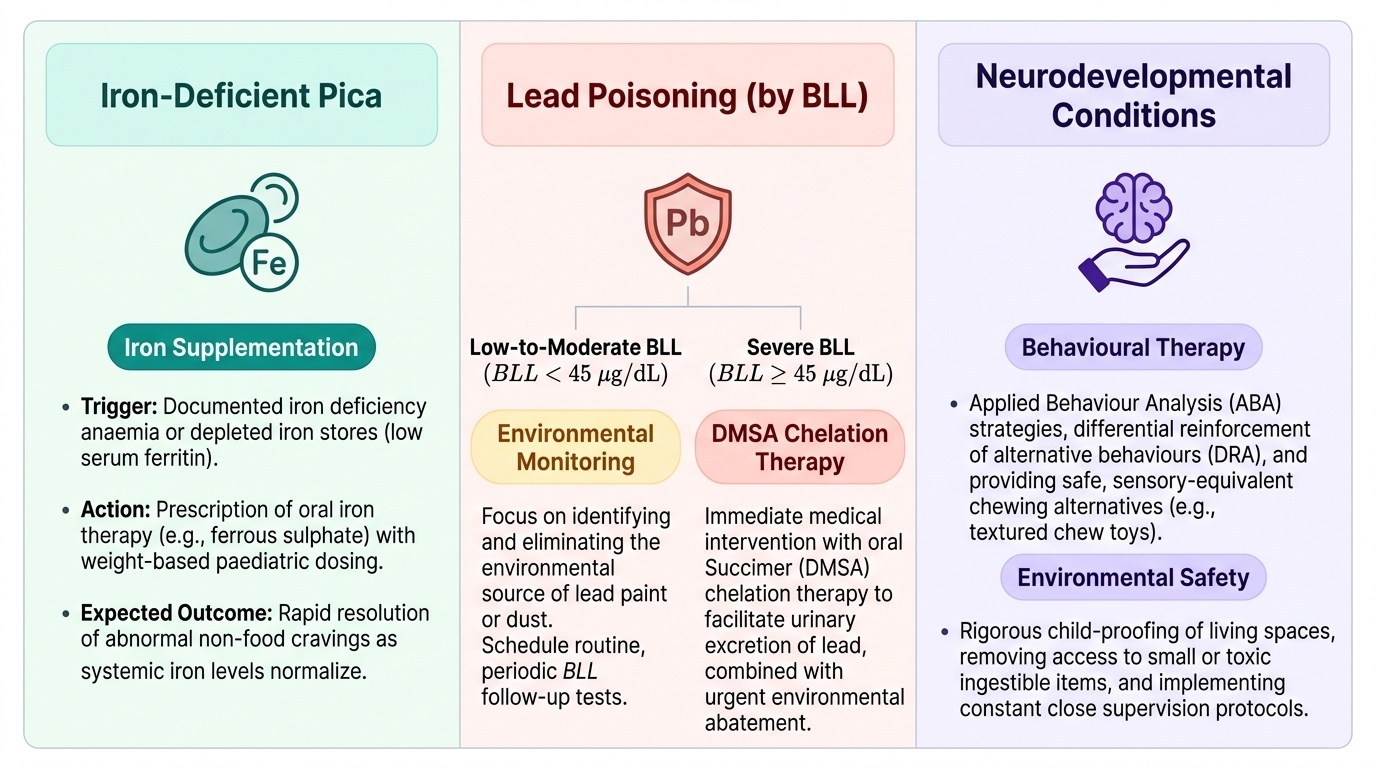
Management of pica:
Iron supplementation: Correct iron deficiency with elemental iron 3–6 mg/kg/day in divided doses for 3 months; repeat FBC and ferritin at 3 months. In the majority of iron-deficient children, iron supplementation alone resolves pica. Continue dietary iron counselling (iron-rich foods, vitamin C with meals).
Lead poisoning management (by BLL):
- BLL <5 µg/dL: No chelation; repeat BLL in 3 months; environmental investigation to remove lead source; correct iron deficiency.
- BLL 5–44 µg/dL: Repeat BLL to confirm; remove lead source; treat iron deficiency; repeat BLL every 1–3 months; refer to paediatrician for follow-up; no chelation in this range.
- BLL ≥45 µg/dL: Chelation with DMSA (dimercaptosuccinic acid, succimer) 10 mg/kg/dose three times daily for 5 days, then twice daily for 14 days; hospitalise if BLL >70 µg/dL; remove from lead source before and during chelation; monitor FBC, liver function, and renal function during chelation.
- Environmental remediation: Identify and remove the lead source (wet-dust old paint surfaces; replace kajal with lead-free alternatives; repair deteriorating old paint).
Behavioural strategies for pica: Physical barriers (covering soil in the yard, locking access to hazardous materials); applied behaviour analysis (ABA) techniques for children with intellectual disability or ASD; close supervision.
Underlying conditions: Treat iron deficiency in all; nutritional rehabilitation for SAM; referral to developmental paediatrician for ASD/intellectual disability.
SELF-CHECK
A 5-year-old boy with intellectual disability has been eating paint chips from the walls of his old house. Blood lead level returns at 55 µg/dL. He has pallor but no encephalopathy. Serum ferritin is low. What is the most appropriate immediate management?
A. Oral iron supplementation alone and repeat BLL in 6 months
B. Intravenous calcium EDTA chelation and immediate hospitalisation
C. DMSA (succimer) chelation with environmental lead source removal and iron supplementation
D. Activated charcoal and gastric lavage
Reveal Answer
Answer: C. DMSA (succimer) chelation with environmental lead source removal and iron supplementation
BLL ≥45 µg/dL in a child with symptomatic exposure (paint chips, pallor) warrants chelation. DMSA (dimercaptosuccinic acid/succimer) is the first-line oral chelating agent (10 mg/kg/dose TDS for 5 days, then BD for 14 days). Intravenous calcium EDTA is reserved for BLL >70 µg/dL or when oral therapy is not feasible. Iron supplementation corrects the coexisting iron deficiency (which amplified lead absorption) — both must be addressed. Environmental remediation (removing the lead paint source) is essential before/during chelation. Oral iron alone is insufficient at this BLL. Activated charcoal is for acute ingestion, not chronic lead poisoning.
Self-Assessment
You have now covered the clinical features, pathophysiology, diagnosis, and management of both temper tantrums and pica. These two conditions represent opposite ends of the behavioural spectrum: tantrums are developmentally normal and almost never require medical investigation, while pica — particularly in its soil-eating and paint-eating forms — carries real medical risks that demand systematic evaluation. The key clinical skill for tantrums is accurate developmental contextualisation and parental guidance; the key skill for pica is recognising and investigating the underlying nutritional and neurodevelopmental causes. Review the following checklist before attempting the self-assessment questions — ensure you can confidently explain each point in plain language, as if counselling a parent or defending your answer in an examination vignette involving a toddler with soil-eating or frequent meltdowns.
- Temper tantrums: normal 18 months–3 years; pathological if >5/day, persist >5 years, or associated with self-injury/developmental delay.
- Pica: pathological only ≥18–24 months; geophagy most common in India; pagophagia strongly associated with iron deficiency.
- Iron deficiency is the most common correctable cause of pica; ALWAYS screen with FBC + serum ferritin.
- Lead poisoning: BLL ≥5 µg/dL = reference level; BLL ≥45 µg/dL = DMSA chelation; iron deficiency amplifies lead absorption via DMT-1.
- Burton's lead line (gingival blue-black line) = chronic lead poisoning; basophilic stippling on smear.
- Tantrum management: planned ignoring, positive reinforcement, consistent limits, no capitulation.
- Pica management: correct iron deficiency + environmental remediation + chelation if BLL ≥45 µg/dL.