Page 1 of 28
PE6.1-3 | Adolescent Development — SDL Guide
Learning Objectives
- Define adolescence and describe its stages using the WHO classification
- Describe the sequence of physical, physiological, and psychological changes during puberty using Tanner/SMR staging
- Enumerate the common general health problems affecting adolescents in India
- Describe national programmes — RKSK, AFHC, and WIFS — and apply the HEEADSSS psychosocial assessment framework in clinical practice
INSTRUCTIONS
Adolescents constitute 20–22% of India's population, yet they occupy a peculiar clinical blind spot — neither children nor adults. Their developmental transitions create unique vulnerabilities: reproductive health concerns, nutritional anaemia, mental health challenges, and risk-taking behaviours. Understanding normal adolescent development is the essential clinical foundation for recognising what is pathological. This module builds the knowledge you need before encountering adolescents in the OPD, providing the anatomical, physiological, and psychological frameworks alongside the Indian national programmes designed to address adolescent health needs.
References
- Ghai Essential Pediatrics, 9th ed., Chapter on Adolescent Health (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Part VI — Adolescent Medicine (textbook)
- IAP Standard Treatment Guidelines — Adolescent Health, 2022 (guideline)
- Rashtriya Kishor Swasthya Karyakram (RKSK), MoHFW, Government of India, 2014 (programme)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 13-year-old girl is brought to the paediatric OPD by her mother who is worried: her daughter has started developing breast buds, has had a growth spurt of 7 cm in the past year, and has become moody and secretive. The mother asks, 'Is something wrong with her?' Meanwhile, the girl herself is embarrassed and wants to know what is happening to her body. As the treating doctor, you need to reassure both the mother and the girl, explain where this child is in her pubertal journey, anticipate what comes next, and screen for any health concerns — all within a 10-minute consultation.
WHY THIS MATTERS
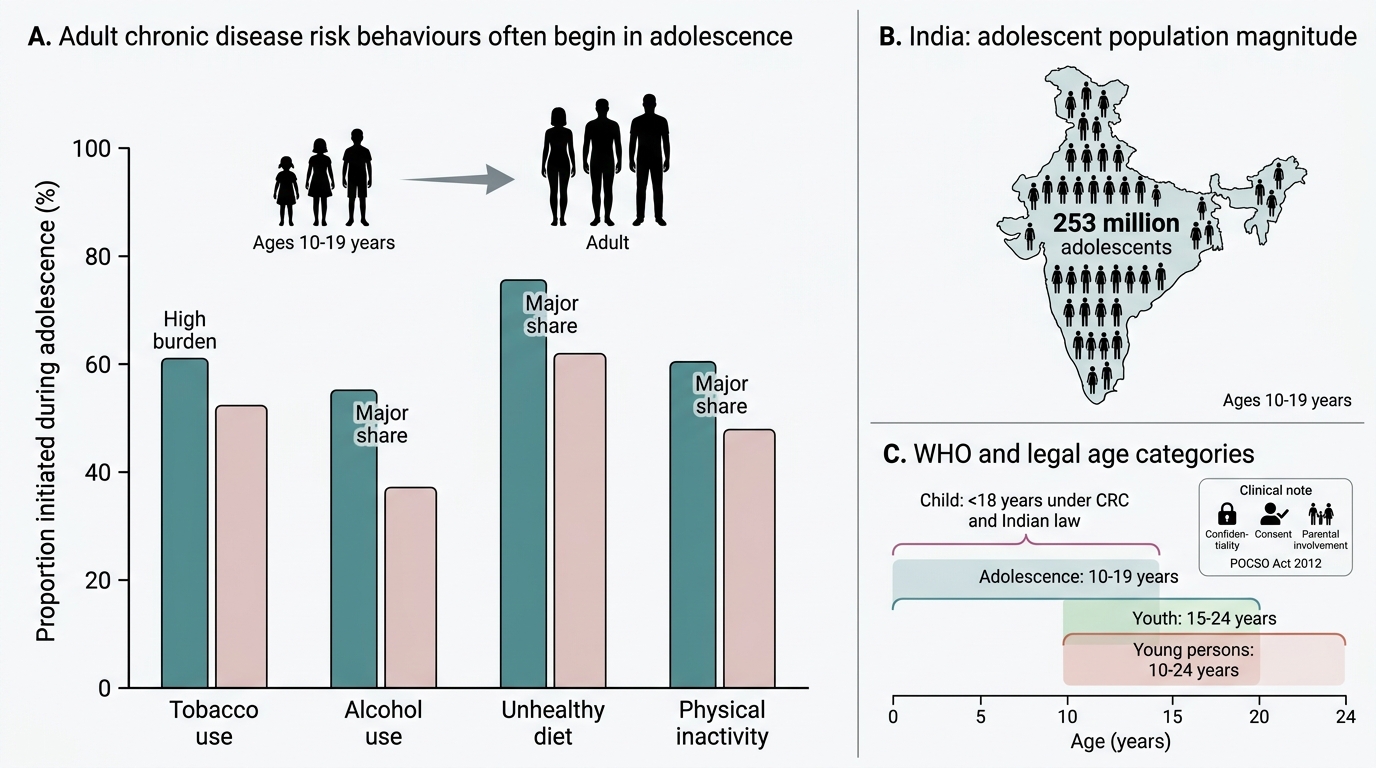
Adolescence is not merely a social label — it is a biologically driven developmental window during which the body transforms, the brain rewires, and identity consolidates. Paediatricians and family physicians are the first-contact providers for adolescents, yet medical training historically under-emphasises this age group. India has approximately 253 million adolescents (10–19 years), making it the country with the largest adolescent population in the world. Health behaviours established during adolescence — dietary habits, physical activity, risk-taking, sexual debut — have lifelong consequences. Recognising normal pubertal development allows you to identify precocious puberty, constitutional delay, primary amenorrhoea, and psychosocial distress early. The national RKSK programme now mandates dedicated adolescent health services in every block-level health system, and HEEADSSS screening is the evidence-based tool for psychosocial risk detection. This module gives you the foundation for all subsequent adolescent health competencies in this cluster.
RECALL
Before engaging with pubertal physiology, recall from your Year-1 Physiology the hypothalamic-pituitary-gonadal (HPG) axis: GnRH from the hypothalamus stimulates LH and FSH from the anterior pituitary, which drive gonadal steroid production (oestrogen from ovaries, testosterone from testes). In the prepubertal child, this axis is suppressed by inhibitory tone from the CNS. Recall also from your Paediatrics growth-and-development sessions the concept of growth velocity and the role of growth hormone, as the pubertal growth spurt is driven by both gonadal steroids and GH surge. Recall the WHO definition of childhood (0–9 years) as context for understanding where adolescence begins.
Why Adolescence Matters in Clinical Paediatrics
Adolescence is a distinct phase of human development that marks the biological, psychological, and social transition from childhood to adulthood. It is not simply the teenage years: the World Health Organization (WHO) defines adolescence as the period from 10 to 19 years of age, making it a decade-long developmental epoch that encompasses puberty, identity formation, and the acquisition of adult cognitive capacities. India's adolescent population — approximately 253 million individuals, roughly 21% of the nation's total — is the largest of any country in the world, giving this phase both immense individual importance and enormous public-health significance.
The clinical relevance of adolescent health has historically been under-appreciated in medical education because adolescents are biologically healthy by most disease-burden metrics — they have the lowest mortality rates of any age group. Yet this obscures a critical reality: adolescence is the seeding period for the chronic disease burden of adulthood. Nutritional anaemia, obesity, type 2 diabetes risk, mental health disorders, sexually transmitted infections, substance use disorders, and risk-taking injuries all have their roots in adolescent health behaviour. The WHO estimates that 16% of the global burden of disease and 70% of premature adult deaths are attributable to health-risk behaviours initiated during adolescence.
For the clinician, understanding adolescent development serves three core purposes: (1) recognising normal pubertal variation so that constitutional delay or precocity is not missed; (2) conducting developmentally appropriate clinical interviews that respect adolescent autonomy and confidentiality; and (3) deploying evidence-based screening tools such as HEEADSSS to identify psychosocial risk before it becomes clinical disease. The paediatrician, family physician, or adolescent-medicine specialist who grasps normal development is best equipped to identify pathology.
Adolescent Health Burden and Age Classification
Defining and Staging Adolescence
The WHO classification of adolescence and youth uses overlapping but distinct age categories that carry specific programmatic and clinical implications, and which the practising clinician must not conflate. Adolescence is defined by the World Health Organization as spanning 10 to 19 years of age — a decade-long window that encompasses the entirety of puberty, the maturation of the adolescent brain, and most of the psychosocial transition to adulthood. Youth is a broader WHO category covering ages 15 to 24 years, most commonly deployed in reproductive health, labour-force, and vocational-programme contexts. Young persons is the most encompassing term, defined as ages 10 to 24 years, used in policy documents that address the entire adolescent-to-early-adult spectrum. Children, under the UN Convention on the Rights of the Child and under Indian law (the Juvenile Justice Act, 2015), refers to all persons under 18 years of age — creating a legal overlap where a 16-year-old is simultaneously an adolescent (WHO definition) and a child (Indian law). This dual classification has direct clinical implications: informed consent, confidentiality, the applicability of the POCSO Act 2012, and the duty to involve parents all depend on which framework is operative. For clinical and public-health purposes, the RKSK programme and NMC CBME competencies use the WHO 10–19 year definition as the primary working boundary.
Within adolescence, three sub-stages are commonly used in clinical practice to calibrate communication style, developmental expectations, and the domains of anticipatory guidance that are most relevant to the patient in front of you. These stages reflect the progression of both biological puberty and psychosocial development, and they guide the clinician in deciding whether to include parents in a consultation, whether to use concrete or abstract language, and which health risks to probe most urgently.
| Sub-stage | Age band | Dominant features |
|---|---|---|
| Early adolescence | 10–13 years | Onset of puberty, concrete thinking still dominant, parent-child relationship central |
| Middle adolescence | 14–16 years | Rapid pubertal completion, peer group primacy, risk-taking behaviours peak, identity exploration begins |
| Late adolescence | 17–19 years | Pubertal completion, abstract reasoning consolidated, emerging adult identity, career and relationship planning |
This staging is not merely academic. A 10-year-old in early adolescence needs factual, parent-assisted communication about pubertal changes, while a 17-year-old in late adolescence requires confidential one-on-one consultation about reproductive health, vocational choices, and mental health. Clinically, the stage also guides what is normal: a 10-year-old girl beginning thelarche is at the expected boundary; a 7-year-old with the same finding requires investigation for precocious puberty.
Physical and Physiological Changes — Puberty and the Tanner/SMR Stages
Puberty is the biological process by which a child acquires secondary sexual characteristics and reproductive capacity. It is initiated by disinhibition of the HPG axis: a rise in pulsatile GnRH release triggers increased LH and FSH, which stimulate ovarian oestrogen and testicular testosterone production. The adrenal cortex contributes independently through adrenarche — DHEAS-driven pubic and axillary hair growth — which can precede gonadal puberty.
Provided image
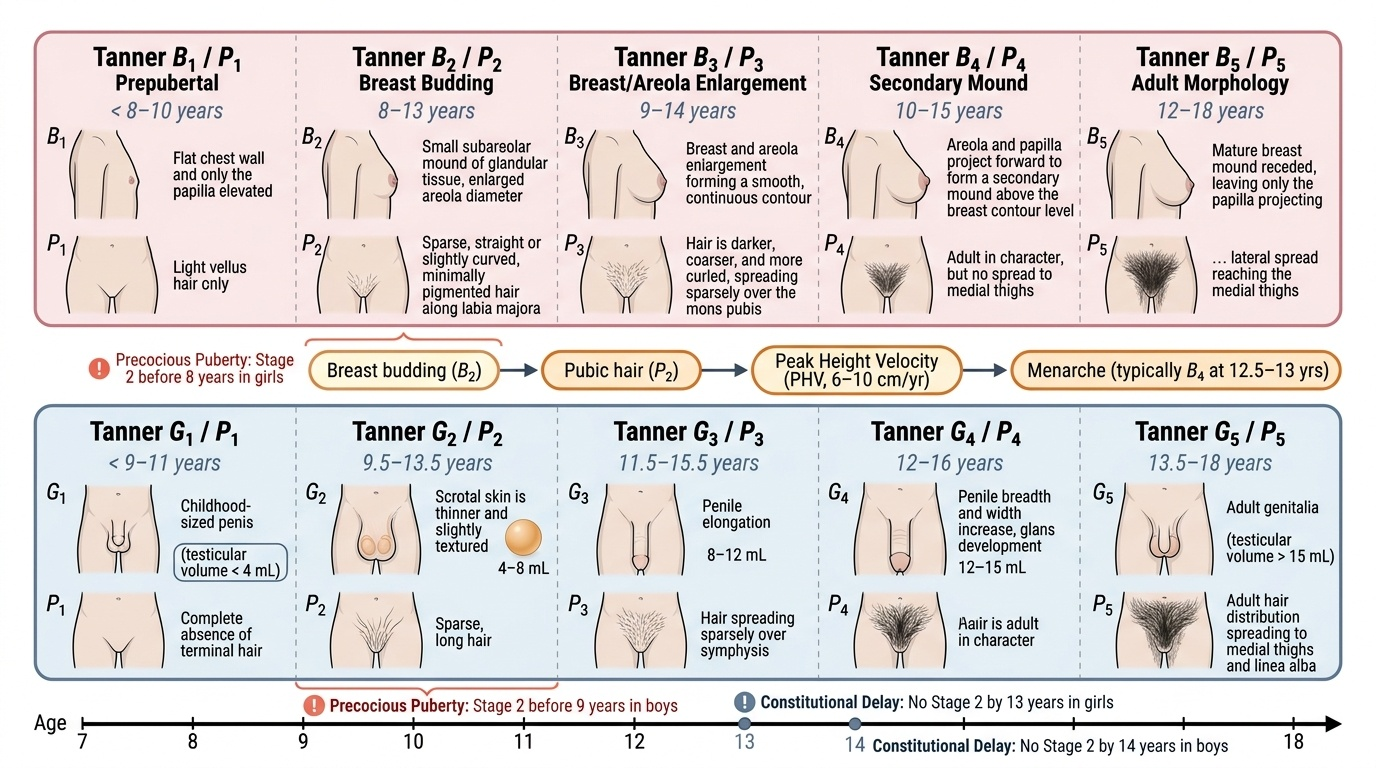
The Tanner staging system (also called Sexual Maturity Rating, SMR) provides a standardised 5-stage framework for assessing pubertal progression in clinical practice. Stages 1–5 describe the sequential anatomical changes in (a) breast development in girls, (b) genital development in boys, and (c) pubic hair growth in both sexes. Tanner Stage 1 = prepubertal baseline; Tanner Stage 5 = adult morphology. The system allows clinicians to record pubertal progress objectively and to diagnose precocious puberty (Stage 2 before 8 years in girls, 9 years in boys) or constitutional delay (no Stage 2 by 13 years in girls, 14 years in boys).
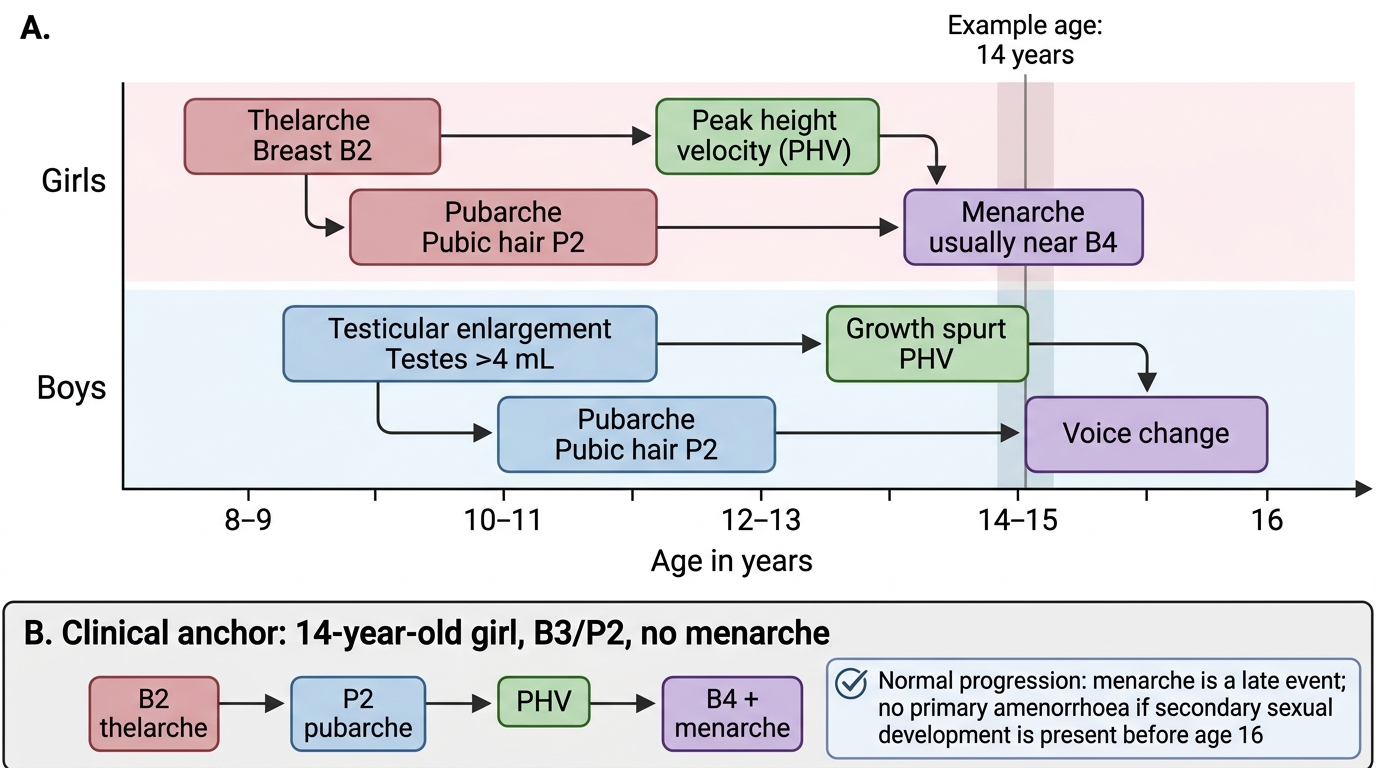
In girls, the typical pubertal sequence follows the mnemonic B-PGM: Breast budding (thelarche, usually Tanner B2) appears first → pubic hair (pubarche, Tanner P2) → peak height velocity (PHV, a growth spurt of 6–10 cm/yr) → menarche (first menstrual period, typically Tanner B4). In India, the mean age of menarche is approximately 12.5–13 years (Ghai Essential Pediatrics). Menarche arrives late in the pubertal sequence; a girl's height potential is largely utilised before her first period.
In boys, the sequence begins with testicular enlargement (Tanner G2, testicular volume ≥4 mL by Prader orchidometer) → pubic hair (Tanner P2) → penile growth (Tanner G3) → PHV (growth spurt: 8–12 cm/yr, typically 1–2 years later than girls, peaking at Tanner G4) → voice change (deepening due to laryngeal growth driven by testosterone) → facial hair as late puberty matures.
Key physiological changes accompany the anatomical progression:
- Body composition: girls gain adipose tissue (fat redistribution to hips/breasts); boys gain lean muscle mass and lose relative fat percentage driven by testosterone.
- Bone mineral density: rapid accrual during puberty — peak bone mass is achieved by late adolescence; calcium and vitamin D sufficiency is critical during this window.
- Cardiovascular/metabolic: cardiac output increases, blood pressure rises to adult levels; basal metabolic rate is high.
- Sleep architecture: delayed sleep-phase tendency in mid-adolescence is physiological (driven by melatonin timing shift), not laziness.
Pubertal Sequence in Girls and Boys
SELF-CHECK
A 14-year-old girl has Tanner Stage 3 breast development and Tanner Stage 2 pubic hair. She has not yet had menarche. Which statement about her pubertal status is MOST accurate?
A. She has primary amenorrhoea and requires immediate gynaecological evaluation
B. She is progressing normally — menarche typically follows PHV and occurs at approximately Tanner Stage 4 breast
C. She has constitutional delay — menarche should have occurred by Tanner Stage 2 breast
D. Her pubic hair development (Tanner P2) should precede breast development — this sequence is abnormal
Reveal Answer
Answer: B. She is progressing normally — menarche typically follows PHV and occurs at approximately Tanner Stage 4 breast
Menarche is a LATE event in the pubertal sequence, typically occurring at Tanner Stage 4 breast development (B4). A girl at Tanner B3/P2 who has not yet had menarche is progressing completely normally. The expected sequence in girls is B2 (thelarche) → P2 (pubarche) → PHV → B4/menarche. Primary amenorrhoea is defined as absence of menarche by age 16 in a girl with otherwise normal secondary sexual development, or by age 14 with no signs of puberty. This girl's Tanner B3 at age 14 is within the normal range and no investigation is warranted.