Page 9 of 28
PE6.5 | Adolescent Eating Disorders — SDL Guide
Learning Objectives
- Describe the clinical presentation of anorexia nervosa and bulimia nervosa in adolescents, including the physical signs and behavioural red flags
- Apply the DSM-5 diagnostic criteria for anorexia nervosa (both subtypes) and bulimia nervosa
- Enumerate the medical complications of eating disorders, including refeeding syndrome
- Describe the management approach for adolescent eating disorders, including indications for inpatient care and the role of Family-Based Treatment
INSTRUCTIONS
Anorexia nervosa carries the highest mortality rate of any psychiatric disorder. Bulimia nervosa causes silent but progressive medical harm. Both conditions disproportionately affect adolescent girls during the developmental window most vulnerable to body image disturbance. Yet eating disorders are systematically under-diagnosed: patients minimise symptoms, families miss the signs, and clinicians are not trained to probe the specific history that reveals the diagnosis. This module gives you the DSM-5 criteria, the clinical red flags, and the initial management framework to identify and begin addressing eating disorders in your adolescent patients.
References
- Ghai Essential Pediatrics, 9th ed., Chapter on Adolescent Health — Eating Disorders (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Chapter on Eating Disorders (textbook)
- DSM-5 — Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, American Psychiatric Association, Feeding and Eating Disorders section (classification)
- IAP Standard Treatment Guidelines — Adolescent Eating Disorders, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 15-year-old girl is brought to the paediatric OPD by her mother, who is concerned about weight loss over the past eight months. The girl says she is 'just being healthy' and eating 'clean food.' Her weight is 38 kg, height 162 cm (BMI 14.5 kg/m²). She has not menstruated for six months. On examination, she has fine lanugo hair on her forearms, bradycardia (pulse 48 bpm), and dry, mottled skin. When you ask about her eating, she says she is 'not hungry' and resents being brought to the doctor. Her mother, visibly distressed, adds: 'She counts every calorie. She spends two hours on the treadmill every morning. She gets angry if we try to make her eat more.' What is the diagnosis, and what are your immediate priorities?
WHY THIS MATTERS
Eating disorders are not diet fads or attention-seeking behaviour — they are serious psychiatric illnesses with profound medical consequences. Anorexia nervosa has the highest mortality rate of any psychiatric disorder, with death occurring from medical complications of starvation (cardiac arrhythmias, organ failure) and from suicide. Bulimia nervosa is significantly more prevalent than AN, often undetected because body weight may be normal, yet it causes progressive electrolyte disturbances, dental erosion, and oesophageal damage over years of purging. Both conditions emerge predominantly during adolescence — the period of greatest biological and psychosocial vulnerability to body image disturbance. The paediatrician who does not know the DSM-5 criteria, the physical examination signs, and the initial management pathway will miss these diagnoses until they become medical emergencies.
RECALL
Recall from your nutrition cluster the parameters of malnutrition assessment: weight-for-height z-scores, BMI-for-age, MUAC. In eating disorders, the mechanism of malnutrition is behavioural restriction and/or purging rather than food scarcity, but the physiological consequences — including micronutrient deficiency, muscle wasting, immune suppression, and bone mineral loss — are the same or worse. Recall from your Basic Sciences the physiological role of oestrogen on bone mineralisation: its deficiency in amenorrhoea-related AN leads to osteopenia and osteoporosis. Recall from your Psychiatry exposure the concept of ego-syntonic conditions — where the patient does not perceive their illness as alien to their sense of self — which explains why patients with AN typically resist treatment.
Clinical Presentation of Adolescent Eating Disorders
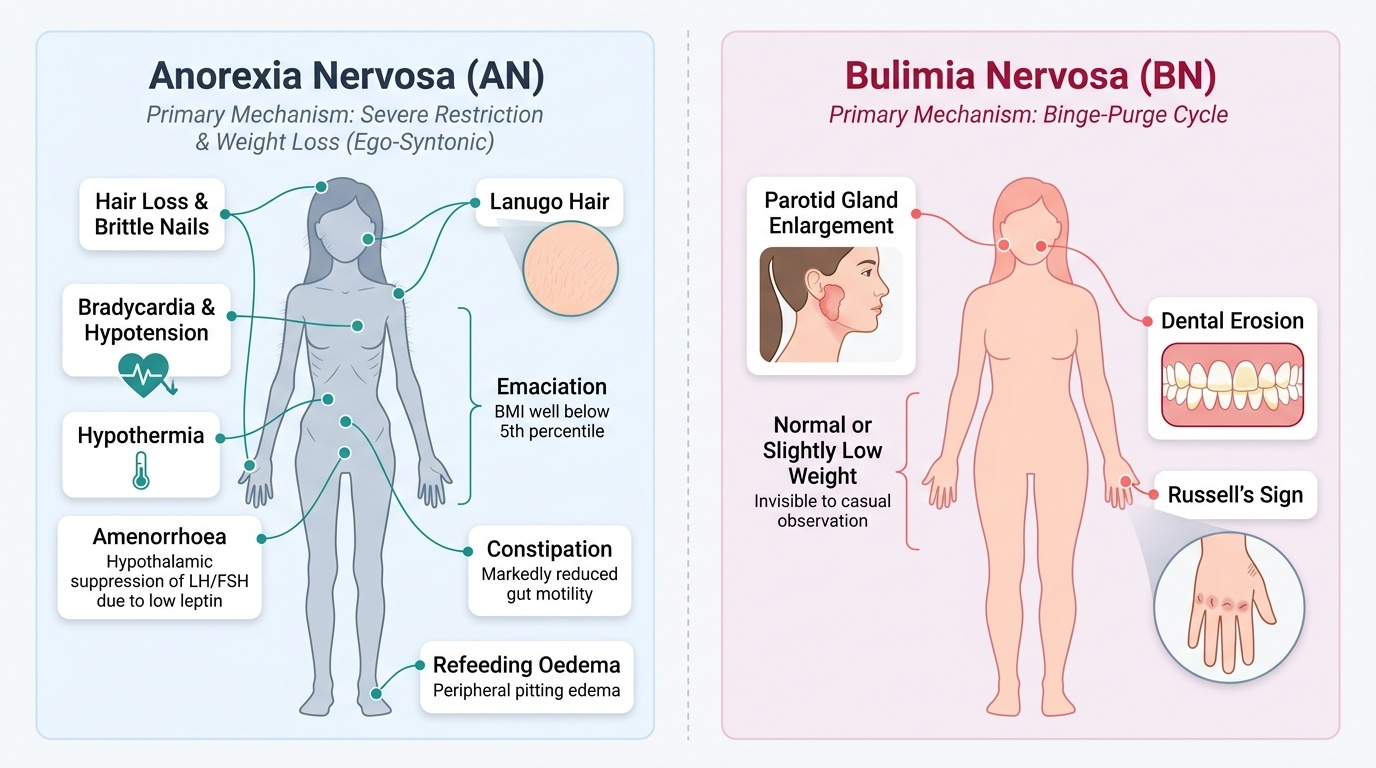
Eating disorders present through a combination of physical examination findings and behavioural and psychological features that require active, directed clinical inquiry to elicit. The two major eating disorders covered in this module — anorexia nervosa (AN) and bulimia nervosa (BN) — have overlapping but distinct presentations that reflect their different primary mechanisms (restriction in AN; binge-purge cycle in BN). Recognising these presentations is clinically essential because patients with AN almost universally deny or minimise their symptoms — AN is ego-syntonic (the patient does not experience her restriction as illness), making the history unreliable without collateral information from the family. Patients with BN may present with a normal or near-normal body weight, making the diagnosis completely invisible to the untrained eye unless the specific examination signs (Russell's sign, parotid enlargement, dental erosion) are sought. Both conditions are under-diagnosed in clinical practice, with years typically elapsing between symptom onset and correct diagnosis.
Provided image
Anorexia Nervosa — clinical presentation:
AN presents typically as progressive weight loss in an adolescent girl (onset usually 12–18 years) associated with deliberate dietary restriction, intense preoccupation with weight and food, and a distorted perception of body image. The patient insists she is 'fat' or 'needs to lose more weight' despite objective evidence of emaciation. Physical examination findings in established AN include:
- Emaciation: severe underweight, with BMI well below the 5th percentile for age (or BMI <17.5 kg/m² in adults)
- Bradycardia and hypotension: cardiac adaptations to starvation; resting heart rate may be <50 bpm
- Hypothermia: impaired thermoregulation
- Lanugo hair: fine downy hair on the trunk and extremities — a foetal pattern of thermoregulation re-emerging in severe starvation
- Primary or secondary amenorrhoea: cessation of menstruation due to hypothalamic suppression of LH/FSH (low leptin from fat depletion)
- Oedema: peripheral pitting oedema may paradoxically appear on refeeding
- Dry, mottled skin; hair loss; brittle nails
- Constipation: markedly reduced gut motility
- Parotid gland enlargement in the binge-purge subtype
Bulimia Nervosa — clinical presentation:
BN is characterised by cycles of secretive binge eating (consuming very large amounts of food rapidly, with a sense of loss of control) followed by compensatory purging behaviours. Unlike AN, most patients with BN maintain a normal or slightly above-normal body weight. Physical examination findings specific to BN:
- Russell's sign: calluses or scarring on the dorsal surface of the hand (particularly the metacarpophalangeal joints and dorsal fingers) caused by repeated trauma from the teeth during self-induced vomiting. This is a pathognomonic sign of BN purging.
- Parotid gland hypertrophy (parotitis): bilateral painless enlargement, giving the 'chipmunk cheeks' appearance, from repeated vomiting-related salivary gland stimulation
- Dental erosion: erosion of the enamel on the lingual (tongue-facing) surface of the upper front teeth by gastric acid
- Peripheral oedema: from electrolyte disturbances or rebound fluid retention after stopping laxatives
- Pharyngeal irritation, hoarseness
Behavioural red flags in both conditions: spending long periods in the bathroom after meals, exercising excessively, food rituals (cutting food into tiny pieces, eating in a particular sequence), wearing baggy clothing to hide body shape, social withdrawal at mealtimes, frequent weighing, irritability when food intake is monitored.
SELF-CHECK
A 16-year-old girl with suspected bulimia nervosa is referred to you. She has a normal BMI (20.5 kg/m²). On examination, you notice calluses on the dorsal surface of her right hand at the metacarpophalangeal joints. What is this sign called and what does it indicate?
A. Dupuytren's contracture — indicating hepatic disease from alcohol abuse
B. Russell's sign — indicating repeated self-induced vomiting as a compensatory purging behaviour in bulimia nervosa
C. Raynaud's phenomenon — indicating peripheral vascular disease from emaciation
D. Acanthosis nigricans — indicating insulin resistance from binge eating
Reveal Answer
Answer: B. Russell's sign — indicating repeated self-induced vomiting as a compensatory purging behaviour in bulimia nervosa
Russell's sign is the term for calluses or scarring on the dorsum of the hand (typically at the metacarpophalangeal joints and the dorsal knuckles) caused by repeated contact of the teeth with the hand during self-induced vomiting. It is named after Gerald Russell, who described it in 1979. It is pathognomonic (specifically diagnostic) of the purging subtype of bulimia nervosa, or of the binge-purge subtype of anorexia nervosa. Its presence in a patient with normal weight and behavioural red flags is strong clinical evidence for BN. This sign may be absent in patients who use other methods (laxatives, diuretics) to compensate for binge eating.
Pathophysiology and Aetiology of Eating Disorders
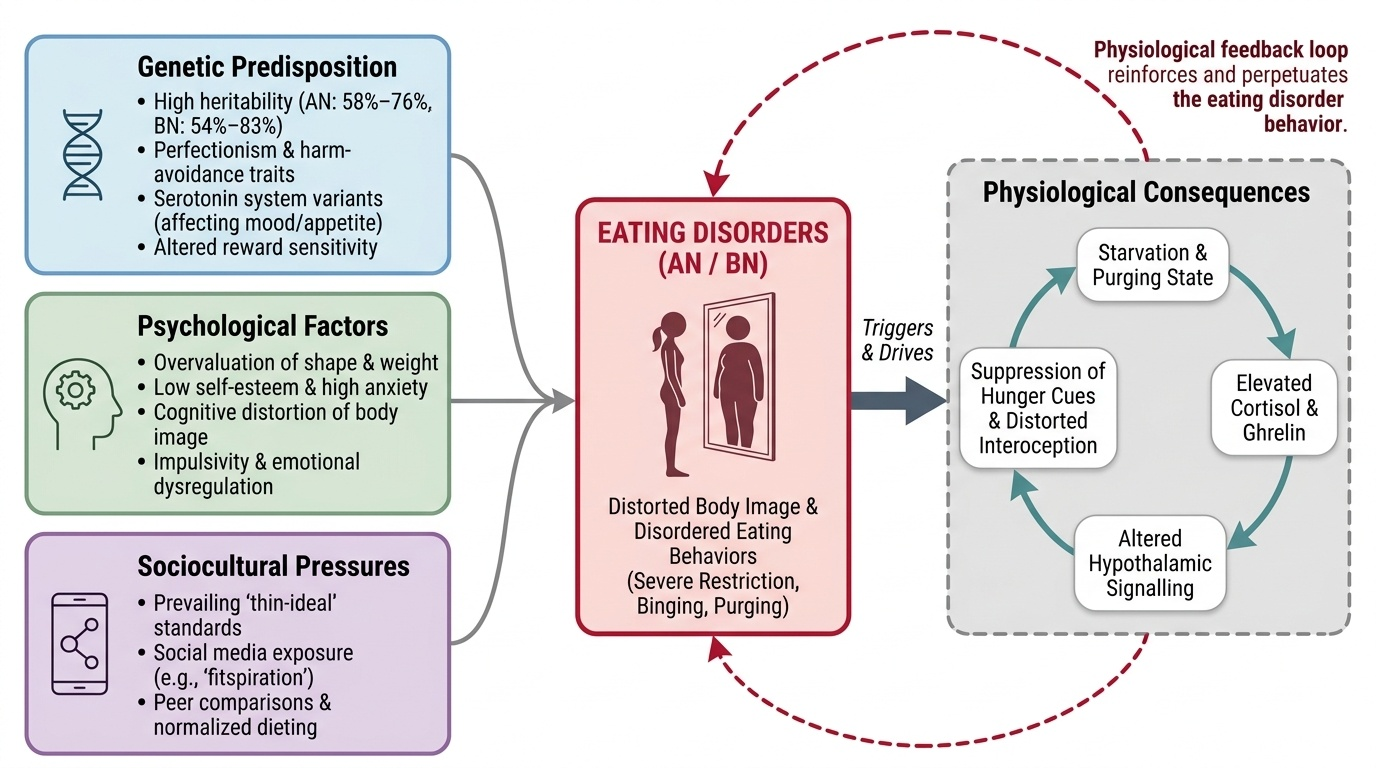
Eating disorders arise from the convergence of genetic, psychological, and sociocultural risk factors that create a vulnerability to distorted body image and disordered eating behaviours. This biopsychosocial model is the current accepted framework and is important for both understanding the disorder and explaining it to families who may wrongly attribute it to wilfulness or poor parenting.
Provided image
Genetic factors: first-degree relatives of individuals with AN have an 11-fold increased risk of AN, and twin studies show heritability estimates of 58–76% for AN and 54–83% for BN. This genetic predisposition operates through traits such as perfectionism, harm-avoidance, reward sensitivity, and serotonin system variants that influence both mood regulation and appetite.
Psychological factors: the cognitive core of AN is the overvaluation of body shape and weight as the primary determinant of self-worth, combined with a profound distortion of body image (the patient perceives herself as fat when objectively emaciated). Perfectionism, high achievement orientation, obsessive-compulsive traits, and low self-esteem are the psychological substrate on which AN typically develops. In BN, impulsivity, emotional dysregulation, and difficulty tolerating negative affect (binge eating as a coping mechanism for distress) are more prominent. Both conditions are strongly associated with comorbid depression, anxiety disorders (especially OCD, social anxiety), and a history of childhood trauma or abuse.
Sociocultural factors: the prevailing thin-ideal body standard in media, social media, fashion, and peer culture creates a cultural environment in which dieting and body dissatisfaction are normalised, particularly for adolescent girls. Social media exposure to 'fitspiration' content and peer comparisons of body image amplify the risk. The social pressure to conform to ideals of thinness is a trigger that activates genetic and psychological vulnerabilities.
Physiological consequences of the eating disorder: once established, AN creates a physiological feedback loop: starvation → elevated cortisol and ghrelin → altered hypothalamic signalling → suppression of hunger cues → perpetuation of restriction. Distorted interoception (diminished awareness of hunger and fullness) is also present. In BN, the binge-purge cycle becomes self-reinforcing through both physiological (electrolyte fluctuations driving cravings) and psychological (temporary relief of distress by purging) mechanisms.
Diagnosis — DSM-5 Criteria for Anorexia Nervosa and Bulimia Nervosa
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, APA 2013) provides the diagnostic criteria for eating disorders. Knowing these criteria precisely is essential for both diagnosis and for communicating with psychiatry teams.
Anorexia Nervosa DSM-5 Criteria:
Criterion A: Restriction of energy intake relative to requirements, leading to a significantly low body weight in the context of age, sex, developmental trajectory, and physical health. ('Significantly low' is defined as weight less than minimally expected.)
Criterion B: Intense fear of gaining weight or of becoming fat, OR persistent behaviour that interferes with weight gain, even though at a significantly low weight.
Criterion C: Disturbance in the way body weight or shape is experienced (body image distortion), undue influence of body weight or shape on self-evaluation, OR persistent lack of recognition of the seriousness of the current low body weight.
Note: the previous DSM-IV criterion of amenorrhoea has been removed in DSM-5 — this allows diagnosis in males, pre-menarchal females, and post-menopausal women.
AN Subtypes:
- Restricting type (AN-R): weight loss primarily through dieting, fasting, and/or excessive exercise
- Binge-eating/purging type (AN-BP): weight loss accompanied by recurrent binge eating and/or purging behaviour (self-induced vomiting, laxatives, diuretics)
AN Severity (based on adult BMI; in adolescents, use BMI-for-age percentiles):
- Mild: BMI ≥17 kg/m²
- Moderate: BMI 16–16.99 kg/m²
- Severe: BMI 15–15.99 kg/m²
- Extreme: BMI <15 kg/m²
Bulimia Nervosa DSM-5 Criteria:
Criterion A: Recurrent episodes of binge eating — characterised by (1) eating an amount of food in a discrete period that is definitely larger than most people would eat under similar circumstances, AND (2) a sense of lack of control over eating during the episode.
Criterion B: Recurrent inappropriate compensatory behaviour to prevent weight gain, including: self-induced vomiting; misuse of laxatives, diuretics, or other medications; fasting; or excessive exercise.
Criterion C: The binge eating and compensatory behaviours occur, on average, at least once per week for 3 months.
Criterion D: Self-evaluation is unduly influenced by body shape and weight.
Criterion E: The disturbance does NOT occur exclusively during episodes of anorexia nervosa.
BN Severity (based on frequency of compensatory behaviours per week):
- Mild: 1–3 episodes/week
- Moderate: 4–7 episodes/week
- Severe: 8–13 episodes/week
- Extreme: ≥14 episodes/week
| Feature | Anorexia Nervosa | Bulimia Nervosa |
|---|---|---|
| Body weight | Significantly low | Normal or slightly above normal |
| Core cognition | Fear of weight gain + body image distortion | Self-evaluation tied to body shape/weight |
| Compensatory behaviour | Restriction (± purging in AN-BP) | Binge-purge cycle |
| Amenorrhoea | Common (not required for DSM-5 diagnosis) | May be present; not defining |
| Self-insight | Ego-syntonic (poor insight) | Often ego-dystonic (distress about behaviour) |
| Mortality | Highest of any psychiatric disorder | Significant but lower than AN |
Investigations in a new diagnosis of AN or BN:
- Full blood count: anaemia, leucopenia, thrombocytopenia
- Serum electrolytes: hypokalaemia (purging), hyponatraemia, hypochloraemia, metabolic alkalosis (from vomiting) or metabolic acidosis (from laxatives)
- Renal function: pre-renal azotaemia
- Liver function tests: elevated transaminases in starvation
- Blood glucose: hypoglycaemia
- Thyroid function: euthyroid sick syndrome (low T3, normal TSH)
- Phosphate: pre-refeeding baseline; essential for monitoring refeeding syndrome
- Bone density (DEXA): if amenorrhoea >6 months
- ECG: QTc prolongation, bradycardia, arrhythmias