Page 13 of 28
PE6.6 | Adolescent Mental Health — SDL Guide (Part 2)
Suicidal Ideation and Self-Harm in Adolescents — Assessment and Crisis Management
Suicidal ideation and self-harm in adolescents represent the highest-stakes clinical scenario in adolescent mental health practice. Every clinician who sees adolescents must be able to conduct a structured risk assessment and make an appropriate safety plan or emergency referral.
Provided image
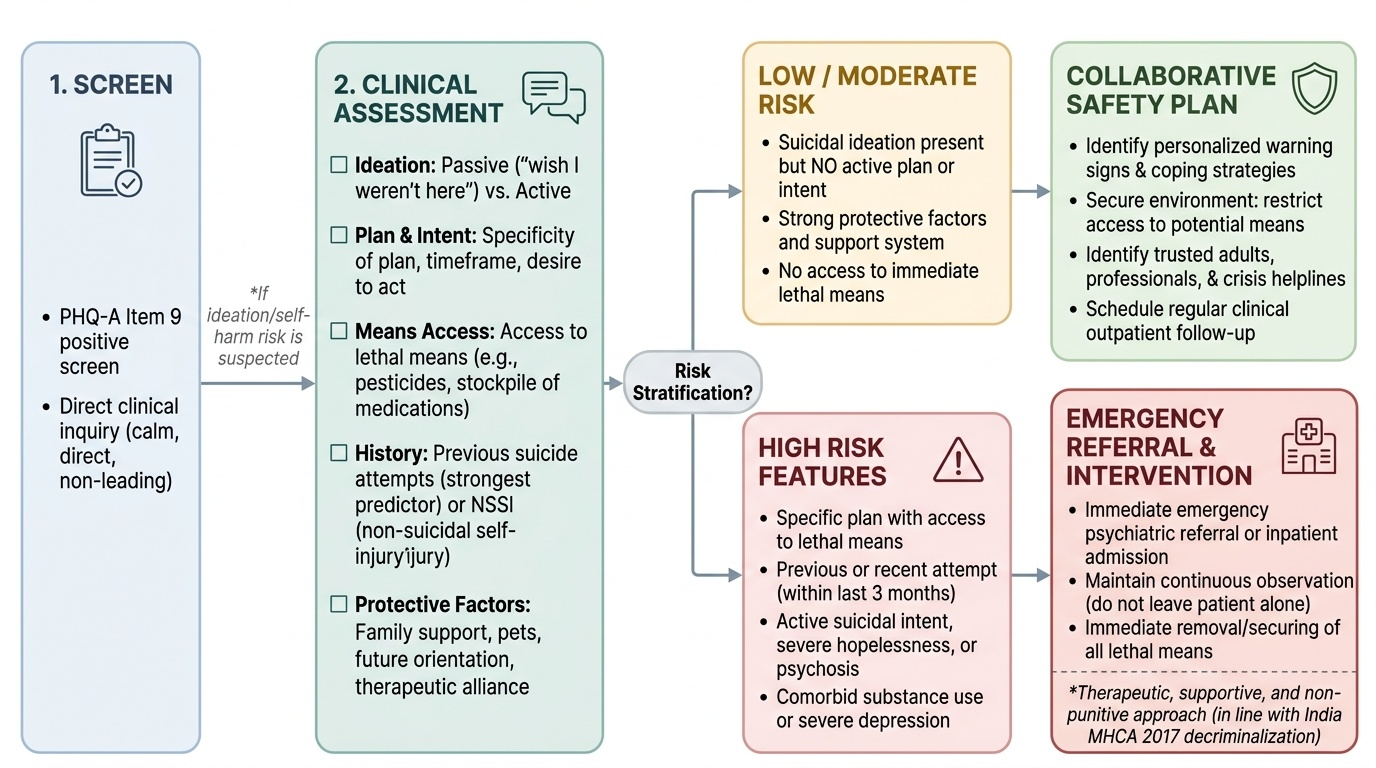
The Mental Healthcare Act 2017 (MHCA 2017) is foundational to understanding the clinical approach: Section 115 decriminalised suicide attempts in India, recognising persons who attempt suicide as being in need of care, rehabilitation, and support — not criminal punishment. This has clinical implications: the clinician's role is supportive and therapeutic, not punitive.
Distinguishing ideation from behaviour: the spectrum ranges from passive ideation ('I wish I were not here') through active ideation with varying levels of planning and intent to suicide attempt. Non-suicidal self-injury (NSSI) — self-cutting, burning, or scratching without intent to die — must be assessed as a separate but related phenomenon; NSSI significantly increases the risk of future suicide attempts.
Structured risk assessment — ask directly, calmly, without leading questions:
1. Ideation: 'Have you had thoughts of harming yourself or ending your life?'
2. Plan: 'Do you have a plan for how you would do it?'
3. Intent: 'Have you thought about actually doing it?'
4. Means access: 'Do you have access to [stated method]?' (e.g. medications, pesticides — common in India)
5. Timeframe: 'Have you thought about when?'
6. Previous attempt: 'Have you ever tried to harm yourself or end your life before?'
7. Protective factors: 'What has stopped you?' (family, religion, pets, future plans — protective factors reduce risk)
High-risk features requiring emergency psychiatric referral or inpatient admission:
- Specific plan with access to lethal means (especially pesticides, medications in stockpile)
- Previous suicide attempt (strongest predictor of future attempt)
- Recent attempt (within last 3 months)
- Active suicidal intent
- Comorbid substance use or severe depression
- Social isolation, hopelessness ('nothing will change'), intent to complete
- Psychosis
Safety planning for lower-risk situations (ideation without plan/intent):
1. Identify warning signs the adolescent notices before a crisis
2. Identify coping strategies the adolescent can use independently
3. Identify people they can reach out to (trusted adult, peer)
4. Emergency contact numbers (iCall India: 9152987821; NIMHANS helpline: 080-46110007)
5. Means restriction: work with the family to remove or secure medications, pesticides, or other identified means from the home
6. Schedule close follow-up within 1–2 weeks
CLINICAL PEARL
Asking about suicide does NOT increase the risk of suicide attempt — this is the most pervasive clinical myth that leads to under-assessment. Multiple studies confirm that directly asking a distressed adolescent about suicidal ideation does not plant the idea or increase risk; it communicates that the clinician is taking their distress seriously and creates an opening for disclosure. The adolescent who has been silently ruminating about suicide is often RELIEVED when asked directly. Frame the question matter-of-factly within a routine screen: 'When young people are going through a hard time like this, sometimes they have thoughts of hurting themselves or not wanting to be here. Has that happened for you?' This destigmatises the question and makes honest disclosure more likely than a blunt 'Are you suicidal?'
SELF-CHECK
A 16-year-old boy scores 12 on the PHQ-A (Patient Health Questionnaire — Adolescent). He endorses item 9 positively. What is the CORRECT interpretation and clinical response?
A. PHQ-A score 12 is mild — schedule routine follow-up in 6 weeks and reassure the parents
B. PHQ-A score 12 indicates moderate depression; a positive item 9 mandates immediate direct suicide risk assessment regardless of total score, followed by active treatment
C. PHQ-A is a diagnostic tool — a score of 12 confirms the DSM-5 diagnosis of MDD and pharmacotherapy should be started immediately
D. Refer to psychiatry only if the PHQ-A score exceeds 20
Reveal Answer
Answer: B. PHQ-A score 12 indicates moderate depression; a positive item 9 mandates immediate direct suicide risk assessment regardless of total score, followed by active treatment
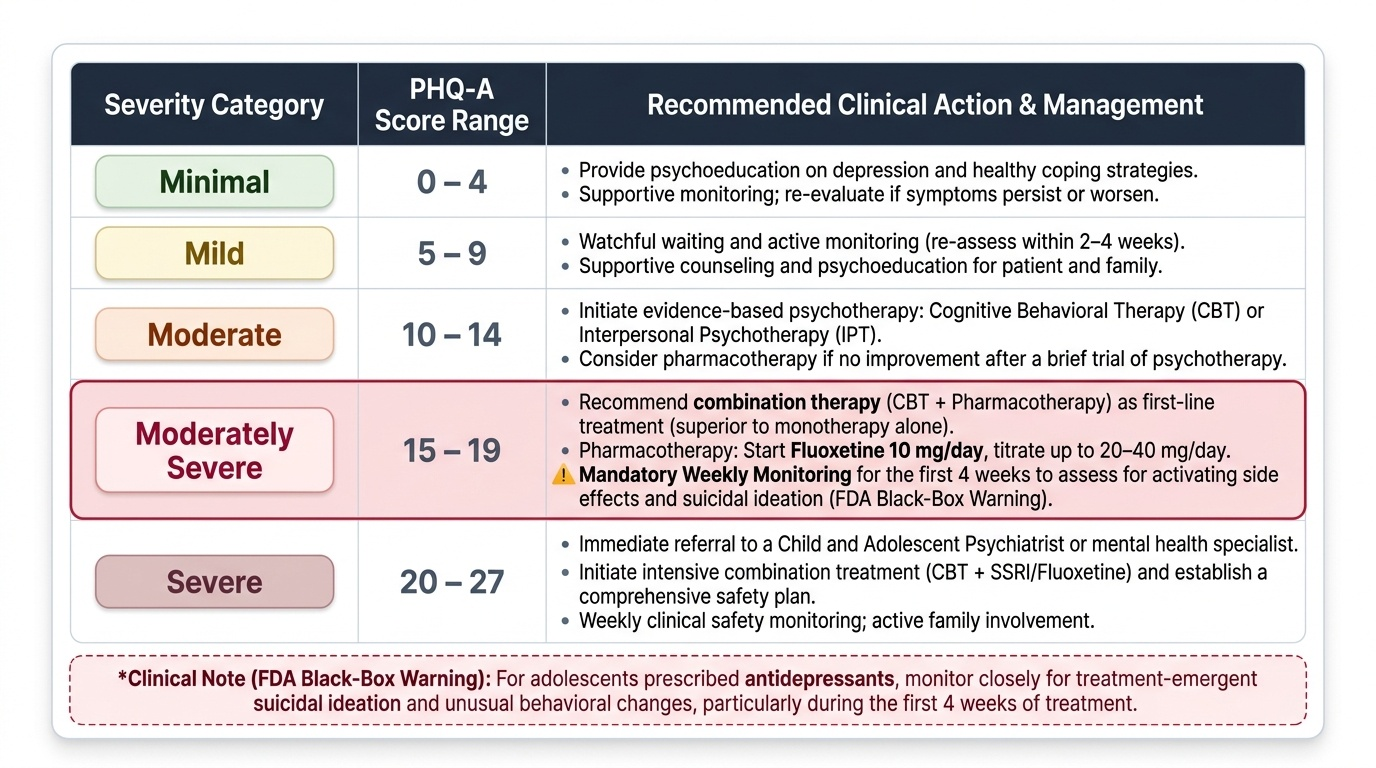
PHQ-A score 10–14 = MODERATE depression severity, which indicates the need for active treatment (CBT with or without medication). However, Item 9 of the PHQ-A asks about thoughts of self-harm or death — a positive response to Item 9 ALWAYS mandates a direct, structured suicide risk assessment, regardless of the total PHQ-A score. This is because even a low total score with a positive item 9 represents a patient at risk. The PHQ-A is a screening tool, not a diagnostic tool — it guides clinical action but does not replace the full clinical assessment. A score of 12 with a positive item 9 requires: (1) direct suicide risk assessment today; (2) active treatment plan (referral for CBT ± medication consideration); (3) safety planning with the patient and family.
Management of Common Adolescent Mental Health Problems
Management of adolescent mental health disorders follows a stepped-care model in which the least intensive, most accessible intervention is applied first, with escalation when the initial step proves insufficient within a defined time frame. This approach reflects the evidence base: most mild-to-moderate adolescent mental health problems respond to well-delivered psychosocial interventions at the primary care level, and pharmacotherapy — while evidence-based and effective for moderate-to-severe conditions — is reserved for cases where psychological intervention alone has not produced adequate improvement within an appropriate trial period. The stepped-care model has the additional advantage of matching the intensity of care to the severity of the condition, avoiding over-treatment of mild presentations while ensuring that moderate-to-severe conditions receive the combined CBT-plus-medication approach that the TADS trial and other paediatric studies have shown to be superior. The steps described below apply specifically to depression; the management of anxiety and ADHD is addressed separately.
Step 1 — Mild depression or anxiety (PHQ-A 5–9):
- Psychoeducation: explain the diagnosis to the adolescent and family in destigmatising, non-judgmental language; normalise treatment-seeking.
- Sleep hygiene: structured bedtime, limiting screens before sleep; sleep disturbance both causes and maintains depression/anxiety.
- Physical activity: evidence-based antidepressant effect; 30–60 minutes of aerobic activity on most days.
- Reduced social media exposure: limit comparison-driven social media use.
- Monitoring: schedule review in 4 weeks; if no improvement, advance to Step 2.
Step 2 — Mild-to-moderate depression and anxiety (PHQ-A 10–14):
- Cognitive Behavioural Therapy (CBT) is the first-line psychological treatment for adolescent depression and all anxiety disorders. CBT teaches the adolescent to identify and restructure negative automatic thoughts, use behavioural activation (re-engaging with rewarding activities), and apply graduated exposure for anxiety. Delivered as 8–16 sessions with a trained psychologist or counsellor.
- Interpersonal Psychotherapy for Adolescents (IPT-A): alternative to CBT; focuses on improving interpersonal relationships and resolving role transitions.
- Family involvement is important — family sessions to address communication patterns and reduce high-expressed emotion.
Step 3 — Moderate-to-severe depression (PHQ-A ≥15) or anxiety unresponsive to therapy:
- Fluoxetine is the ONLY antidepressant with robust evidence for adolescent MDD (TADS trial: fluoxetine 20–40 mg + CBT combination superior to either alone; fluoxetine superior to placebo). Dose: 10–20 mg/day initial, titrated to 20–40 mg/day. Monitor for activating side effects (agitation, insomnia, akathisia) in the first 2–4 weeks, particularly suicidal ideation (the FDA black-box warning for antidepressants in paediatric/adolescent patients — risk of increased suicidal ideation in first weeks of treatment; requires weekly monitoring at start). Benefits of treatment outweigh risk of non-treatment in moderate-severe depression.
- Combination CBT + fluoxetine is superior to either treatment alone for moderate-to-severe adolescent MDD.
- SSRIs are also first-line for adolescent anxiety disorders (especially sertraline, fluoxetine).
Step 4 — Severe depression with psychotic features, treatment-resistant, or acute suicidal risk:
- Specialist inpatient adolescent psychiatry referral.
- Electroconvulsive therapy (ECT) is an option for severe, life-threatening, treatment-resistant adolescent depression — requires specialist decision.
ADHD management in adolescents:
- Methylphenidate (short-acting: 5–10 mg BD/TDS; long-acting: OROS-MPH 18–54 mg once daily) is the first-line pharmacotherapy for moderate-severe ADHD. Weight-based dosing: 0.3–1 mg/kg/day. Monitor growth, appetite, blood pressure, and heart rate.
- Non-pharmacological: structured routines, academic accommodations (extended time for exams), parent training, organisational coaching.
- Comorbid depression or anxiety in ADHD requires integrated treatment.
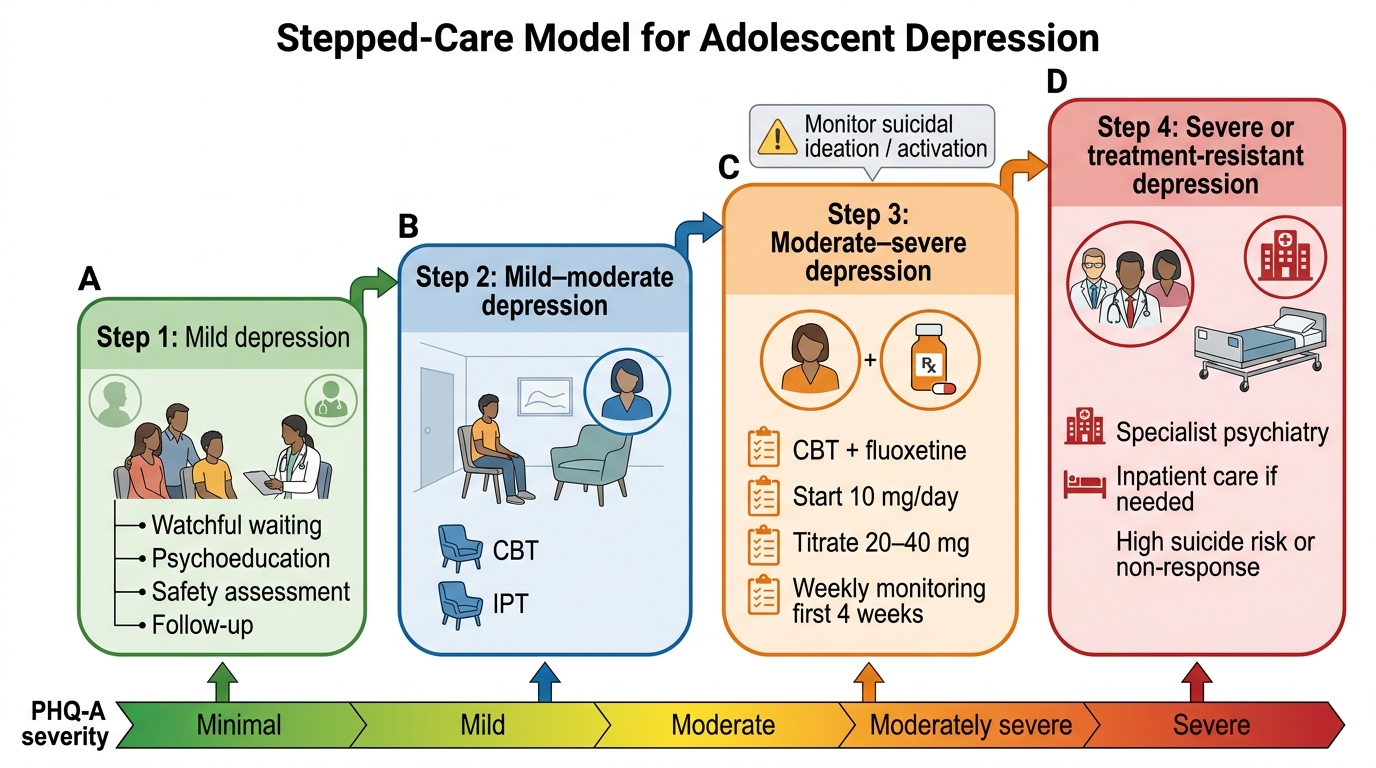
Stepped-Care Management of Adolescent Depression
Self-Assessment — Adolescent Mental Health
Test your understanding with these scenario-based questions before reviewing the answers.
Provided image
Question 1: A 16-year-old girl has had symptoms meeting MDD criteria for 6 weeks. PHQ-A score is 17. She has been seen by a psychologist for 8 sessions of CBT but has had minimal improvement. What is the next appropriate step in her management?
Answer: She is moderately severe (PHQ-A 17) and has not responded to CBT alone. The next step is to add fluoxetine (start 10 mg/day, titrate to 20–40 mg). This follows the TADS trial evidence that combination CBT + fluoxetine is superior to either alone for moderate-severe adolescent depression. Ensure weekly monitoring for the first 4 weeks for activating side effects and for any increase in suicidal ideation (FDA black-box warning).
Question 2: According to DSM-5, how many somatic symptoms must be present for a diagnosis of GAD in a 12-year-old child (compared to an adult)?
Answer: In children, only 1 somatic symptom is required (compared to ≥3 in adults). The DSM-5 notes this child-specific modification because younger children typically report fewer somatic symptoms than adults.
Question 3: Name two features in a suicide risk assessment that would indicate HIGH risk requiring emergency psychiatric referral.
Answer: Any two from: (a) specific plan with access to lethal means; (b) previous suicide attempt; (c) recent attempt within 3 months; (d) active suicidal intent; (e) comorbid substance use; (f) hopelessness with stated intent to complete.
SELF-CHECK
Which of the following statements about fluoxetine for adolescent depression is CORRECT?
A. Fluoxetine is contraindicated in adolescents under 18 due to the FDA black-box warning
B. Fluoxetine combined with CBT is superior to either treatment alone for moderate-to-severe adolescent MDD, according to the TADS trial; the black-box warning requires weekly monitoring at treatment start for activating effects and suicidal ideation
C. Fluoxetine is second-line — sertraline is the first-choice antidepressant for adolescent MDD
D. The black-box warning means fluoxetine should never be used in adolescents — the risk of suicidal ideation from the medication outweighs all benefits
Reveal Answer
Answer: B. Fluoxetine combined with CBT is superior to either treatment alone for moderate-to-severe adolescent MDD, according to the TADS trial; the black-box warning requires weekly monitoring at treatment start for activating effects and suicidal ideation
The TADS (Treatment for Adolescents with Depression Study) trial demonstrated that fluoxetine combined with CBT was superior to either treatment alone for adolescent MDD, and fluoxetine alone was superior to placebo. Fluoxetine (20–40 mg/day) is the first-choice antidepressant for moderate-to-severe adolescent depression based on this and other paediatric evidence. The FDA black-box warning (2004) notes a small increased risk of suicidal ideation in the first weeks of antidepressant treatment in children and adolescents — NOT completed suicide. The warning requires increased monitoring (weekly visits for the first 4 weeks, then fortnightly), but does NOT prohibit fluoxetine use. The consensus of paediatric and psychiatric guidelines is that the benefits of treating moderate-to-severe depression with fluoxetine substantially outweigh the risk of untreated depression (including suicide). The warning requires vigilance, not avoidance.