Page 11 of 21
PE7.8 | Human Milk Bank — SDL Guide
Learning Objectives
- Explain the clinical rationale for human milk banks and the populations they serve
- Describe the complete processing chain of a human milk bank from donor screening to dispensing
- Specify the Holder pasteurisation parameters and explain their effect on milk components
- Identify India's policy framework for human milk banks and Lactation Management Centres
- Recognise the ethical and cultural considerations relevant to donor milk use in the Indian context
INSTRUCTIONS
When a mother cannot provide her own breast milk — because of extreme prematurity, critical illness, death, or temporary separation — her vulnerable infant faces a dilemma: formula feeding carries a substantially higher risk of necrotising enterocolitis (NEC), infection, and poor neurodevelopmental outcomes, particularly in preterm infants; yet the ideal alternative, donor human milk, requires a sophisticated collection, processing, and dispensing infrastructure. The human milk bank (HMB) is the clinical solution to this dilemma. India has moved decisively toward establishing HMBs in public hospitals under NHM guidelines, and the number of functional Lactation Management Centres (LMCs) is growing. As a paediatrician working in any NICU, district hospital, or community setting, you need to know how an HMB works, what pasteurisation does to milk, who can receive donor milk, and how to counsel donor families.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 — Infant Feeding (textbook)
- WHO/PAHO Guidelines for the Establishment and Operation of Human Milk Banks, 2013 (guideline)
- NHM/MoHFW India: Operational Guidelines for Lactation Management Centres, 2017 (guideline)
- BPNI (Breastfeeding Promotion Network of India) — HMB standards (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Baby Rohan is born at 28 weeks gestation, weighing 980 g, by emergency caesarean section for severe pre-eclampsia. His mother is in the ICU, critically ill and sedated, unable to express milk. The neonatologist tells the father: 'We will use donor milk from the milk bank to feed Rohan for now — it is the closest thing to his mother's own milk.' The father, confused and a little worried, asks: 'Doctor, whose milk is it? Is it safe? How is it tested? Could it pass on diseases?' How do you answer him — and what does the milk bank actually do to ensure the milk is safe?
WHY THIS MATTERS
Human milk banks occupy a unique position at the intersection of neonatology, public health, ethics, and milk science. For preterm and very low-birth-weight (VLBW) infants, mother's own milk is the first choice — but when it is unavailable, donor pasteurised human milk is the WHO-recommended alternative, superior to formula specifically because it preserves many of the bioactive components that protect against NEC. NEC — necrotising enterocolitis — is the most feared complication of prematurity; it carries a 20–30% mortality and causes long-term gastrointestinal morbidity. Cochrane meta-analysis shows that preterm infants fed donor human milk have significantly lower rates of NEC compared with those fed preterm formula. Understanding the HMB — how it works, what processing achieves, and how it is regulated in India — is clinically essential because you will encounter donor milk in any NICU, and because you may be asked to counsel donor families or to prescribe pasteurised donor milk.
RECALL
From the breastfeeding physiology module: breast milk contains secretory IgA, lactoferrin, lysozyme, and human milk oligosaccharides (HMOs) — bioactive components with antimicrobial and immune-modulatory functions. Colostrum is highest in these factors; mature milk maintains them at lower but significant levels. From biochemistry (BI): pasteurisation is a heat treatment that kills pathogenic microorganisms by controlled heating below the boiling point — named after Louis Pasteur. HTLV-1 (Human T-lymphotropic virus type 1) is a retrovirus transmissible via breastfeeding; screening donors for this (in addition to HIV, HBV, HCV) is essential. Hold these — pasteurisation is both the key benefit and the main limitation of donor milk.
Orientation: Why Human Milk Banks Exist
The fundamental premise of the human milk bank is that breast milk is a living biological fluid whose benefits — particularly for preterm and ill infants — cannot be replicated by formula, and that if a mother cannot provide her own milk, the closest available alternative is milk from a screened, healthy donor, made safe by pasteurisation. This premise is backed by compelling evidence specific to the preterm population. Preterm infants — born before 37 weeks, and especially those born before 32 weeks or weighing <1500 g (very low birth weight, VLBW) — have an immature gut epithelium with increased permeability, an underdeveloped mucosal immune system, and a microbiome that is easily disrupted by formula. Necrotising enterocolitis (NEC), the most serious gastrointestinal emergency of the NICU, occurs predominantly in preterm formula-fed infants: bowel wall invasion by gas-forming bacteria leads to pneumatosis intestinalis, perforation, peritonitis, and death in 20–30% of affected infants. Human milk — by virtue of its secretory IgA, HMOs acting as prebiotics, epidermal growth factor (EGF) promoting gut epithelial repair, and lactoferrin preventing microbial proliferation — substantially reduces this risk.
The clinical gap that HMBs fill is specific: in settings where prematurity is common and NICU capability exists, a meaningful proportion of preterm infants will have mothers who are (a) critically ill and unable to express milk, (b) deceased, (c) temporarily separated, (d) producing insufficient colostrum in the first 24–48 hours while supply is being established, or (e) taking medications contraindicated in breastfeeding. For all these scenarios, pasteurised donor human milk is the bridge — it provides the protective benefits of human milk during the most vulnerable window, until the mother's own milk supply is established or the clinical situation changes.
The World Health Organization and IAP clearly state the hierarchy: (1) mother's own fresh milk is first choice; (2) mother's own expressed and stored milk is second; (3) pasteurised donor human milk from a certified HMB is third; (4) formula is the last resort for preterm infants when human milk is unavailable.
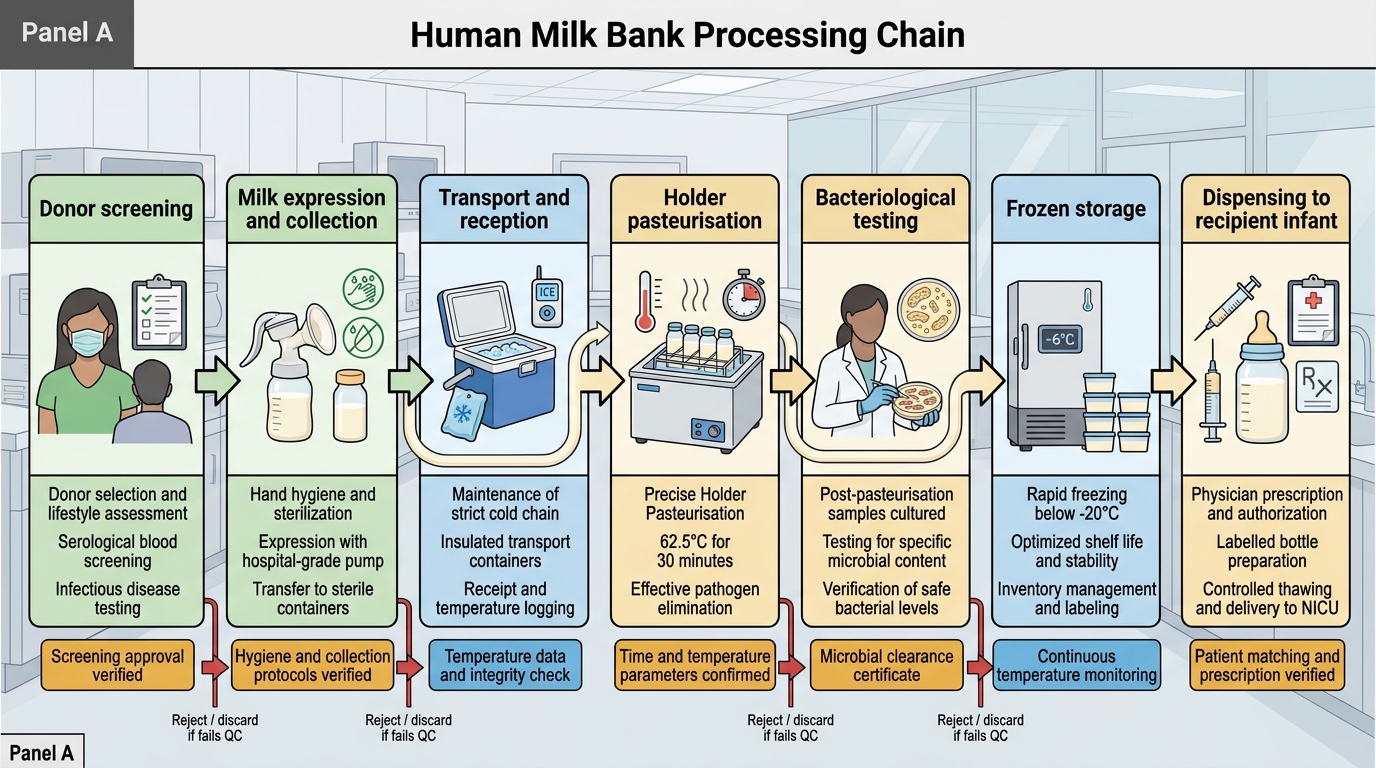
Human Milk Bank Processing Chain
Structure and Components of a Human Milk Bank
A functioning human milk bank is a specialised facility within a hospital (typically attached to a NICU or maternity unit) that manages the complete chain from donor recruitment to recipient dispensing. Each step is governed by standard operating procedures to ensure microbiological safety and nutritional integrity of the final product. The chain is essentially a quality-controlled supply pipeline: raw donated milk enters at one end, is screened for pathogens at the donor level, heat-treated to eliminate infectious agents, tested bacteriologically to confirm safety, stored under controlled conditions, and released by clinician prescription to specific recipients at the other end. The safety of the system depends on every link in this chain; a failure at any point — a screened-negative donor who seroconverts between rescreenings, an inadequate pasteurisation temperature, a bacteriological release without testing — could result in pathogen transmission to a vulnerable preterm infant. Understanding each step therefore means understanding both its purpose and its specific quality control parameter. The following describes the seven key steps of the HMB operating chain.
1. Donor recruitment and selection: Donors are healthy lactating mothers, typically those who have excess milk beyond their own infant's needs. Recruitment occurs through postnatal wards, community outreach, and media campaigns. Key eligibility criteria:
• Mother of a healthy infant (own infant's nutritional needs are fully met)
• No current medications contraindicated in breastfeeding (cytotoxic drugs, radioactive agents, certain antivirals)
• Non-smoker, no alcohol or illicit drug use
• Willing to provide informed consent and undergo serological screening
2. Donor screening (serological): All prospective donors must have negative serology for:
• HIV-1 and HIV-2 (ELISA + confirmatory test)
• HBsAg (Hepatitis B surface antigen)
• Anti-HCV (Hepatitis C antibody)
• VDRL/RPR (syphilis)
• HTLV-1/2 (Human T-lymphotropic virus — retrovirus transmissible via breastfeeding)
Rescreening is done every 3–6 months for continuing donors.
3. Milk collection: Donors are trained in hand expression or use of hospital-grade electric breast pumps. Strict hand hygiene is required. Milk is collected into sterile, graduated plastic containers (polypropylene or glass). Donated milk should be expressed within 2–4 hours of the last feed to maximise freshness. Home expression is common; the mother transports frozen or refrigerated milk to the HMB.
4. Pasteurisation — Holder method: The standard HMB pasteurisation method is the Holder pasteurisation technique: heating milk to 62.5°C for 30 minutes, followed by rapid cooling. The parameters (62.5°C, 30 minutes) are critical — too low or too brief fails to eliminate pathogens; too high or too long degrades heat-sensitive bioactive components. Holder pasteurisation eliminates HIV, HBV, HCV, CMV, HTLV-1, and all bacterial pathogens while preserving most macronutrients, HMOs, and a substantial fraction of bioactive proteins.
5. Bacteriological quality control: After pasteurisation, a sample of each batch is sent for bacterial culture. Pasteurised milk must have a total bacterial count of <10 colony-forming units (CFU) per mL to be cleared for dispensing. Pre-pasteurisation culture is also performed; milk with very high pre-pasteurisation counts (>105 CFU/mL) is discarded.
6. Storage: Cleared pasteurised milk is stored at 2–4°C (refrigerator) for up to 72 hours or at -20°C (freezer) for up to 3 months. Milk is labelled with donor ID, date of pasteurisation, and expiry date. Thawed pasteurised milk must be used within 24 hours and must not be re-frozen.
7. Dispensing: Donor milk is dispensed only on prescription by a clinician. Priority recipients are preterm infants <32 weeks or <1500 g (VLBW) whose mothers' own milk is unavailable. Recipients must have informed consent from parents/guardians. In many institutions, the milk is dispensed by volume per feed, calculated at 60–180 mL/kg/day depending on postnatal age and clinical status.
SELF-CHECK
The standard pasteurisation method used in human milk banks is Holder pasteurisation. What are the correct parameters?
A. 72°C for 15 seconds (HTST — high temperature short time)
B. 62.5°C for 30 minutes (Holder pasteurisation)
C. 100°C for 5 minutes (boiling)
D. 56°C for 60 minutes (low-temperature long-time)
Reveal Answer
Answer: B. 62.5°C for 30 minutes (Holder pasteurisation)
Holder pasteurisation uses 62.5°C for 30 minutes — the standard method for human milk banks worldwide and the method specified in WHO/PAHO guidelines and India's NHM LMC guidelines. These parameters were chosen to eliminate HIV, HBV, HCV, CMV, HTLV-1, and bacterial pathogens while preserving as much nutritional and bioactive content as possible. HTST (72°C/15 sec) is used for dairy milk and is less commonly used in HMBs as it degrades more heat-sensitive milk proteins. Boiling (100°C) destroys most bioactive factors. The 56°C/60 min protocol is not standard for HMBs.
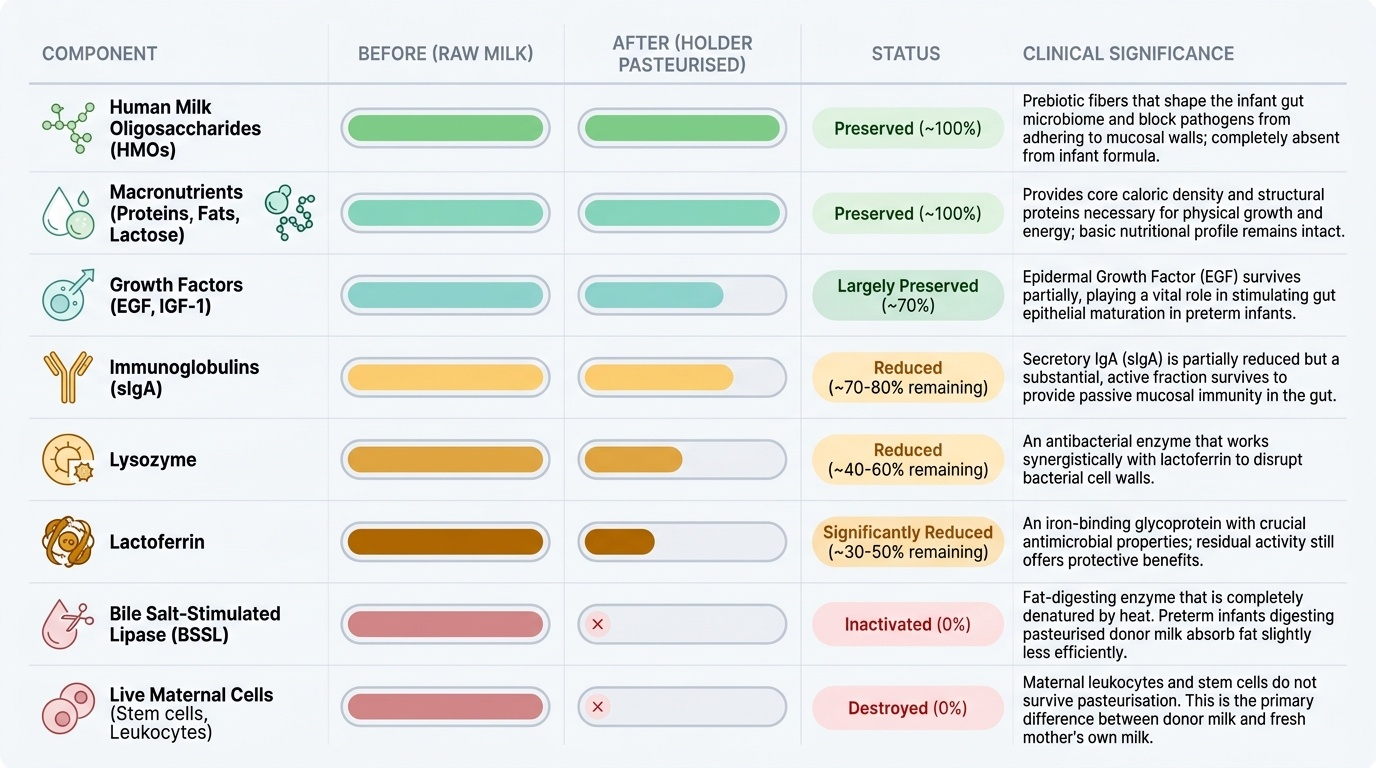
Effects of Pasteurisation on Milk Components
Holder pasteurisation is not a neutral process — it is a deliberate trade-off between eliminating pathogen risk and preserving bioactive milk components. Understanding what is preserved, what is reduced, and what is destroyed is clinically important because it explains both the advantages of donor milk (over formula) and its limitations (compared with fresh mother's own milk).
Provided image
The trade-off can be summarised in four categories:
Largely preserved: Most macronutrients — protein, fat, carbohydrate — are not substantially altered by Holder pasteurisation at the macronutrient level; total protein concentration, fat globule structure, and lactose are preserved. Human milk oligosaccharides (HMOs) — the prebiotic oligosaccharides — are heat-stable and survive Holder pasteurisation almost entirely intact; this is a critical advantage because HMOs are absent from formula and their preservation means donor milk retains its microbiome-shaping and pathogen-adhesion-blocking functions. Growth factors — EGF, IGF-1 — survive partially; EGF, important for gut epithelial maturation in preterm infants, is approximately 70% preserved.
Significantly reduced (but not eliminated): Secretory IgA (sIgA) — approximately 20–30% reduction with Holder pasteurisation; a substantial fraction survives and continues to provide mucosal protection. Lactoferrin — more heat-sensitive; approximately 50–70% is denatured, but residual activity remains. Lysozyme — similarly reduced by about 40–60%. The clinical implication is that pasteurised donor milk retains immunological activity, though at lower levels than fresh milk.
Largely or completely destroyed: Live cells — all live leucocytes (macrophages, lymphocytes, neutrophils) are killed by pasteurisation; this is one of the significant immunological losses. Bile-salt-stimulated lipase (BSSL) — the lipase that initiates fat digestion in the duodenum — is almost entirely inactivated by heat; this reduces fat absorption efficiency in preterm infants on donor milk compared with fresh mother's milk. Cytokines (e.g. IL-6, TNF-α) are largely destroyed. CMV — cytomegalovirus, which can be transmitted via fresh breast milk to preterm infants causing serious infection — is reliably eliminated by Holder pasteurisation; this is a major safety benefit for immunocompromised preterm recipients.
The net clinical conclusion: pasteurised donor human milk is substantially superior to formula for preterm infants because it preserves HMOs, growth factors, and residual immune proteins; it is inferior to fresh mother's own milk because live cells, full BSSL activity, and native IgA concentration are reduced. This hierarchy (mother's own > pasteurised donor > formula) is reflected in every clinical guideline.
| Component | Effect of Holder pasteurisation |
|---|---|
| Macronutrients (protein, fat, lactose) | Largely preserved |
| HMOs (oligosaccharides) | Largely preserved (heat-stable) |
| EGF, IGF-1 (growth factors) | Partially preserved (~70%) |
| Secretory IgA | Reduced ~20–30% |
| Lactoferrin | Reduced ~50–70% |
| Lysozyme | Reduced ~40–60% |
| Live leucocytes | Destroyed |
| Bile-salt-stimulated lipase | Largely destroyed |
| CMV, HIV, HTLV-1 | Eliminated |
| Bacteria | Eliminated |
CLINICAL PEARL
CMV and preterm infants — a reason pasteurisation matters beyond HIV: Fresh breast milk from a CMV-seropositive mother (approximately 60–70% of Indian women of reproductive age) can transmit CMV to a preterm infant. In a term infant with a mature immune system, postnatal CMV infection is usually asymptomatic. In a VLBW preterm infant, postnatal CMV infection can cause sepsis-like illness, hepatitis, thrombocytopenia, and neurodevelopmental sequelae. Holder pasteurisation reliably eliminates CMV from donor milk. This is one of the reasons why, for VLBW infants <28 weeks, even a seropositive mother's own expressed milk may be pasteurised at some centres before use — a practice called short-term pasteurisation or 'flash' heating. This nuance distinguishes the VLBW NICU context from the full-term healthy infant context where fresh milk is unambiguously superior.