Page 13 of 25
PE10.6 | Adolescent Nutrition Problems — SDL Guide (Part 2)
Overweight, Obesity, and Metabolic Syndrome in Adolescents
Adolescent obesity is the fastest-growing nutritional problem in urban India. The National Family Health Survey and multiple school-based studies document that the prevalence of overweight/obesity among urban adolescents has risen from approximately 5-7% in 2000 to over 14-20% in major metropolitan cities by 2020. This epidemiological transition reflects rapid dietary shifts — increased consumption of ultra-processed foods (high sugar, high saturated fat, high sodium, low fibre), sugar-sweetened beverages, and fast food — combined with dramatically reduced physical activity (increased screen time, motorised transport, decreased outdoor play).
Assessment of adiposity in adolescents requires BMI-for-age z-scores (not adult BMI cut-offs), because lean mass and fat mass change substantially through puberty. The WHO 2007 Growth Reference for adolescents uses: BMI-for-age ≥1 SD as overweight and ≥2 SD as obese. These correspond approximately to the 85th and 95th BMI percentiles. The IAP also recommends the IAP 2015 BMI-for-age charts for Indian adolescents.
Metabolic syndrome in adolescents — defined as central obesity plus ≥2 of: hypertriglyceridaemia (≥150 mg/dL), low HDL cholesterol (<40 mg/dL boys, <50 mg/dL girls), hypertension (≥130/85 mmHg for adolescents), or impaired fasting glucose (≥100 mg/dL) — is now being identified in Indian adolescents as young as 12-13 years. Insulin resistance is the central metabolic driver: excess visceral adipose tissue secretes inflammatory adipokines (TNF-α, interleukins), suppresses adiponectin, and impairs insulin signalling across multiple tissues.
The long-term consequences of adolescent obesity are not remote: type-2 diabetes is now being diagnosed in Indian teenagers; adolescent-onset hypertension tracks into adult hypertension in 50-70% of cases; non-alcoholic fatty liver disease (NAFLD) is increasingly detected in obese adolescents. Adolescent obesity also impairs respiratory function (obesity hypoventilation, obstructive sleep apnoea), musculoskeletal health (slipped capital femoral epiphysis, tibia vara/Blount's disease), and psychological wellbeing (stigma, depression, reduced self-esteem).
Management involves lifestyle intervention as first-line: dietary modification (reduce energy-dense/nutrient-poor foods, increase fibre, increase meal frequency), increased physical activity (60 minutes of moderate-vigorous activity per day — WHO recommendation for adolescents), and reduction of sedentary screen time to <2 hours/day (WHO). Pharmacological intervention (metformin, orlistat) is reserved for severe obesity with metabolic complications; bariatric surgery in adolescents is exceptional and outside routine practice.
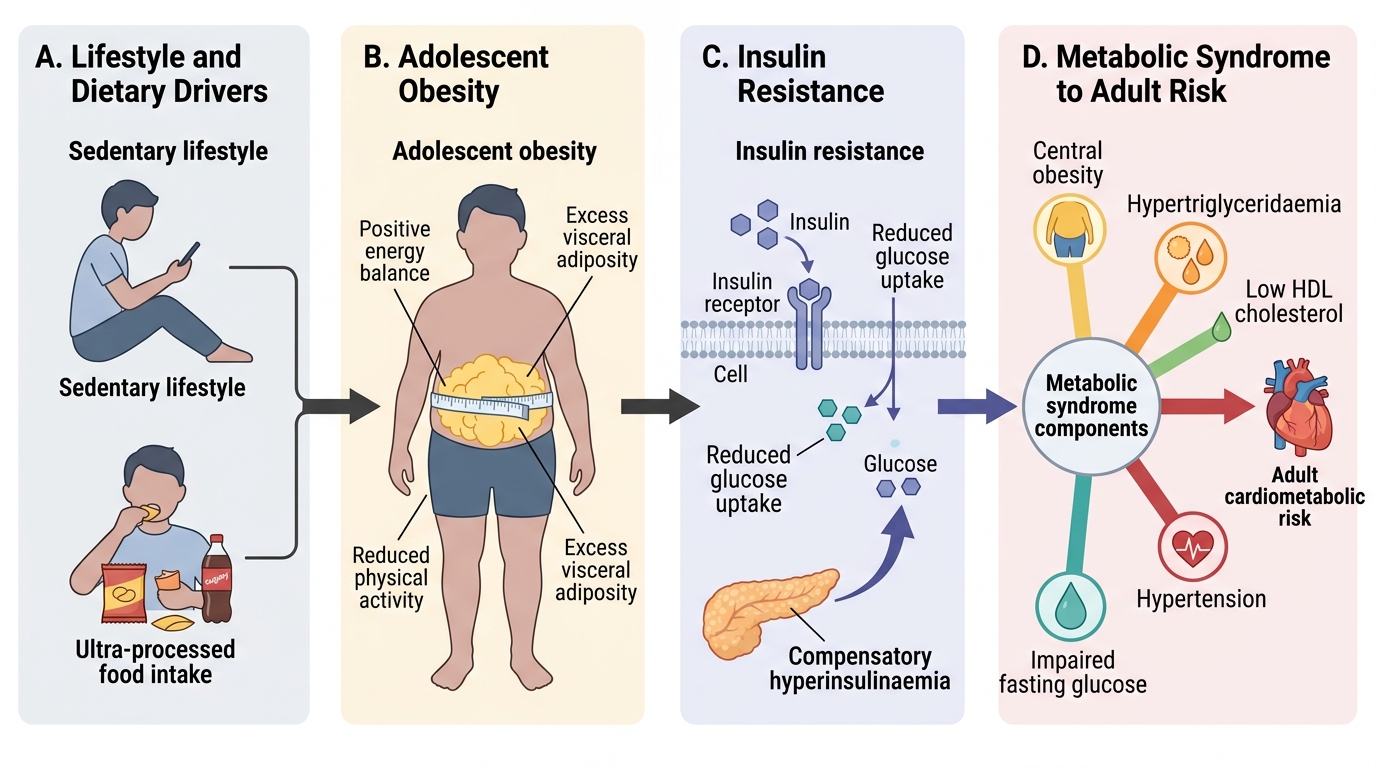
Pathway from Adolescent Obesity to Cardiometabolic Risk
CLINICAL PEARL
The single most cost-effective, evidence-based intervention for adolescent nutrition in India is the WIFS programme — yet its effectiveness depends entirely on compliance. The most common barriers to WIFS compliance are: (1) gastrointestinal side effects (nausea, dark stools) — advise taking the tablet after a meal, not on an empty stomach; (2) misconception that the tablet causes weight gain or darkens the skin — both false, and explicitly addressed in the WIFS counselling module; (3) stigma of being singled out for supplementation — school-based programmes mitigate this by supplementing all students simultaneously. When counselling adolescent girls, explicitly address these three concerns before prescribing — compliance is the rate-limiting step.
Eating Disorders: Anorexia Nervosa and Bulimia Nervosa
Eating disorders are psychiatric-nutritional conditions that occur predominantly in adolescents and young adults, with a strong female predominance (female:male ratio approximately 10:1 for anorexia nervosa, 5:1 for bulimia). They are increasingly recognised in urban India, particularly in higher socioeconomic groups, driven by media-promoted ideals of thinness and the psychosocial pressures of adolescence. Both conditions represent significant medical emergencies that require multi-disciplinary management.
Anorexia nervosa is characterised by: (1) significantly low body weight for developmental stage (BMI <17.5 kg/m² in adults; in adolescents, failure to gain expected weight during growth is equivalent); (2) intense fear of gaining weight or becoming fat, despite being underweight; (3) disturbed body image — seeing oneself as fat when demonstrably thin (body dysmorphic perception). The medical consequences of anorexia nervosa are severe and reflect profound nutritional and endocrine derangements: amenorrhoea (in >90% of girls — hypothalamic suppression from energy deficit); bradycardia and hypotension; prolonged QTc interval (risk of fatal ventricular arrhythmia); osteoporosis (oestrogen deficiency + inadequate calcium); lanugo (fine downy body hair — thermoregulatory response to fat loss); hypokalaemia; and anaemia. Anorexia nervosa has the highest mortality rate of any psychiatric disorder — approximately 5-10% of diagnosed cases die, primarily from cardiac complications or suicide.
Bulimia nervosa is characterised by recurrent episodes of binge eating (consuming large amounts of food in a short time with loss of control) followed by compensatory behaviours to prevent weight gain: self-induced vomiting, laxative abuse, excessive exercise, or fasting. Unlike anorexia nervosa, weight may be normal or elevated. Medical complications are predominantly electrolyte-driven: hypokalaemia from vomiting/laxatives → cardiac arrhythmias; dental erosion from gastric acid exposure to enamel; parotid gland enlargement (sialadenosis from repeated vomiting stimulation); oesophageal tears (Mallory-Weiss syndrome from forceful retching); calluses on the dorsum of the dominant hand (Russell's sign from induced vomiting).
Management of eating disorders is multidisciplinary: nutritional rehabilitation (structured meal plans with gradual caloric increase), psychotherapy (cognitive-behavioural therapy — CBT — is evidence-based for bulimia), family-based therapy (Maudsley approach) for adolescent anorexia, and medical monitoring of electrolytes and cardiac function. Inpatient admission is required when: BMI <14 kg/m², haemodynamic instability, severe electrolyte disturbance, or suicide risk.
Clinical and Applied Significance: Screening and Counselling in Practice
Practical nutritional screening of adolescents in clinical settings requires a systematic but time-efficient approach that can be executed in a routine consultation. The clinician should integrate nutritional screening into every adolescent visit — not only dedicated nutrition clinics. The key principle is that nutritional problems in adolescents are frequently asymptomatic or masked by adaptation; they are detected only by systematic screening, not by waiting for a chief complaint. Iron-deficiency anaemia, for example, is commonly compensated physiologically until haemoglobin falls below 9-10 g/dL — the adolescent may deny fatigue and appear functional while carrying a significant deficit. Obesity-related metabolic syndrome may be entirely asymptomatic in its early stages. Eating disorders are actively concealed. Without a proactive screening protocol applied to every adolescent encounter, these conditions are missed until they are advanced and harder to reverse. The framework below converts this clinical principle into a practical three-component screen that takes under 10 minutes to complete.
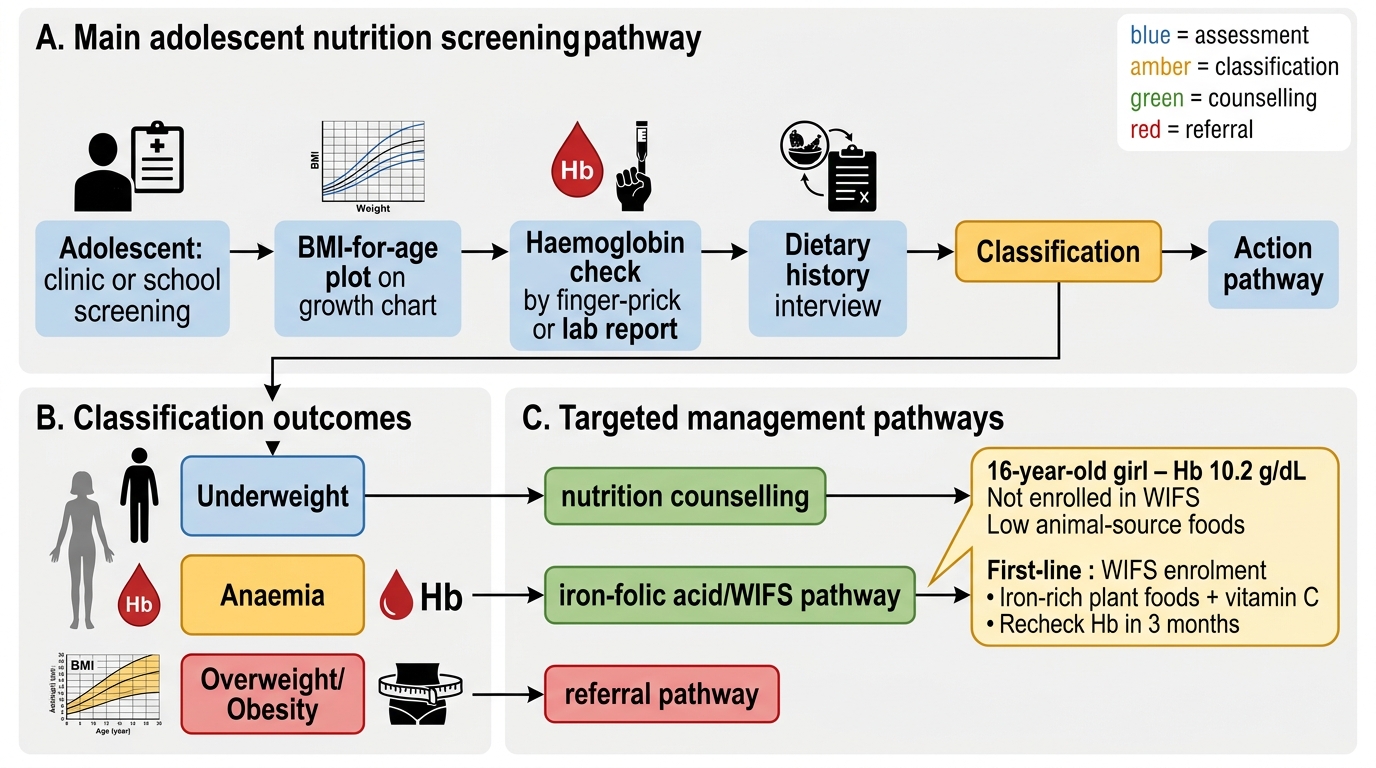
A minimum screening protocol for adolescent nutritional assessment in clinical practice includes three components:
1. Anthropometric screen: plot weight, height, and BMI-for-age on WHO/IAP 2015 growth charts; identify underweight (BMI < −2 SD), overweight (BMI ≥ +1 SD), or obesity (BMI ≥ +2 SD).
2. Haemoglobin check: a point-of-care Hb measurement detects anaemia (threshold <12 g/dL in girls, <13 g/dL in older adolescent boys); if Hb is low, proceed to full blood count and iron studies.
3. Dietary history: a brief 5-question dietary screen covers: frequency of dairy consumption (calcium), frequency of green leafy vegetables (iron/folate), frequency of ultra-processed food/sugary beverages (obesity risk), breastfeeding/infant feeding history (if in post-pubertal girl — pre-conception folate awareness), and any episodes of food restriction or purging behaviour (eating disorder screen).
Counselling content should be tailored to the problem identified:
• For anaemia: WIFS enrolment (if not already enrolled), dietary advice on iron-rich foods (dates, green leafy vegetables, dal, eggs, fortified cereals), vitamin C with iron sources, avoiding tea/coffee with meals.
• For calcium/vitamin D deficiency: increase dairy (or dairy alternatives), supervised 15-30 minutes of outdoor sun exposure daily, consider IAP-recommended supplementation (vitamin D 600 IU/day for adolescents if insufficient sun exposure).
• For overweight/obesity: motivational interviewing (not shaming); reduce sugar-sweetened beverages; substitute ultra-processed snacks with whole foods; increase physical activity gradually; involve family as the primary dietary influencer.
• For eating disorder suspicion: validate concerns without confrontation, refer to adolescent psychiatry and dietetics, assess for medical emergency indicators (pulse, BP, electrolytes).
Adolescent Nutritional Screening in Clinical Practice
SELF-CHECK
A 16-year-old girl is found to have haemoglobin of 10.2 g/dL on school screening. She is not enrolled in WIFS and says she rarely eats meat or eggs. Which combination of interventions is MOST appropriate as first-line?
A. Daily parenteral iron infusion and restrict all plant-based foods
B. Enrol in WIFS (100 mg elemental iron + 500 μg folic acid weekly), counsel on dietary iron-rich plant foods + vitamin C pairing, and recheck Hb in 3 months
C. Recommend only dietary changes with no supplementation as her anaemia is mild
D. Prescribe daily oral iron 200 mg and monthly haemoglobin checks
Reveal Answer
Answer: B. Enrol in WIFS (100 mg elemental iron + 500 μg folic acid weekly), counsel on dietary iron-rich plant foods + vitamin C pairing, and recheck Hb in 3 months
For a 16-year-old girl with mild-to-moderate anaemia (Hb 10.2 g/dL = moderate, between 7-12 g/dL) and no dietary iron source, the combination of WIFS enrolment (the national programme) with targeted dietary counselling is the evidence-based first-line approach. WIFS provides 100 mg elemental iron + 500 μg folic acid weekly — the standard NHM dose. Dietary counselling should include iron-rich plant foods (dates, leafy vegetables, fortified cereals) paired with vitamin C to enhance non-haem iron absorption. Daily 200 mg iron in option D exceeds the WIFS protocol dose and is the treatment dose for established anaemia in pregnancy — not the supplementation dose for adolescents. Dietary change alone without supplementation is insufficient for established moderate anaemia. Parenteral iron is not indicated for mild-moderate uncomplicated iron-deficiency anaemia.
Self-Assessment
Before completing this module, confirm your mastery of the most clinically important facts. These are the anchor points that appear in every undergraduate examination covering adolescent nutrition and are tested directly in OSCE stations, short-answer questions, and clinical case discussions. Adolescent nutrition spans a wide problem spectrum — from the most common single nutritional disorder in India (iron-deficiency anaemia in girls) to the most lethal psychiatric disorder in medicine (anorexia nervosa) — and the clinician must have fluency at both ends. Can you state the WHO anaemia threshold for adolescent girls (12-18 years) without hesitation? Can you describe the WIFS programme — the dose, frequency, and route — and explain why weekly dosing is used rather than daily? Can you identify the three components of a minimum adolescent nutritional screening protocol? Can you name two medical complications each of anorexia nervosa and bulimia nervosa that require emergency management? Can you use BMI-for-age (rather than adult BMI cut-offs) correctly to classify an adolescent's adiposity?
Key anchors:
• WIFS dose: 100 mg elemental iron + 500 μg folic acid, once weekly (school-based, supervised)
• Anaemia threshold (adolescent girls): Hb <12 g/dL; (boys ≥14 yr): Hb <13 g/dL
• Calcium requirement adolescent (9-18 yr): 1300 mg/day
• Iron requirement adolescent girls (menstruating): 21 mg/day (ICMR 2020)
• Obesity cut-off adolescents: BMI-for-age ≥ +2 SD (WHO 2007 reference)
• Anorexia nervosa warning: amenorrhoea + bradycardia + prolonged QTc — cardiac emergency
• NAFLD, metabolic syndrome, type-2 diabetes in adolescents — consequences of obesity