Page 18 of 25
PE11.3-4 | Childhood Obesity Assessment — SDL Guide
Learning Objectives
- Elicit a structured history from an obese child including physical activity assessment, 24-hour dietary recall, and growth charting
- Calculate BMI and plot it on an IAP age- and sex-specific growth chart to classify weight status
- Measure waist circumference and hip circumference and calculate the waist-hip ratio
- Identify and describe external markers of obesity-related comorbidity including acanthosis nigricans, striae distensae, and pseudogynaecomastia
- Synthesise history and examination findings into a structured clinical assessment with appropriate documentation
INSTRUCTIONS
Knowing that childhood obesity exists and understanding its pathophysiology are necessary but not sufficient clinical skills — you must also be able to systematically assess an obese child in front of you. This module builds the practical competency for that assessment: how to take a focused history that captures dietary intake, physical activity, and growth trajectory; how to perform and document the key anthropometric measurements; and how to recognise the external physical signs that indicate metabolic and hormonal complications. These are the skills tested in OSCE stations and required in every paediatric outpatient encounter with an overweight or obese child.
References
- Ghai Essential Pediatrics, 9th ed, Ch 7 (Nutrition & Growth Assessment) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 60 (Obesity Assessment) (textbook)
- IAP Guidelines on Childhood Obesity, 2015 (guideline)
- WHO Growth Reference Charts, 2007 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are at an OSCE station. A 12-year-old boy weighing 68 kg and 150 cm tall is seated in front of you. The instruction card reads: 'Assess this child for obesity. Take a relevant history and perform the appropriate examination. Document your findings and classify the child's weight status.' The examiner is watching. Where do you start? What measurements must you take, and in what sequence? What specific questions must you ask about diet and activity? What do you look for on examination beyond the obvious? This module answers every one of those questions.
WHY THIS MATTERS
A structured assessment of the obese child is the foundation for every subsequent clinical decision — the choice of investigations, the counselling conversation with parents, the referral pathway, and the monitoring plan. An unstructured approach (simply noting 'overweight' in the notes) is clinically useless: it misses the dietary and activity drivers that are the targets of intervention, it fails to document the anthropometric baseline needed for monitoring progress, and it will not detect the early comorbidity markers (acanthosis nigricans, elevated blood pressure, striae) that indicate urgent metabolic screening. As a final-year student you are expected to be able to perform this assessment independently and document it in a format that is useful to any clinician who subsequently sees the child.
RECALL
Recall from earlier modules: (1) the BMI formula (weight in kg divided by height in metres squared) and the IAP/WHO cut-offs for overweight (≥85th percentile) and obese (≥95th percentile) in children; (2) the physiological basis of insulin resistance and why acanthosis nigricans signals it at the skin; (3) the Holliday-Segar formula for maintenance fluids — relevant because you may be asked to estimate caloric needs in the same clinical context; (4) basic nutrition assessment tools from your Community Medicine posting: 24-hour dietary recall, food frequency questionnaire, and dietary diversity score. These prior-knowledge anchors make the new procedural content easier to integrate.
Clinical Indication and Relevance of Obesity Assessment
A systematic, structured assessment of an obese child is clinically indicated whenever a child's BMI-for-age is at or above the 85th percentile on the IAP/WHO growth chart, when a parent or teacher expresses concern about a child's weight, or when the child presents with symptoms potentially attributable to obesity-related comorbidities — such as snoring, daytime sleepiness, knee pain, irregular periods in an adolescent girl, or fatigue on exertion. The assessment is also indicated as a surveillance procedure during well-child visits in children with high-risk family backgrounds (two obese parents, parental type 2 diabetes, or family history of early cardiovascular disease).
The purpose of a structured assessment is fourfold. First, it classifies severity — distinguishing between overweight, obese, and severely obese using validated anthropometric criteria, which determines management intensity. Second, it identifies the aetiology — distinguishing primary exogenous obesity from secondary causes (endocrine, genetic) through the history and clinical examination. Third, it detects comorbidities — the metabolic, cardiovascular, and orthopaedic complications that may already be present at the time of first presentation. Fourth, it documents a baseline — the anthropometric and clinical data against which future progress will be measured, making the assessment the first step in a longitudinal monitoring plan rather than a one-time event.
A structured assessment that is poorly performed — using the wrong equipment, measuring at the wrong anatomical landmarks, or failing to ask the right dietary history questions — produces data that is useless for these four purposes and may actively mislead clinical decision-making. The skill therefore depends on both procedural precision and systematic completeness.
Anatomical Landmarks for Waist and Hip Circumference Measurement
Anatomy and Governing Principles of Anthropometric Measurement
Accurate anthropometric measurement of an obese child requires knowledge of precise anatomical landmarks and adherence to standardised technique. Small errors in landmark identification or positioning introduce systematic biases that make serial comparisons meaningless and cross-sectional comparisons with reference data invalid.
Weight measurement: The child should be weighed in light clothing (no shoes, no heavy garments) on a calibrated digital scale. The scale must be placed on a hard, flat surface and zeroed before each measurement. Record weight to the nearest 0.1 kg.
Height measurement: Use a wall-mounted stadiometer (not a portable measuring tape). The child stands barefoot with heels, buttocks, shoulder blades, and the back of the head touching the vertical surface (Frankfurt plane — the Frankfort horizontal plane, defined by the lower border of the orbit and the upper border of the external auditory meatus, should be parallel to the floor). The child inhales, stands maximally tall, and the headpiece is brought firmly onto the crown. Record height to the nearest 0.1 cm. The combination of weight and height allows BMI calculation: weight (kg) ÷ height (m)², which is then plotted on the IAP 2015 age- and sex-specific chart to determine the percentile.
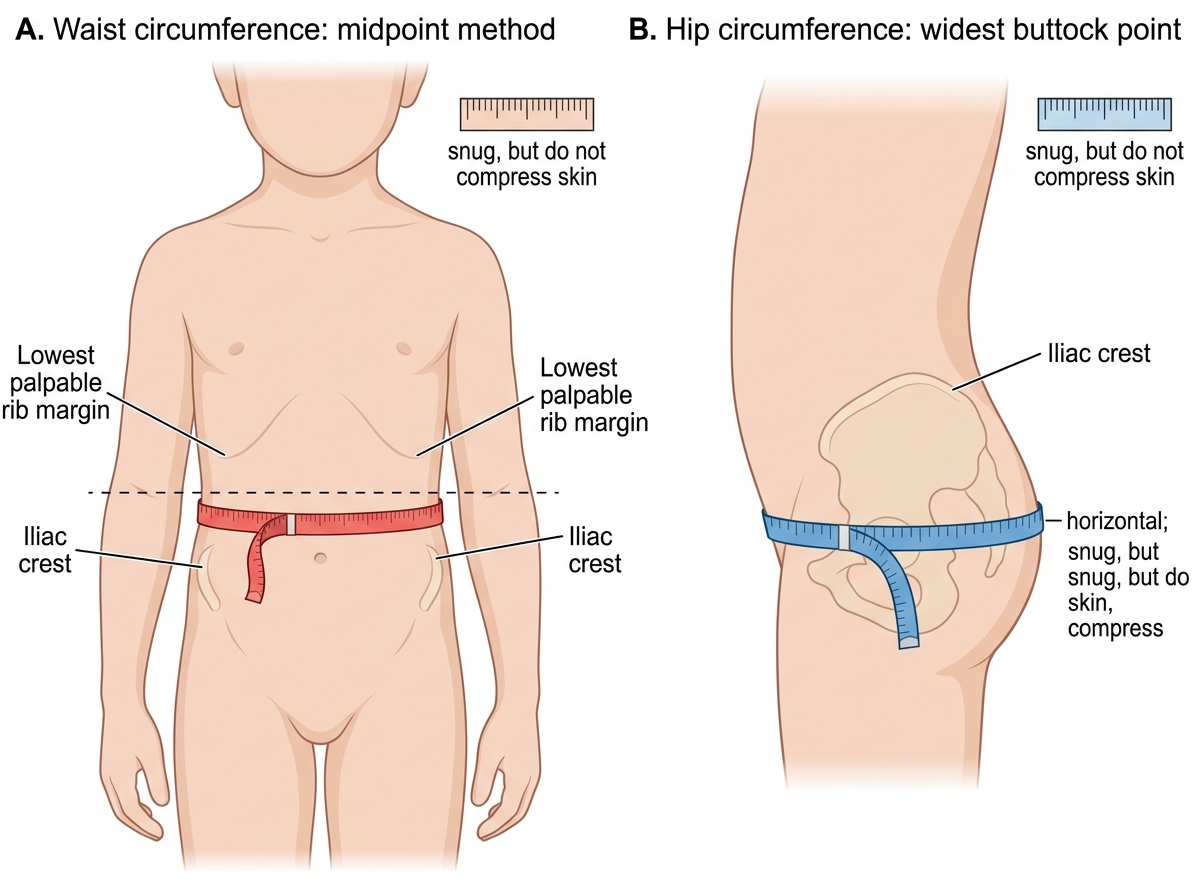
Waist circumference is measured at the midpoint between the inferior border of the lowest (12th) rib and the superior border of the iliac crest, in the mid-axillary line. The child stands relaxed, breathes out gently (not sucking in), and the non-stretchable tape is applied horizontally, making contact with the skin but not compressing soft tissue. Record to the nearest 0.1 cm. Waist circumference >90th percentile for age and sex indicates abdominal obesity with significant visceral fat.
Hip circumference is measured at the widest point of the buttocks (approximately at the level of the greater trochanters), with the tape horizontal and the child standing with feet together. The waist-hip ratio (WHR) = waist circumference ÷ hip circumference. In adults, WHR >0.85 (women) or >0.90 (men) indicates abdominal obesity; in children, absolute WHR cut-offs are less well validated — the waist-to-height ratio >0.5 is a more robust paediatric cardiometabolic risk indicator.
Blood pressure must be measured with an age-appropriate cuff (cuff bladder width = 40% of the arm circumference at the midpoint; bladder length = 80–100% of arm circumference). Using an adult cuff on a child's arm gives a falsely low reading; a cuff that is too small gives a falsely high reading. The child must be seated quietly for 5 minutes before measurement.
SELF-CHECK
When measuring waist circumference in a child for obesity assessment, where is the correct anatomical landmark for placing the measuring tape?
A. At the level of the umbilicus
B. At the midpoint between the lowest rib and the iliac crest in the mid-axillary line
C. At the narrowest point of the abdomen as seen from the front
D. At the level of the anterior superior iliac spine
Reveal Answer
Answer: B. At the midpoint between the lowest rib and the iliac crest in the mid-axillary line
The WHO/IAP standard for waist circumference measurement in children is the midpoint between the inferior border of the lowest (12th) rib and the superior border of the iliac crest, measured in the mid-axillary line. Measuring at the umbilicus overestimates waist circumference in obese children (the umbilicus migrates inferiorly with central adiposity). Measuring at the narrowest point introduces observer-dependent variability. Measuring at the anterior superior iliac spine is incorrect and would underestimate the true waist circumference.
History-Taking: Physical Activity, Dietary Recall, and Charting
A focused history in an obese child serves to establish the probable aetiology (primary vs secondary), identify the modifiable behavioural drivers that will be the targets of intervention, and document the temporal trajectory of weight gain. The history is most productive when taken from both the child and the parent together, then supplemented by separate questions to the child to obtain answers the child may not give freely in front of parents — particularly regarding emotional eating, bullying, sedentary habits, or activity preferences. Unlike many clinical histories that can be compressed without information loss, the obesity history has five distinct domains that each yield operationally important data: the weight-gain trajectory, the dietary intake, the physical activity and screen-time pattern, systems review for comorbidities, and the family background. Skipping any domain produces an incomplete assessment that cannot guide counselling. Structure your history in this order, giving appropriate time to the dietary and activity components — these are the sections students most commonly rush through.
History of weight gain:
- When was excess weight first noticed? Was onset gradual (primary) or rapid (suggests secondary cause)?
- Birth weight (large-for-gestational-age infants have increased obesity risk)
- Feeding history: breastfed vs formula-fed; age of complementary food introduction
- Any previous attempts at dietary modification or weight-loss programmes?
Dietary history — the 24-hour dietary recall:
The 24-hour dietary recall is the most practical dietary assessment tool for clinical use. Ask the child/parent to describe EVERY food and drink item consumed in the previous 24 hours, in the order it was consumed, from waking to sleeping. Use open-ended prompts: 'What was the first thing you ate or drank after waking up?' 'What did you have next?' 'Was there anything between meals?' Crucially, probe for portion sizes using household measures (cups, tablespoons, standard serving size). Key items to specifically ask about in Indian children: frequency and quantity of sugar-sweetened beverages (soft drinks, packaged juices, milkshakes); fried and processed snacks (chips, biscuits, namkeen); oil used in cooking; rice and roti quantity; frequency of fast food and restaurant meals.
| Meal | Time | Food Item | Portion Size | Estimated kcal |
|---|---|---|---|---|
| Breakfast | 7 am | Poha with peanuts | 1 cup (200 g) | ~250 |
| Mid-morning | 10 am | Packaged biscuits | 3 (50 g) | ~220 |
| Lunch | 1 pm | 3 chapati + dal + sabzi + rice | full plate | ~600 |
| Snack | 4 pm | 1 glass cold drink (500 mL) | 1 bottle | ~200 |
| Dinner | 8 pm | Rice + chicken curry | large plate | ~700 |
| After dinner | 9 pm | Ice cream | 2 scoops | ~200 |
Physical activity assessment:
Ask about: (1) structured exercise — type, frequency, duration; (2) school-based physical education — frequency, whether the child participates; (3) active commuting — walking or cycling to school; (4) unstructured outdoor play — hours per day; (5) screen time — total hours per day including television, smartphone, tablet, computer games (ask separately, as children often under-report total screen time when asked about 'TV' alone). The WHO/IAP recommendation is ≥60 minutes of moderate-to-vigorous physical activity (MVPA) daily and screen time <2 hours/day for school-age children.
Growth charting:
Obtain previous growth records (vaccination card, school health records, previous clinic visits) and plot weight, height, and BMI at each time point on the IAP growth chart. This reveals the tempo of weight gain: a sudden inflection point (e.g. dramatic weight gain after a tonsillectomy, starting a new medication, or a family upheaval) suggests a specific precipitating event or secondary cause. A child who has been tracking at the 90th percentile since early childhood has a very different clinical picture from one who crossed from the 50th to the 95th percentile in 18 months.
Systems review for secondary causes and comorbidities:
- Constipation, cold intolerance, lethargy (hypothyroidism)
- Snoring, apnoeas, daytime sleepiness (OSA)
- Knee or hip pain (Blount's, SCFE)
- Irregular periods, acne, excess facial hair (PCOS)
- Headaches (intracranial hypertension, hypertension)
- Mood, school performance, social relationships (psychosocial impact)
Family history: obesity, type 2 diabetes, cardiovascular disease, dyslipidaemia, hypertension in parents or first-degree relatives.