Page 1 of 25
PE9.{1,3} | Normal Nutritional Needs — SDL Guide
Learning Objectives
- Describe the age-related nutritional requirements for energy, protein, fat, and carbohydrates in infants, children, and adolescents using ICMR/WHO reference values
- Identify the key micronutrients (iron, calcium, zinc, vitamins A, D, C, B12, iodine) and their recommended daily allowances across paediatric age groups
- Explain the caloric value of common Indian staple foods and apply this to simple meal-planning scenarios
- Outline the principles of breastfeeding and complementary feeding and their role in meeting infant nutritional needs
INSTRUCTIONS
Nutrition in the first two decades of life is not merely about preventing hunger — it is the biological foundation on which a child's entire physical and cognitive potential is built. Clinicians who understand age-specific requirements can recognise deviation early, counsel families accurately, and intervene before irreversible deficits occur. This module provides the reference framework for normal nutritional needs that underpins every topic from assessment to therapeutic diet planning.
References
- Ghai Essential Pediatrics, 9th ed, Ch 7 (Nutrition and Nutritional Disorders) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Section on Nutritional Requirements (textbook)
- ICMR-NIN Recommended Dietary Allowances for Indians, 2020 (guideline)
- WHO Child Growth Standards, 2006; WHO/UNICEF Breastfeeding Guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old boy is brought to the OPD with his anxious mother who says, 'I stopped breastfeeding at 5 months because I thought my milk was not enough, and now I give him only rice kanji twice a day.' On examination the child has visible wasting, irritability, and pallor. His weight is 6.2 kg — well below the 3rd centile. The child is not receiving adequate energy, protein, or iron for his age. Understanding what a 9-month-old actually needs each day is the first step towards recognising this failure early enough to matter.
WHY THIS MATTERS
Malnutrition remains one of the leading contributors to under-5 mortality in India. The NFHS-5 (2019-21) found that 35% of Indian children under 5 years were stunted, 19% were wasted, and 32% were underweight — figures that have barely halved over two decades. Behind each number is a failure to provide age-appropriate nutrition consistently across the first years of life. Equally important, over-nutrition among adolescents is driving a rising epidemic of childhood obesity and type-2 diabetes. As a final-year student, you will counsel parents, screen for nutritional disorders at every encounter, and prescribe dietary interventions. None of that is possible without fluency in what each age group requires — the reference quantities, the food sources, and the Indian dietary context.
RECALL
Before exploring paediatric requirements, recall from your biochemistry course: carbohydrates are the primary fuel for most tissues, providing 4 kcal/g; proteins yield 4 kcal/g and are the structural substrate for growth; fats provide 9 kcal/g and are essential for brain myelination, fat-soluble vitamin absorption, and cell membrane integrity. From physiology, recall that the small intestine absorbs iron by regulated transport (ferroportin) and that iron absorption is enhanced by vitamin C and inhibited by phytates — an important interaction in predominantly plant-based Indian diets. Vitamins A and D are fat-soluble (stored in liver; can accumulate toxically); vitamins B and C are water-soluble (not stored; daily replenishment needed). These biochemistry foundations will help you reason about deficiency consequences rather than merely memorising them.
Orientation: Why Nutrition Matters in Paediatrics
The paediatric period encompasses the most rapid phase of growth and brain development in the human lifespan. From birth to 2 years — often called the 'first 1000 days' (from conception) — brain synaptic density doubles, body weight quadruples, and height increases by approximately 50%. Every cell division during this phase requires an adequate supply of energy, amino acids, fatty acids, and micronutrients; a deficit during this critical window leads to permanent structural and functional consequences that cannot be fully reversed later.
Nutritional requirements are not uniform across childhood. They are determined by three intersecting factors: (1) the basal metabolic rate (BMR), which scales with body surface area and lean mass; (2) the growth velocity, which peaks in infancy and again in adolescence; and (3) physical activity level (PAL), which increases progressively from toddler through school age. Superimposed on these are disease states — fever, infection, and chronic illness each increase caloric demand further. Clinicians must therefore have age-specific reference values in mind, not a single 'paediatric' figure.
The term recommended dietary allowance (RDA) refers to the daily intake sufficient to meet the nutrient requirements of 97-98% of healthy individuals in a specific group. In India, the ICMR-NIN (National Institute of Nutrition) publishes Indian-specific RDAs that account for the predominantly plant-based diet, body size, and local food availability. The 2020 ICMR-NIN RDA update is the current national reference and supersedes the older 2010 values — clinicians should use the 2020 figures.
From a clinical standpoint, understanding normal requirements allows the practitioner to: (a) identify a dietary gap when taking a history; (b) prescribe a therapeutic diet that actually meets the deficit; and (c) counsel families in terms of locally available and affordable foods rather than imported supplements.
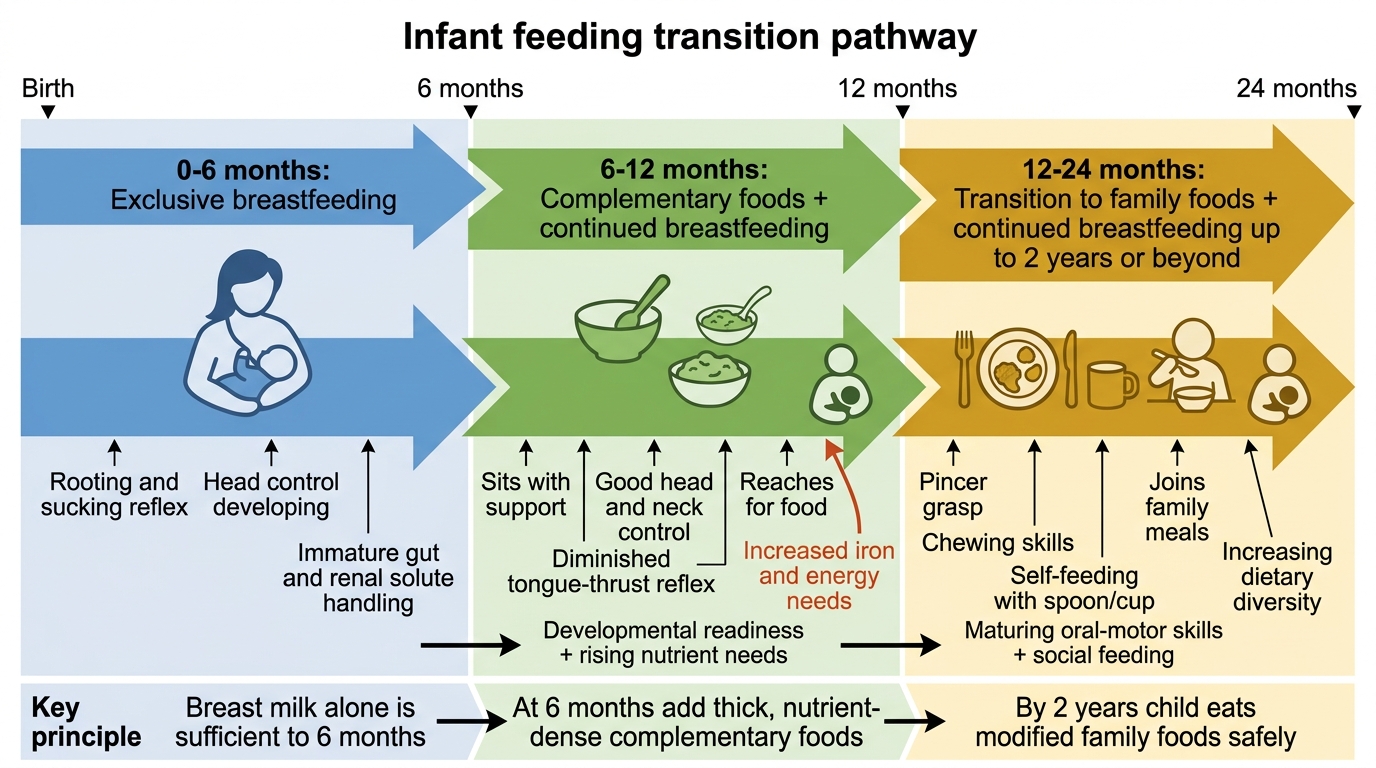
Infant Feeding Transitions from Birth to 2 Years
Age-Specific Energy and Macronutrient Requirements
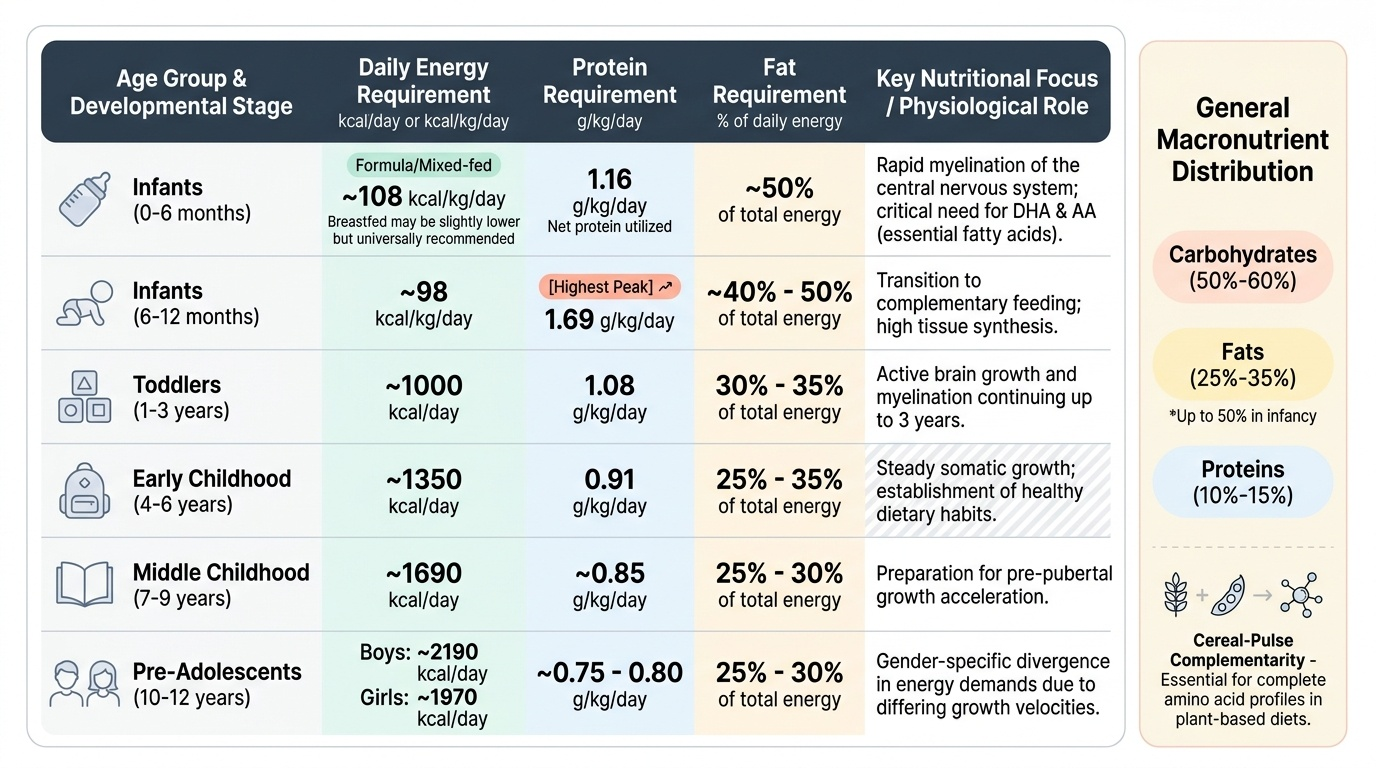
Energy requirements are highest per kilogram during early infancy and decline progressively as growth velocity falls. In the first 6 months of life, the WHO/FAO recommends approximately 108 kcal/kg/day for formula-fed or mixed-fed infants; exclusive breastfeeding provides somewhat lower energy but is universally endorsed because of non-caloric benefits. By 6-12 months, as growth velocity decreases slightly, the requirement falls to approximately 98 kcal/kg/day. The ICMR-NIN 2020 values for absolute daily energy requirements are: 1-3 years ≈ 1000 kcal/day; 4-6 years ≈ 1350 kcal/day; 7-9 years ≈ 1690 kcal/day; 10-12 years (boys) ≈ 2190 kcal/day; 10-12 years (girls) ≈ 1970 kcal/day. Adolescents (13-18 years) have the highest absolute requirements — boys up to 2640 kcal/day — driven by the pubertal growth spurt.
Provided image
Macronutrient distribution should follow these approximate proportions across childhood: carbohydrates 50-60% of total energy, fats 25-35% (with higher fat proportions for infants, where fat constitutes ~50% of breast-milk energy), and proteins 10-15%. These percentages are not rigid but provide a framework for diet assessment.
Protein requirements are highest per kilogram in infancy, reflecting rapid tissue synthesis. The ICMR-NIN 2020 recommends for breastfed infants 0-6 months ≈ 1.16 g/kg/day (net protein utilised); 6-12 months ≈ 1.69 g/kg/day; 1-3 years ≈ 1.08 g/kg/day; 4-6 years ≈ 0.91 g/kg/day; 13-15 years (boys) ≈ 0.73 g/kg/day. Protein quality matters as much as quantity: plant proteins (cereals, pulses) have lower digestibility and incomplete amino-acid profiles compared to animal proteins (milk, egg, meat). In India, most children depend on cereal-pulse complementarity — consuming rice or wheat with dal achieves a near-complete amino-acid profile by providing complementary limiting amino acids.
Dietary fat in infancy is indispensable for myelination of the central nervous system, which is most active from birth to 3 years. Docosahexaenoic acid (DHA) and arachidonic acid (AA) — long-chain polyunsaturated fatty acids — are specifically required for brain and retinal development. Breast milk is the best natural source; in formula-fed infants, these must be supplemented. After infancy, total fat intake can be reduced, but essential fatty acids (linoleic acid, alpha-linolenic acid) remain mandatory throughout childhood.
SELF-CHECK
A 2-year-old child weighing 12 kg is being assessed for dietary adequacy. According to ICMR-NIN 2020 recommendations, approximately how many kilocalories per day should this child receive?
A. 600-700 kcal/day
B. 1000-1050 kcal/day
C. 1350-1400 kcal/day
D. 1690-1750 kcal/day
Reveal Answer
Answer: B. 1000-1050 kcal/day
The ICMR-NIN 2020 RDA for children aged 1-3 years is approximately 1000 kcal/day. This reflects lower growth velocity compared to infancy but still accounts for high BMR relative to body weight. The 1350-1400 kcal/day range applies to 4-6 year olds, and 1690 kcal/day to 7-9 year olds. The 600-700 range is inadequate for any child in this age group and would represent significant under-nutrition.
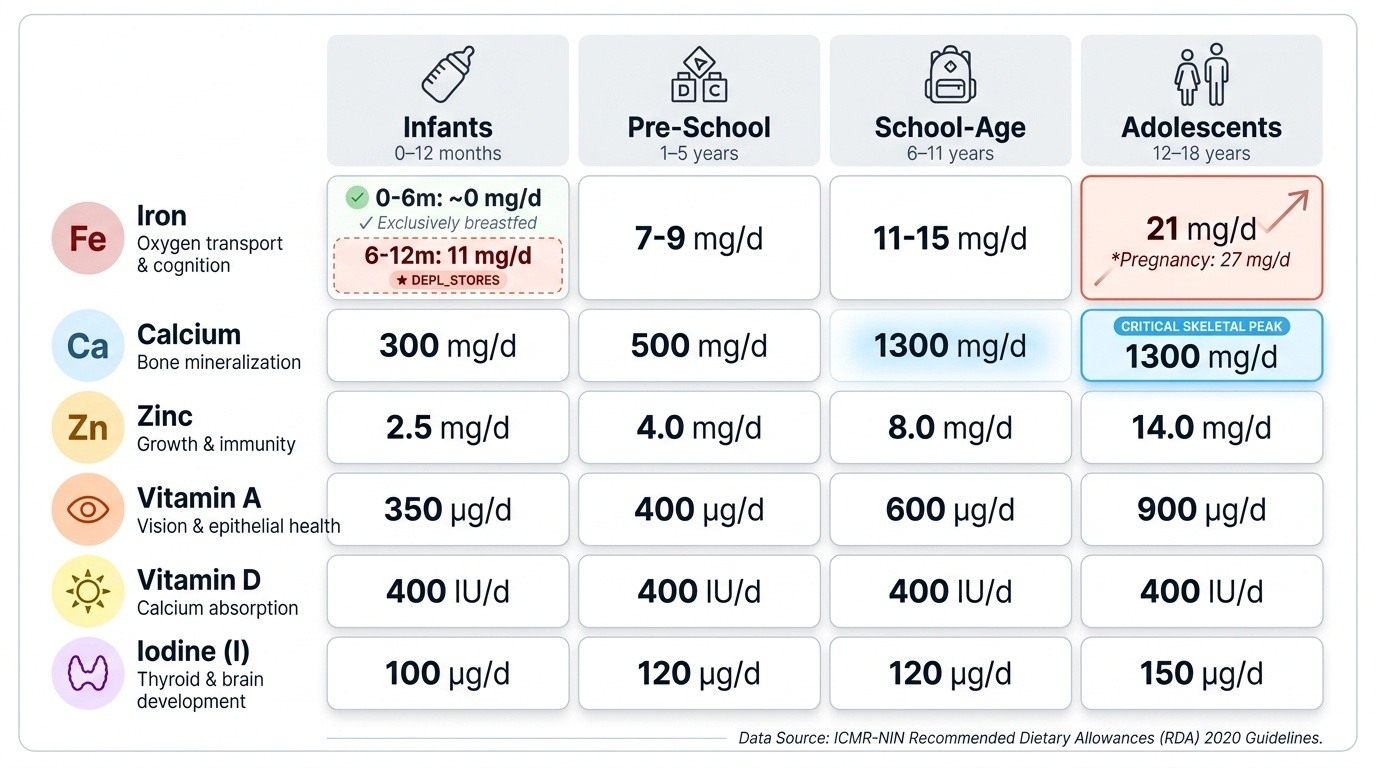
Micronutrient Requirements Across Age Groups
Micronutrients are required in small quantities but their absence causes specific, often severe, clinical syndromes. Unlike macronutrients, micronutrient requirements do not consistently decline per kilogram with age — some (iron, calcium) peak sharply at specific developmental stages driven by physiology rather than simply body size.
Provided image
Iron is the single most common micronutrient deficiency in Indian children. Requirement is paradoxically low in the first 6 months of life (approximately 0 mg/day in exclusively breastfed infants — breast milk iron has high bioavailability and fetal iron stores from in-utero transfer suffice); it rises sharply after 6 months to approximately 11 mg/day from 6-12 months, when stores are depleted and growth is rapid. Toddlers (1-3 years) require 7-9 mg/day. Pre-adolescent and adolescent girls have the highest requirement — 27 mg/day in pregnancy and 21 mg/day during adolescence (ICMR 2020) — due to menstrual losses superimposed on growth needs. Iron-deficiency anaemia is the commonest cause of anaemia in Indian children; its prevention requires timely introduction of iron-rich complementary foods and supplementation per IAP/NHM protocols (iron supplementation at 6 months in breastfed infants).
Calcium is the primary structural mineral in bone. Requirements peak during the adolescent growth spurt when skeletal mass accumulates rapidly: 1300 mg/day for 9-18 years (ICMR 2020). Dairy products are the most bioavailable source; Indian children who are lactose-intolerant or from dairy-limited households are at risk of suboptimal peak bone mass, with long-term consequences for osteoporosis in adulthood.
Zinc is required for over 100 enzyme systems and is particularly important for immune function, wound healing, and growth. Requirement is 3-4 mg/day in infancy, rising to 9-12 mg/day in adolescence. Zinc deficiency is associated with stunting, impaired immunity, and diarrhoea (therapeutic zinc supplementation reduces diarrhoea duration and severity — the basis for the WHO/UNICEF zinc + ORS protocol).
Vitamin A supports vision (rod and cone photoreceptors), epithelial integrity, and immune function. Requirement is 350 μg RAE/day in infancy, rising to 600-800 μg RAE/day in adolescence. Vitamin A deficiency is the leading preventable cause of childhood blindness globally; in India, the NHM provides prophylactic vitamin A supplementation at 9 months with the MR vaccine, and 6-monthly thereafter until 5 years. Vitamin D (10-15 μg/day, equivalent to 400-600 IU) is required for calcium absorption and bone mineralisation; deficiency causes rickets (bowing of long bones, craniotabes, rachitic rosary). In India, despite abundant sunshine, dark skin pigmentation, swaddling practices, and indoor upbringing contribute to widespread vitamin D insufficiency. IAP now recommends vitamin D supplementation (400 IU/day) from birth to 1 year, and continued assessment thereafter.
Iodine (90-120 μg/day in children) is essential for thyroid-hormone synthesis, which drives neurological development. Deficiency causes iodine deficiency disorders (IDD) — cretinism, goitre, cognitive impairment. Iodised salt is the cornerstone of prevention (mandatory in India under the National Iodine Deficiency Disorders Control Programme, NIDDCP).