Page 4 of 25
PE9.{2,4-7} | Nutritional Assessment Workflow — SDL Guide
Learning Objectives
- Describe the tools and methods for nutritional assessment of infants, children, and adolescents including anthropometry, dietary recall, clinical signs, and biochemical markers
- Elicit, document, and present a structured nutritional history and 24-hour dietary recall
- Calculate age-related caloric requirements and identify the caloric gap using Holliday-Segar and ICMR-NIN values
- Classify nutritional status using WHO z-scores, Gomez, Waterlow, and MUAC criteria and recognise deviations
- Plan an appropriate diet for a child in health and in common disease states using locally available Indian foods
INSTRUCTIONS
Nutritional assessment is one of the most practical and frequently performed clinical skills in paediatrics. Every growth-monitoring visit, every child with fever or diarrhoea, every hospitalised patient needs an assessment of nutritional status — not just weight, but a structured evaluation that integrates history, anthropometry, and clinical signs. This module trains you in the complete workflow from history-taking to diet prescription, with the emphasis on practical clinical technique.
References
- Ghai Essential Pediatrics, 9th ed, Ch 7 (Nutrition and Nutritional Disorders) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Section on Nutritional Assessment (textbook)
- WHO Child Growth Standards and Growth Reference Data, 2006/2007 (guideline)
- IAP Growth Charts for Indian Children 0-18 years, 2015 (guideline)
- WHO/UNICEF IMNCI Module: Assessment and Classification of Sick Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the paediatrics OPD. A mother brings her 18-month-old daughter for a routine visit. The child looks small but the mother says 'she eats fine.' Her weight is 7.8 kg. You are not sure if this is normal. You do not have a growth chart in front of you, and when you try to take a dietary history, the mother cannot estimate quantities. Meanwhile, the nurse has already moved the next patient in. This module teaches you how to perform a structured nutritional assessment efficiently — so that in 10 minutes you can have a classification, a dietary gap, and a plan.
WHY THIS MATTERS
Nutritional assessment is not a paediatric luxury — it is a mandatory clinical competency. The IAP recommends nutritional screening at every well-child visit and at every acute-care encounter where nutrition may be compromised. In hospital settings, malnutrition complicates 30-50% of paediatric admissions and increases morbidity, length of stay, and mortality. Identifying the malnourished child before admission allows earlier intervention; identifying nutritional deterioration during admission prevents it from going unnoticed. The competencies in this module (PE9.2, PE9.4–9.7) are explicitly assessed in clinical examinations and OSCE stations; they require hands-on practice to master.
RECALL
Before working through this assessment module, recall the reference values from the Normal Nutritional Needs module: the ICMR-NIN energy RDAs by age group (1000 kcal/day at 1-3 years, 1350 kcal/day at 4-6 years, etc.); the Holliday-Segar caloric formula (100 kcal/kg for first 10 kg, 50 for next 10, 20 for each additional kilogram); the macronutrient proportions (carbohydrates 50-60%, fats 25-35%, protein 10-15%); and the key micronutrient RDAs for iron, vitamin A, and zinc. Also recall from your physiology and biochemistry courses the concept of z-scores: a z-score expresses a measurement as the number of standard deviations above or below the reference median — a z-score of −2 means the child's measurement is 2 standard deviations below the median for their age and sex.
Clinical Indication: When and Why to Assess Nutrition
Nutritional assessment is indicated across a wide spectrum of clinical settings, and the practitioner must know both when to screen and when to perform a full assessment. Routine opportunistic screening — at least measuring weight, height, and MUAC — should occur at every well-child visit, at every acute consultation for any illness, and at every hospital admission. The IAP recommends formal nutritional assessment at the following intervals: monthly for children under 1 year, 3-monthly for children aged 1-3 years, and 6-monthly thereafter until school age.
Targeted assessment is indicated when: (1) weight gain has faltered or the child has crossed downward across two major centile lines; (2) the child has a chronic illness that increases metabolic demand or impairs nutrient absorption (coeliac disease, chronic kidney disease, cystic fibrosis, congenital heart disease, HIV); (3) a developmental or neurological condition impairs feeding (cerebral palsy, swallowing dysfunction); (4) growth deviation has been noted by a community health worker or parent; (5) the child has had a recent acute illness, hospitalisation, or surgery; (6) signs of specific nutrient deficiency are present (pallor, rickets, Bitot's spots, oedema).
The purpose of nutritional assessment is to: (a) classify the child's nutritional status accurately; (b) identify specific nutritional deficits; (c) quantify the caloric and nutrient gap; and (d) generate a therapeutic or preventive diet plan. These four outputs drive every subsequent management decision. Assessment without a plan is incomplete; a plan without a prior assessment is guesswork.
From a programmatic perspective, community-level nutritional screening by ASHA/AWW workers (using MUAC tape) feeds into the NHM's Nutrition Rehabilitation Centre (NRC) referral pathway. Understanding this system allows the clinician to integrate into the community-hospital continuum of care for malnourished children — a skill explicitly required by the NMC CBME competency framework.
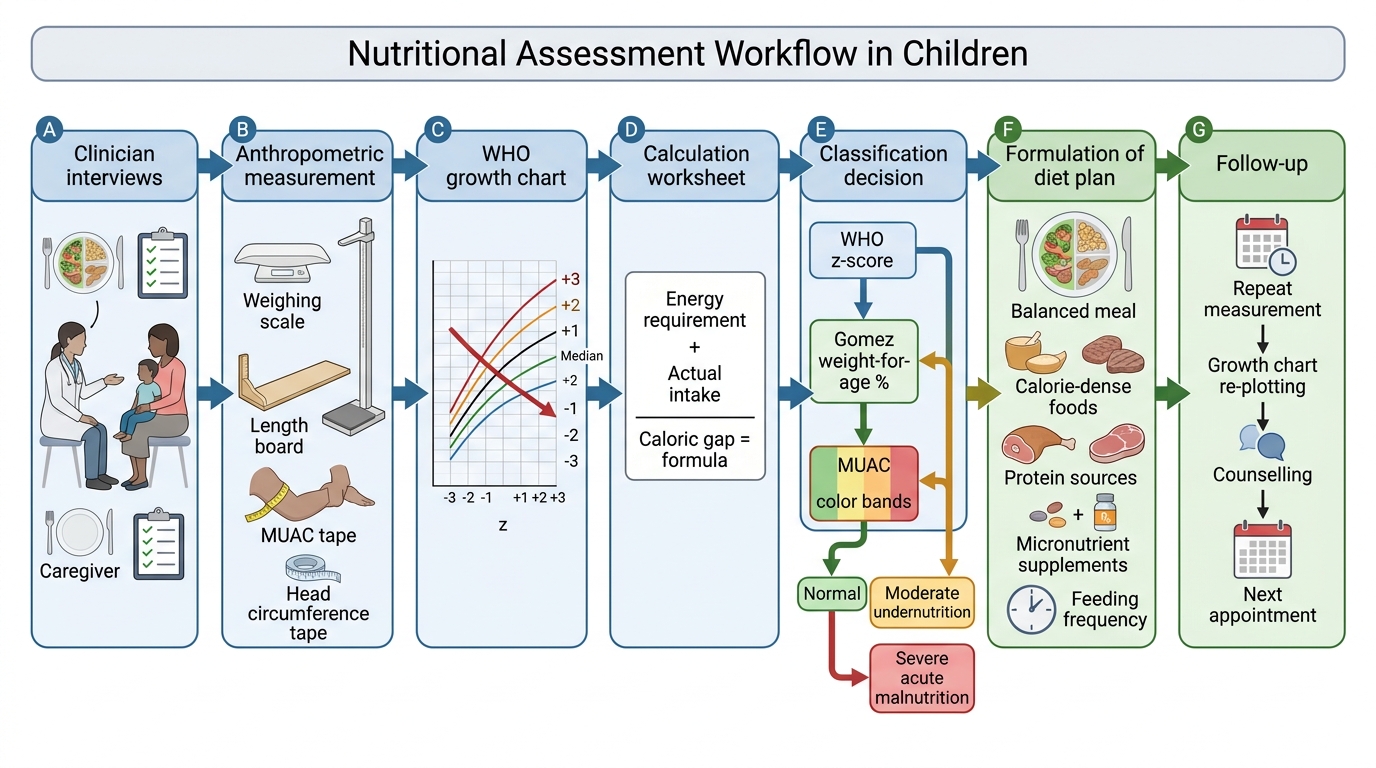
Paediatric Nutritional Assessment Workflow
Anthropometric Measurements and Growth Chart Interpretation
Anthropometry — the systematic measurement of the body — is the cornerstone of nutritional assessment in children. It is inexpensive, non-invasive, and yields objective data that can be tracked over time and compared against reference norms. There are five primary anthropometric measurements used in paediatric practice, each measuring a different aspect of nutritional status.
Provided image
Weight is the most common measurement and reflects total body mass. It should be measured with an accurate, calibrated scale — beam balance (infants and toddlers lying) or standing scale (children able to stand unsupported). Clothes, nappy, and footwear are removed. For infants, weight should be measured to the nearest 10 g; for older children, to the nearest 100 g. Serial weight measurements are more informative than a single value — the rate of weight gain and the direction of change on a growth chart matter more than the absolute number.
Supine length (0-2 years) and standing height (>2 years) are measured with an infantometer or stadiometer, respectively. Length is always measured lying for children under 2 years; errors in measurement are common (foot flexion, head position, failure to extend knees fully) and must be avoided. Height/length reflects linear growth and is sensitive to chronic nutritional deprivation — stunting (low height-for-age) develops over months to years.
Mid-upper arm circumference (MUAC) is measured on the left mid-upper arm at the midpoint between the acromion process and the tip of the olecranon, with the arm hanging relaxed at the side. A non-stretch MUAC tape (or the WHO MUAC tape with colour zones) is used. MUAC measurement is simple, requires no reference chart, and has excellent sensitivity and specificity for identifying SAM. The cut-offs are: <11.5 cm = SAM; 11.5-12.5 cm = MAM; ≥12.5 cm = normal — these apply to children aged 6-59 months. MUAC is the primary screening tool at the community level because it does not require a growth chart or scales.
Head circumference reflects brain growth and is most useful in the first 2 years. Measurement with a non-stretch tape around the largest occipital-frontal circumference. Microcephaly (<-2 SD) suggests in-utero or postnatal brain insult; macrocephaly (>+2 SD) may indicate hydrocephalus.
Skinfold thickness (triceps, subscapular) measures subcutaneous fat directly and is performed with a Harpenden calliper. It is used in research settings for body composition analysis; in routine clinical practice, it is less commonly measured than the above parameters.
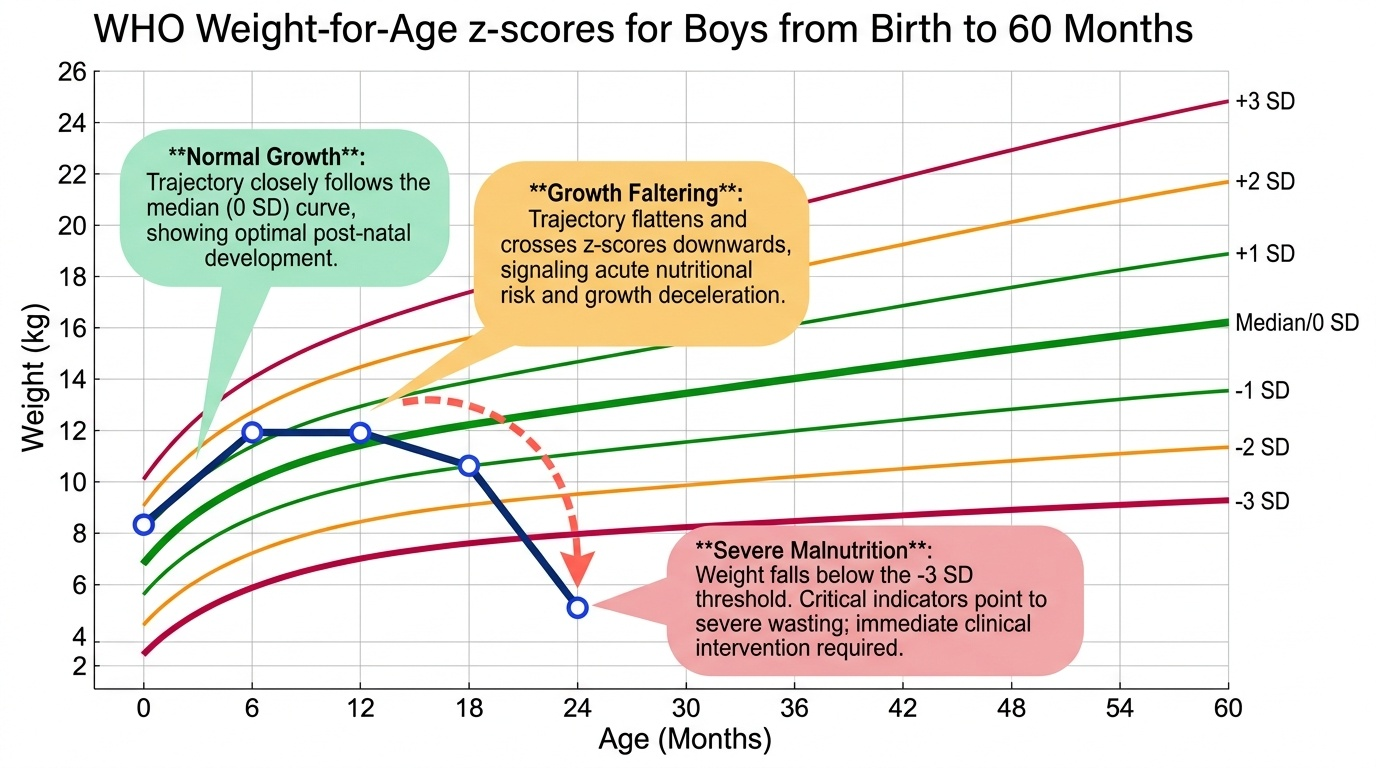
These measurements are plotted on WHO Growth Standards (0-5 years) or WHO Growth Reference (5-19 years) charts. The WHO Standards are prescriptive — they describe how healthy children should grow when all conditions are optimised (multi-country cohort). In India, the IAP 2015 growth charts provide an Indian-specific reference for clinical use. Each chart plots the measurement against age with z-score lines (−3, −2, −1, median, +1, +2, +3) and percentile lines. A measurement between −2 and +2 z-scores is within normal range; below −2 z-scores is flagged as deviation.
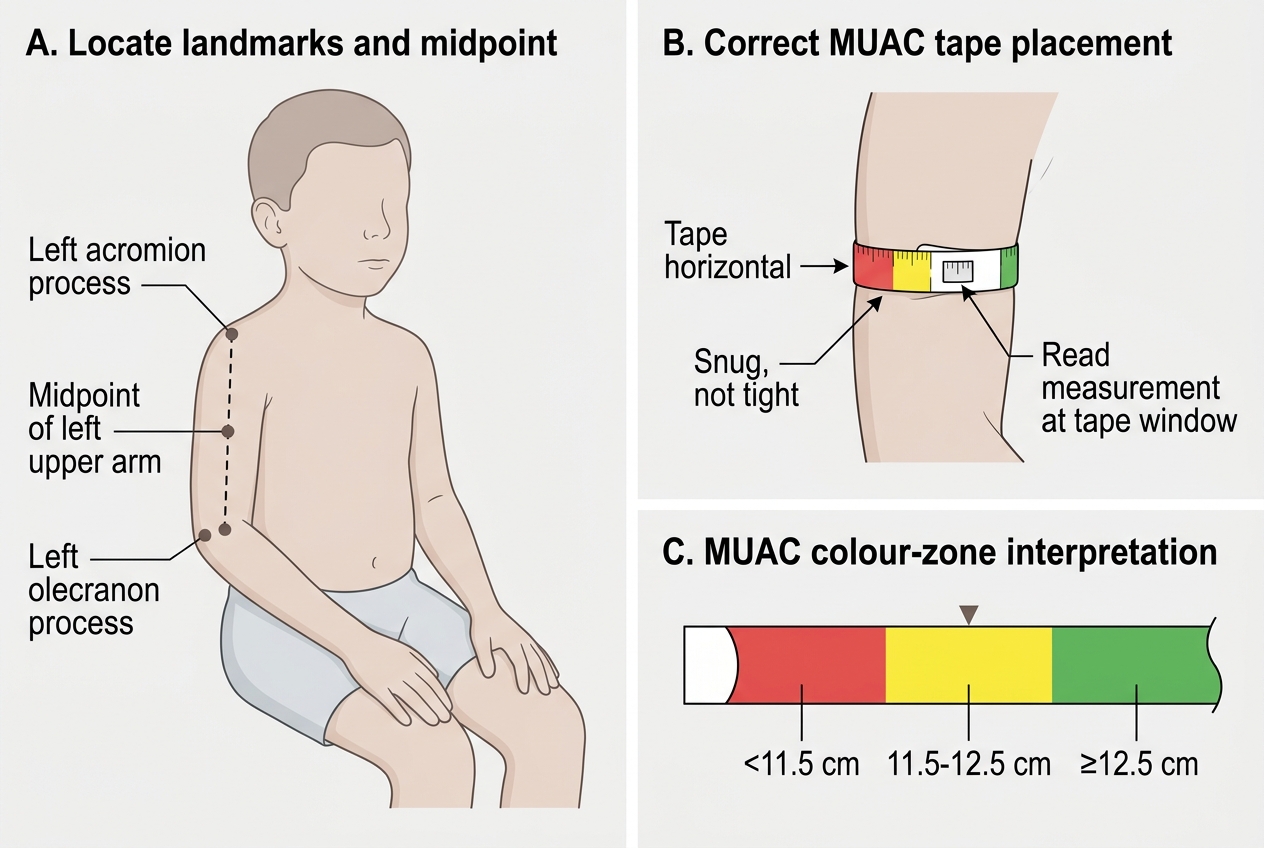
MUAC Measurement Technique in a Child
Nutritional History and Dietary Recall
A comprehensive nutritional history integrates feeding history, current dietary pattern, and a quantitative dietary assessment. It must be elicited systematically, documented clearly, and presented in a format that allows caloric gap calculation. Final-year students and interns are expected to perform this at every nutritional assessment encounter. The nutritional history is not a single question ('What does the child eat?') but a structured interview that begins at birth and traces the entire feeding journey to the present. Taking an inadequate history — one that omits breastfeeding duration, complementary feeding timing, or current meal frequency — is a common clinical error that leads to an incomplete diagnosis and an ineffective diet prescription. The purpose of the history is to understand not just what the child eats, but how much, how often, how it is prepared, who prepares it, and whether any social, economic, or cultural constraints limit dietary access.
The structured nutritional history begins with the infant's or child's feeding journey:
• Breastfeeding history: Was the child breastfed? If yes, when was breastfeeding started (ideally within 1 hour of birth), was it exclusive for 6 months, and when was it stopped? If not breastfed, what formula was used and how was it prepared (correct dilution is critical — over-diluted formula = inadequate calories).
• Complementary feeding: At what age were solids introduced? What types of foods? Were they energy-dense or primarily watery? How many meals per day at each age?
• Current diet pattern: What does the child eat on a typical day — meals, snacks, beverages? Who prepares food and how? Are there food taboos, preferences, or economic constraints?
• Appetite assessment: Is the child's appetite normal or reduced? Reduced appetite is an important symptom of micronutrient deficiency (iron, zinc) and chronic illness.
The 24-hour dietary recall is the standard quantitative method for estimating a child's actual intake over the previous day. It involves asking the caregiver to describe — in as much detail as possible — everything the child ate and drank in the past 24 hours, including portion sizes, preparation methods, and meal timing. The clinician converts this into estimated calories and macronutrients using standard food composition tables (ICMR-NIN Nutritive Value of Indian Foods).
Technique for a reliable recall:
1. Use open-ended prompts: 'Tell me everything Raju ate and drank yesterday, starting from when he woke up.'
2. Probe for forgotten items: 'Any snacks? Biscuits? Tea? Milk? Water?'
3. Estimate quantities using household measures (cups, spoons, handfuls) or food models if available.
4. Avoid leading questions ('Did he eat dal at lunch?').
5. Complete at least 2-3 non-consecutive day recalls for routine assessment; a single-day recall is acceptable for screening.
Limitations of 24-hour recall: recall bias (underestimation by ~10-20%), day-to-day variability in intake, caregiver inability to estimate portions accurately. These are minimised by multiple-day recalls and use of visual aids.
The food frequency questionnaire (FFQ) is a complementary tool that asks how often (daily, weekly, monthly) the child eats specific food groups. It provides information on dietary diversity, micronutrient coverage, and usual dietary pattern rather than precise caloric intake. A simple clinical FFQ includes: cereals, pulses, dairy, eggs/meat, green leafy vegetables, other vegetables, fruits, and processed/snack foods — scored by frequency.
SELF-CHECK
A mother is giving a 24-hour dietary recall for her 3-year-old. She says the child 'had dal-rice twice and some biscuits.' What is the BEST next step in the recall process?
A. Record this as approximately 800 kcal and move on
B. Ask leading questions: 'Did she have milk in the morning?'
C. Probe for quantities using household measures and ask about any forgotten items with open-ended prompts
D. Skip the recall and rely on anthropometry alone
Reveal Answer
Answer: C. Probe for quantities using household measures and ask about any forgotten items with open-ended prompts
A 24-hour dietary recall requires probing for quantities using household measures (cups, spoons, handfuls) and non-leading open-ended follow-up questions to improve completeness ('What else did she have?' rather than 'Did she have milk?'). Recording without quantities is inaccurate, and leading questions introduce recall bias. Anthropometry alone cannot quantify the dietary deficit.