Page 9 of 25
PE10.1-5 | Severe Acute Malnutrition — SDL Guide (Part 2)
WHO 10-Step Management Protocol
The WHO 10-step management protocol is the internationally validated framework for inpatient SAM management. It is structured into two consecutive phases: the stabilisation phase (typically days 1-7, using F-75) addresses immediate life-threatening problems without attempting rapid weight gain; and the rehabilitation phase (weeks 2-6, using F-100 or RUTF) achieves controlled catch-up growth. Understanding the rationale for the two-phase approach is as important as knowing the steps themselves — attempting rapid nutrition in the stabilisation phase causes refeeding syndrome (hypophosphataemia, heart failure), which is the commonest cause of preventable in-hospital death in SAM. Each of the 10 steps has a specific sequence and rationale that reflects the physiological priorities of the SAM child. Steps 1-2 (hypoglycaemia and hypothermia) are immediate emergencies that can kill within hours if unaddressed; steps 3-6 (dehydration, electrolytes, infection, micronutrients) represent the biochemical stabilisation phase that must precede any attempt at nutritional rehabilitation; steps 7-10 represent the graduated nutritional build-up that drives catch-up growth and community reintegration. The steps are not interchangeable — skipping or reordering them is a protocol deviation that increases mortality.
The 10 steps are commonly grouped by phase:
Stabilisation phase (Steps 1-7):
1. Treat/prevent hypoglycaemia — blood glucose <3 mmol/L (54 mg/dL): give 10% dextrose 5 mL/kg IV bolus; if IV access unavailable, 10% glucose 50 mL via NGT; feed every 2-3 hours (never fast the child for more than 2 hours in the first 48 hours).
2. Treat/prevent hypothermia — temperature <35.5°C axillary: skin-to-skin (kangaroo mother care), warm blanket, warm room ≥25°C, hat and socks, avoid draughts and wet nappy; feed immediately (feeding warms the body from within).
3. Treat/prevent dehydration — use ReSoMal (not standard ORS): 5 mL/kg every 30 minutes for 2 hours by NGT (if IV, use Ringer's lactate with 5% dextrose; IV is for only for severe shock or oral/NGT not possible); reassess every 30 min for signs of over-hydration (rising respiratory rate, increasing oedema).
4. Correct electrolyte imbalance — potassium 3-4 mmol/kg/day, magnesium 0.4-0.6 mmol/kg/day added to feeds; do NOT give sodium supplements (hyponatraemia in SAM is dilutional, not true sodium deficit — sodium worsens oedema).
5. Treat/prevent infection — empirical broad-spectrum antibiotics per WHO protocol: amoxicillin 25 mg/kg/dose orally 8-hourly for 5 days (uncomplicated); add gentamicin if systemically unwell; specific antibiotic adjustments for identified infections.
6. Correct micronutrient deficiencies — give a combined micronutrient supplement: vitamin A (100,000 IU for 6-12 months, 200,000 IU for ≥12 months on Day 1 only unless signs of current vitamin A deficiency), folic acid 5 mg on Day 1 then 1 mg/day, zinc 2 mg/kg/day, copper 0.3 mg/kg/day, multivitamin; do NOT give iron in the first week (worsens infection in iron-replete environments).
7. Begin cautious feeding — F-75: 100-130 mL/kg/day in 8-12 feeds; never exceed 130 mL/kg/day in stabilisation.
Rehabilitation phase (Steps 8-10 + transition from Step 7):
7 (continued)/8. Transition to F-100 and achieve catch-up growth — shift to F-100 when: oedema resolving + appetite returning + child appears brighter. Increase volume from 100 mL/kg/day to 150-220 mL/kg/day over 2-3 days to achieve weight gain of 10-15 g/kg/day (catch-up growth target).
9. Provide sensory stimulation and emotional support — structured play, sensory stimulation, tender loving care; malnutrition impairs neurological development and catch-up is enhanced by structured stimulation.
10. Prepare for follow-up after recovery — discharge criteria: WHZ > −2 SD for 2 consecutive weighings + no oedema + good appetite + no medical complication; set up community follow-up schedule; enrol in supplementary feeding programme if needed.
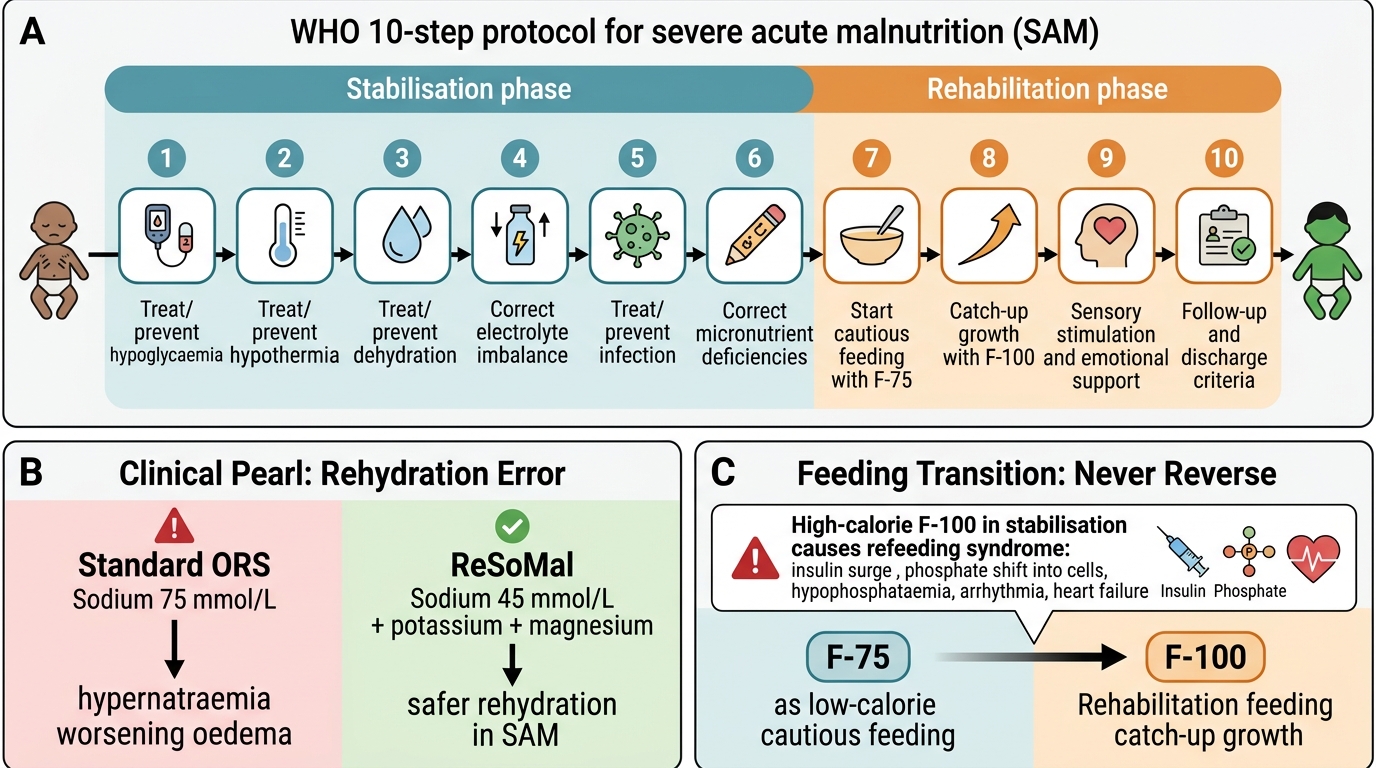
WHO 10-Step Management of Severe Acute Malnutrition
CLINICAL PEARL
The two most common fatal errors in SAM management in India are: (1) giving standard ORS instead of ReSoMal for rehydration; and (2) starting high-calorie feeding (F-100 volumes) in the stabilisation phase. Standard ORS has 75 mmol/L sodium — in a SAM child whose renal sodium handling is already impaired and whose sodium is dilutionally low, this causes dangerous hypernatraemia and worsens oedema. ReSoMal has only 45 mmol/L sodium with added potassium and magnesium. The second error — over-feeding in stabilisation — causes refeeding syndrome: when large quantities of carbohydrate are provided to a chronically starved body, insulin surges, intracellular uptake of phosphate is triggered, and serum phosphate crashes → cardiac arrhythmia and heart failure. F-75 is deliberately low-calorie precisely to prevent this. Memorise the rule: F-75 in stabilisation, F-100 in rehabilitation — never the reverse.
Therapeutic Diets: F-75, F-100, and RUTF
The therapeutic feeding products used in SAM management have been specifically designed to meet the metabolic constraints of the severely malnourished child. Understanding their composition, their phase of use, and the rationale for their properties is essential for correct prescribing.
Provided image
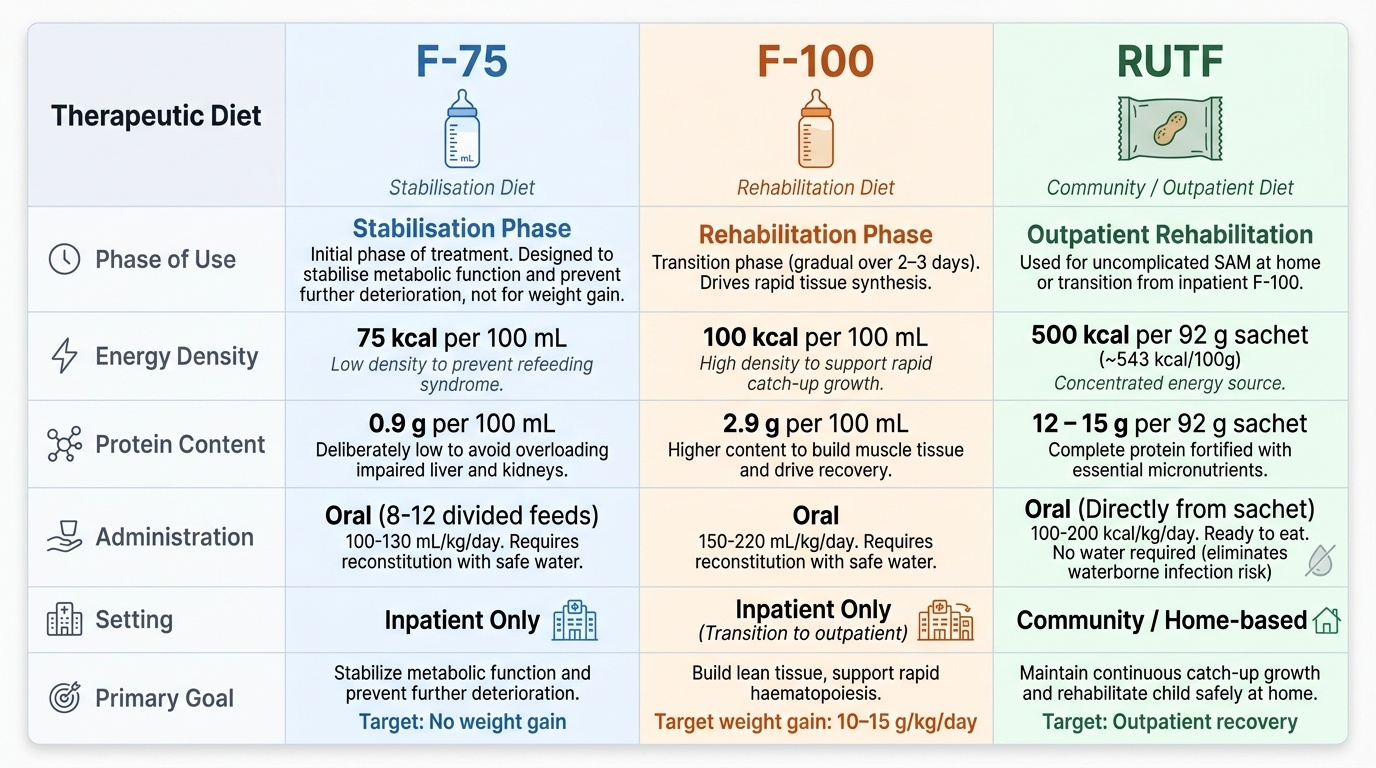
F-75 (the 'F' stands for Formula; '75' is the energy content in kcal per 100 mL) is the stabilisation-phase diet. Composition per 100 mL: 75 kcal, 0.9 g protein, 1.9 g fat, 13.3 g carbohydrate. The deliberately low protein content avoids overwhelming the impaired hepatic and renal function of the SAM child; the low energy density prevents refeeding syndrome. F-75 is not designed to promote weight gain — it is designed to stabilise metabolic function and prevent further deterioration. It is given at 100-130 mL/kg/day in 8-12 divided feeds around the clock. In India, F-75 can be prepared locally from dried skimmed milk + oil + sugar + water to an approximate recipe — NRC staff are trained in its preparation; alternatively, commercial sachets (Insta-F75) are available.
F-100 is the rehabilitation-phase diet: 100 kcal/100 mL, 2.9 g protein, 5.4 g fat, 10.8 g carbohydrate. Higher protein and energy density drive rapid tissue synthesis and catch-up weight gain. F-100 is given at 150-220 mL/kg/day to achieve target weight gain of 10-15 g/kg/day. The shift from F-75 to F-100 is gradual over 2-3 days to prevent sudden metabolic overload. Iron supplementation is started in the rehabilitation phase (not stabilisation) to support haematopoiesis.
RUTF (Ready-to-Use Therapeutic Food) — commercially, Plumpy'Nut is the best-known brand; Indian NHMs also procure or manufacture locally. Composition per 92 g sachet: 500 kcal, 12-15 g protein, 28-31 g fat, with complete micronutrient fortification. Key advantage: does not require water for preparation (eliminating infection risk) and can be stored at ambient temperature for months. RUTF is used for: (1) uncomplicated SAM managed as outpatients; (2) transition from inpatient F-100 to community discharge; (3) treatment of SAM at home in the community-based management (CbM) arm of NHM. The standard RUTF dose is 100-200 kcal/kg/day, adjusted for weight gain.
Locally Prepared Therapeutic Foods (LPTF) use locally available ingredients (full-fat dried milk, oil, sugar, peanuts) to prepare a product with approximately F-75 or F-100 composition. The IAP and NHM have published standardised recipes. LPTF are important where commercial RUTF is not available or affordable.
Appetite test procedure: offer the child 1/4 sachet of RUTF (approximately 23 g, 125 kcal). The test is passed if the child eats the entire 1/4 sachet without coercion, vomiting, or extreme reluctance within approximately 30 minutes. A passed appetite test indicates functional gastrointestinal capacity and absence of severe anorexia — the child can absorb therapeutic food taken orally and is a candidate for outpatient management.
Complication Management: Hypoglycaemia, Hypothermia, Dehydration, and Infection
The four life-threatening acute complications of SAM — hypoglycaemia, hypothermia, dehydration/shock, and sepsis — each require specific, protocol-driven management that differs in important ways from standard paediatric practice. These complications are inter-related and mutually aggravating: hypothermia impairs glucose production and worsens hypoglycaemia; dehydration reduces cardiac output and worsens electrolyte imbalance; the immune suppression of SAM makes sepsis more likely, more rapid, and more difficult to recognise (fever may be absent). Recognising and treating all four simultaneously, or in rapid sequence, is the core skill of SAM emergency management and the reason trained NRC nurses follow a checklist at every admission. The management of each complication in SAM is distinct from the management in a well-nourished child — clinicians who apply standard resuscitation protocols without SAM-specific modifications cause iatrogenic harm. The three most common harmful deviations are: using 50% dextrose instead of 10%, using standard ORS instead of ReSoMal, and giving excess IV sodium-containing fluids.
Hypoglycaemia is defined in SAM as blood glucose <3 mmol/L (54 mg/dL), though symptomatic hypoglycaemia may occur at somewhat higher levels due to impaired counter-regulatory response. Management:
• Conscious child: oral/NGT 10% glucose (dextrose) 50 mL immediately, then feed every 2-3 hours around the clock
• Unconscious or unable to feed orally: 10% dextrose (D10W) 5 mL/kg IV bolus, then continuous feeding via NGT
• Never use 50% dextrose (D50W) in children — hypertonic, causes thrombophlebitis and osmotic injury
• Prevention: feed every 2-3 hours (no fasting periods longer than 2 hours); a bedside glucose check on admission and at 30-minute intervals until stable
Hypothermia (axillary temperature <35.5°C): the malnourished child has reduced subcutaneous fat, low metabolic rate, and impaired thermogenesis.
• Cover with warm blanket and hat, keep room temperature ≥25°C, avoid wet nappy or wet clothes
• Kangaroo mother care (skin-to-skin contact with mother) is the most effective warming method
• Feed immediately — enteral feeding generates heat via thermogenesis
• Avoid excessive bathing; avoid draughts and cold examining tables
• Monitor temperature every 30 minutes until ≥36.5°C
Dehydration in SAM is difficult to assess because the usual signs (skin turgor, fontanelle) are unreliable (skin is loose from wasting; oedema confounds assessment). Clinical signs that remain useful: sunken eyes, absent tears, dry mucous membranes, altered consciousness. Management:
• Use ReSoMal exclusively — NOT standard WHO ORS; ReSoMal: sodium 45 mmol/L, potassium 40 mmol/L, magnesium 3 mmol/L, 300 mOsm/L (vs ORS 245 mOsm/L but lower sodium)
• Give 5-10 mL/kg ReSoMal every 30 minutes for 2 hours by mouth or NGT
• Reassess at 30-minute intervals for signs of over-hydration: rising respiratory rate, increasing oedema, puffy eyelids
• IV fluids are reserved for shock only: use Ringer's lactate with 5% dextrose 15 mL/kg over 1 hour
• Total fluid in stabilisation: 100-130 mL/kg/day (from all sources including feeds)
Infection is universal in SAM — even without obvious fever. SAM impairs neutrophil function, T-cell immunity, and mucosal barriers, making the child susceptible to bacterial, fungal, and viral infections simultaneously. A child with SAM who looks well and is afebrile may still be bacteraemic.
• Empirical antibiotics per WHO/NHM protocol for all SAM admissions: amoxicillin 25 mg/kg orally 8-hourly for 5 days (if no complications); add gentamicin 7.5 mg/kg/day IV (weight-based) if systemically unwell or shocked
• Treat specific identified infections (pneumonia, UTI, meningitis) with appropriate targeted antibiotics
• Malaria testing in endemic areas; treat if positive
• Avoid prophylactic antifungals routinely; treat candidiasis if evident