Page 14 of 33
PE12.7 | B Complex Vitamins — SDL Guide (Part 2)
Clinical Features and Deficiency Syndromes
The clinical syndromes produced by B vitamin deficiency are among the most important nutritional diagnoses in paediatric medicine, each with a characteristic signature that enables bedside recognition.
Beriberi (Thiamine / B1 deficiency): Two distinct paediatric forms exist. Infantile wet beriberi presents acutely in the first 2–6 months of age in breastfed infants of thiamine-deficient mothers. The infant develops tachycardia, cardiomegaly, hepatomegaly, oedema, and dyspnoea — high-output cardiac failure from thiamine-deficient myocardium. If untreated, it progresses rapidly to cardiovascular collapse. Dry beriberi presents later with peripheral neuropathy — the child walks with a foot-drop gait, has diminished reflexes and sensory loss, and may complain of burning paraesthesiae. In older children and adolescents who also consume alcohol (or in malnourished hospitalised patients receiving dextrose without thiamine), Wernicke's encephalopathy (ophthalmoplegia, ataxia, confusion) can occur; crucially, administering intravenous dextrose without thiamine first can precipitate acute Wernicke's by flooding TPP-deficient neurones. Diagnosis: elevated blood pyruvate and lactate; erythrocyte transketolase activity (reduced); low whole-blood thiamine. Management: thiamine 10–25 mg IM or IV immediately, then orally; cardiac failure responds within hours; neurological recovery is slower.
Pellagra (Niacin / B3 deficiency): The classic presentation is the 3 Ds: Dermatitis, Diarrhoea, and Dementia (the 4th D, untreated, is Death). The dermatitis has a striking photosensitive distribution — symmetric, hyperpigmented, scaly, desquamating lesions on sun-exposed areas; Casal's necklace (the band around the neck) and glove-and-stocking pattern on the hands and feet are pathognomonic. The diarrhoea is secondary to inflammatory enteritis. Neuropsychiatric features include irritability, confusion, hallucinations, and dementia. In children in India, pellagra is seen in drought-affected areas where families depend on maize as the sole cereal. Secondary pellagra can occur with isoniazid (which competes with NAD precursors), Hartnup disease (impaired tryptophan absorption), and carcinoid syndrome (tryptophan diversion). Management: nicotinamide (niacinamide) 100–300 mg/day orally in divided doses; nicotinic acid is avoided due to flushing; dermatitis heals within weeks; neuropsychiatric features may persist if severe and prolonged.
Megaloblastic Anaemia (Folate / B9 and Cobalamin / B12 deficiency): Both folate and B12 deficiency impair DNA synthesis, causing megaloblastic erythropoiesis — large, oval macrocytes and hypersegmented neutrophils (≥5 lobes in >5% of neutrophils) on the blood film. The child presents with insidious pallor, fatigue, glossitis, and mild jaundice from ineffective erythropoiesis. The critical distinction is that B12 deficiency — and ONLY B12 deficiency — causes subacute combined degeneration (SCD) of the spinal cord: demyelination of posterior (proprioception, vibration loss) and lateral (spastic weakness) columns, producing gait ataxia, positive Romberg test, and upper motor neuron signs. Infants of vegan mothers may present with neurological regression (hypotonia, developmental delay) before anaemia becomes apparent, because foetal stores are deposited in the third trimester. Treating B12-deficient megaloblastic anaemia with folate alone corrects the haematology but DOES NOT prevent neurological deterioration — a common and dangerous clinical trap. Diagnosis: MCV >100 fL; peripheral smear (hypersegmented neutrophils + oval macrocytes); serum B12 (<200 pg/mL = deficient); serum folate (<3 ng/mL); methylmalonic acid elevated in B12 (not folate) deficiency. Management: B12 deficiency — cyanocobalamin or hydroxocobalamin IM; daily oral B12 1000 mcg if no malabsorption. Folate deficiency — folic acid 1–5 mg/day orally. Always establish the cause.
Pyridoxine-responsive seizures (B6 / pyridoxine): An important paediatric emergency. Neonates and infants may present with refractory seizures that do not respond to standard antiepileptic drugs. The mechanism is either pyridoxine-dependent epilepsy (antiquitin deficiency — ALDH7A1 gene mutation, causing pipecolic-acid accumulation and GABA deficiency) or severe dietary B6 deficiency. The clinical test: IV pyridoxine 100 mg administered during a seizure — cessation within minutes confirms B6-responsive epilepsy. Ongoing treatment: pyridoxine 15–30 mg/kg/day. INH-induced B6 deficiency neuropathy is prevented by co-prescribing pyridoxine 1–2 mg/kg/day.
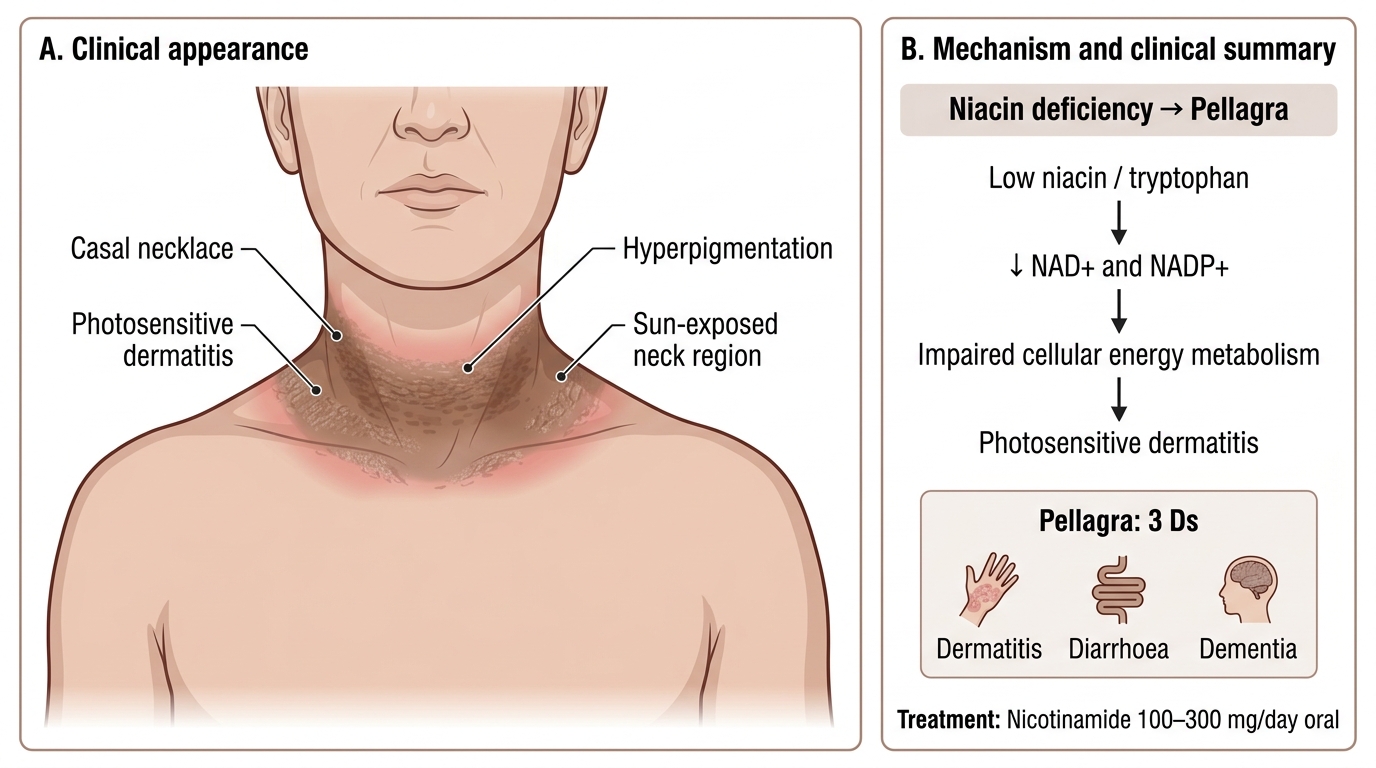
Casal Necklace in Pellagra
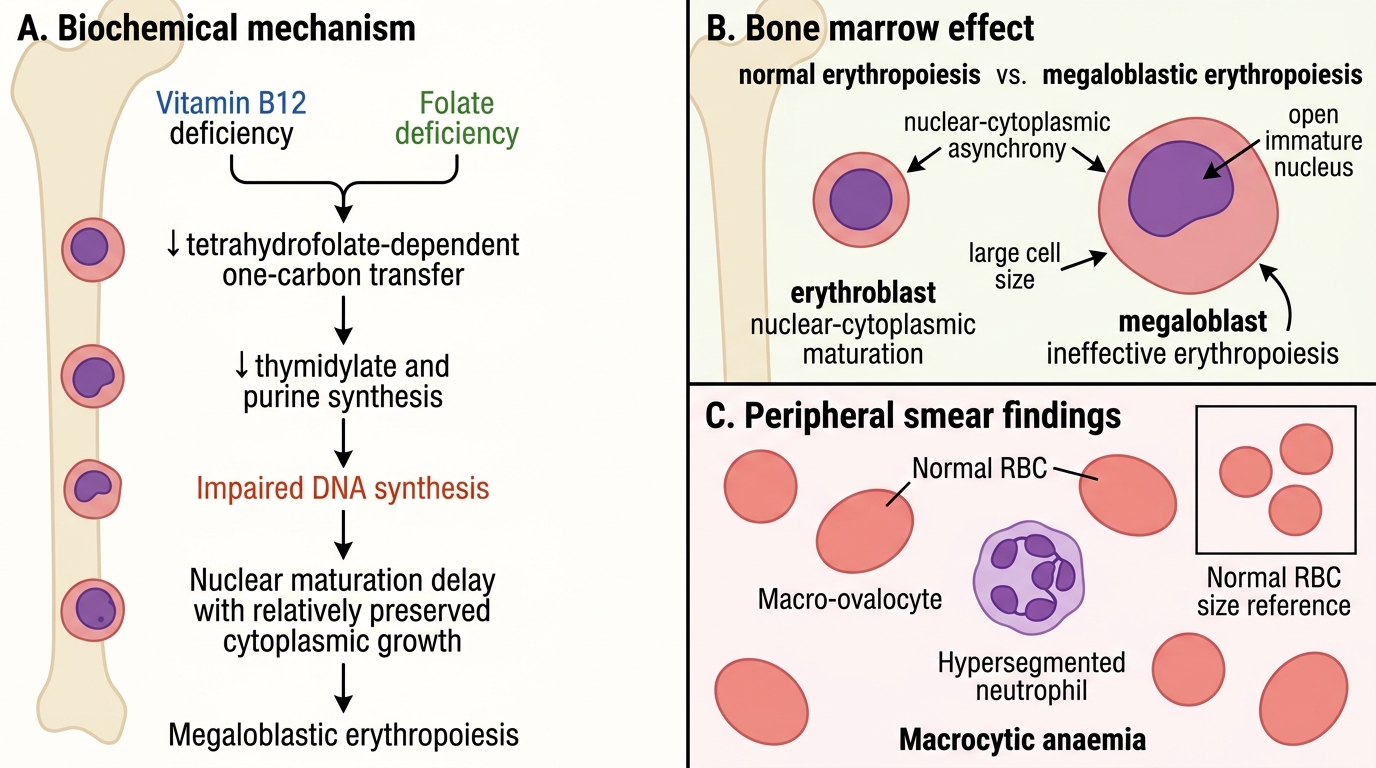
Pathogenesis of Megaloblastic Anaemia
| Deficiency | Syndrome | Key clinical features | Treatment |
|---|---|---|---|
| B1 (thiamine) | Beriberi | Wet: cardiac failure + oedema (infant); Dry: peripheral neuropathy | Thiamine 10–25 mg IM/IV stat, then oral |
| B3 (niacin) | Pellagra | 3 Ds: Dermatitis + Diarrhoea + Dementia; Casal's necklace | Nicotinamide 100–300 mg/day oral |
| B9 (folate) | Megaloblastic anaemia | Macrocytic anaemia, NO neurological SCD | Folic acid 1–5 mg/day |
| B12 (cobalamin) | Megaloblastic anaemia + SCD | Macrocytic anaemia + posterior/lateral column signs | Cyanocobalamin IM (+ oral if no malabsorption) |
| B6 (pyridoxine) | Seizures / neuropathy | Refractory neonatal seizures; INH neuropathy | Pyridoxine IV 100 mg (acute); 15–30 mg/kg/day |
| B2 (riboflavin) | Ariboflavinosis | Angular stomatitis, glossitis, corneal vascularisation | Riboflavin 5–10 mg/day |
CLINICAL PEARL
Three B-vitamin traps to remember in clinical practice:
1. Never give IV dextrose without thiamine first in a malnourished or at-risk child — the glucose load floods TPP-depleted neurones and precipitates acute Wernicke's encephalopathy.
2. Treating megaloblastic anaemia with folate alone without ruling out B12 deficiency corrects the blood count but allows subacute combined degeneration to progress silently — always check B12 levels first, or treat both if B12 cannot be measured urgently.
3. INH + pyridoxine must go together — any child started on isoniazid (TB prophylaxis or treatment) should receive concurrent pyridoxine 1–2 mg/kg/day to prevent peripheral neuropathy and seizures.
Self-Assessment
Self-assessment through clinical vignettes is one of the most effective ways to consolidate your knowledge of B complex vitamin deficiencies, because these syndromes are distinguished not by laboratory results alone but by the contextual clues embedded in the clinical story — the age of the child, the mother's dietary history, the type of community the family lives in, and the pattern of symptoms. Use the scenarios below to practise pattern recognition: identify the most at-risk nutritional deficiency for each context, reason through the pathophysiology, and arrive at a specific diagnosis before looking at the questions. This mirrors the clinical reasoning process you will use in your paediatric postings when laboratory investigations may not be immediately available and empirical treatment must be considered.
Vignette 1: A 2-month-old infant presents with acute onset rapid breathing, tachycardia, and oedema. His mother is a 20-year-old vegetarian who subsists on polished rice and vegetables. The infant is exclusively breastfed.
• What is the most likely diagnosis?
• Which immediate treatment should be given?
• What is the mechanism by which cardiac failure develops?
Vignette 2: A 7-year-old girl from a tribal village presents with symmetric, darkly pigmented, scaly skin lesions on her hands, forearms, and a band-like lesion around her neck. She also has diarrhoea and appears confused. The family's main food is maize.
• Name the deficiency syndrome and its causative vitamin.
• What is the pathognomonic skin sign around her neck called?
• What treatment will you prescribe?
Vignette 3: A 10-month-old infant, exclusively breastfed by a vegan mother, presents with hypotonia, developmental regression (had been achieving milestones normally up to 5 months), and pallor. Blood film shows macrocytic anaemia and hypersegmented neutrophils. Serum B12 is 98 pg/mL.
• What condition does this infant have?
• Why is neurological damage occurring despite the infant appearing well-fed?
• Why should folate alone NOT be given?
• What treatment will you start?
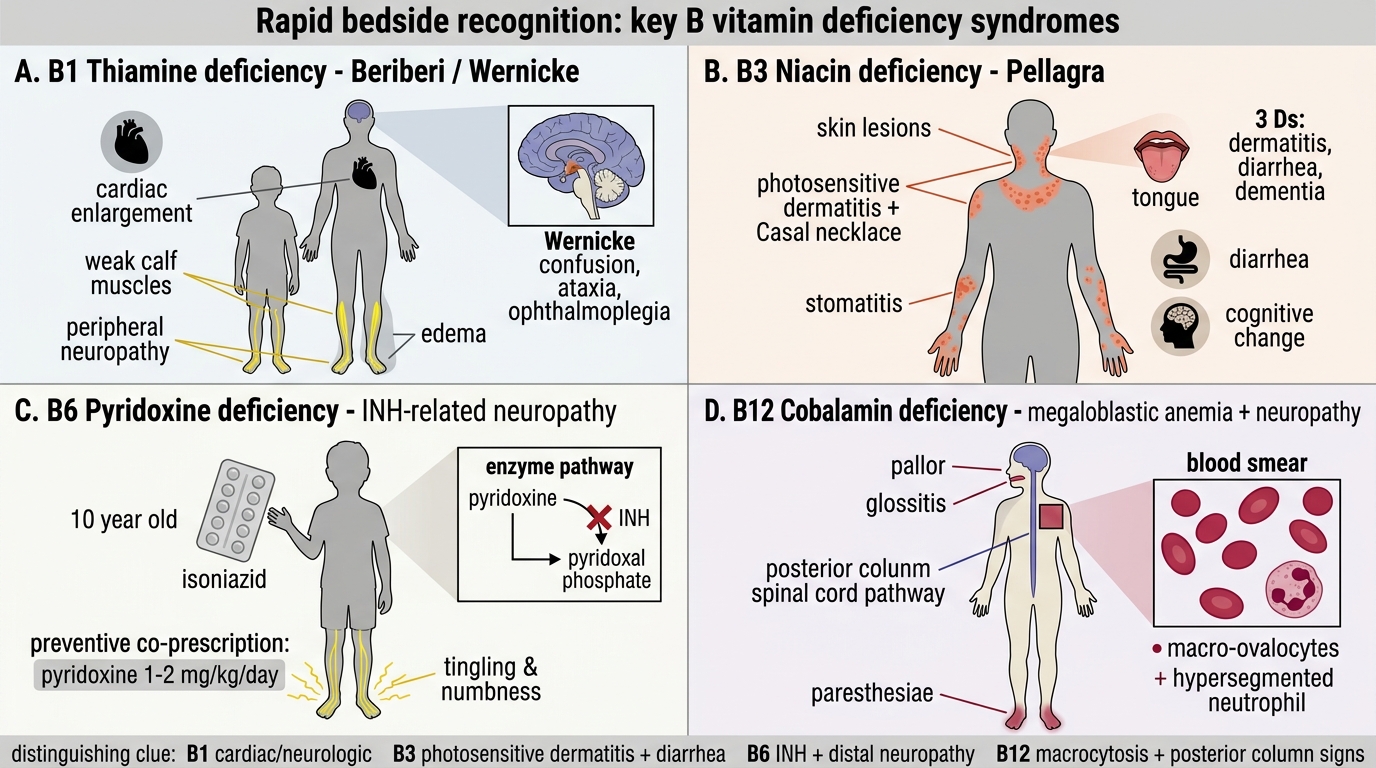
Rapid Recognition of Key B Vitamin Deficiency Syndromes
SELF-CHECK
A 10-year-old child on isoniazid for TB treatment develops numbness and tingling in both feet. Which B vitamin deficiency is responsible, and what is the preventive co-prescription?
A. B1 (thiamine) deficiency — co-prescribe thiamine 10 mg/day
B. B3 (niacin) deficiency — co-prescribe nicotinamide 100 mg/day
C. B6 (pyridoxine) deficiency — co-prescribe pyridoxine 1–2 mg/kg/day
D. B12 (cobalamin) deficiency — co-prescribe cyanocobalamin IM monthly
Reveal Answer
Answer: C. B6 (pyridoxine) deficiency — co-prescribe pyridoxine 1–2 mg/kg/day
Isoniazid (INH) inhibits pyridoxine phosphokinase, the enzyme that converts dietary pyridoxine (B6) to its active coenzyme form, pyridoxal phosphate (PALP). PALP is required for neurotransmitter synthesis and peripheral nerve maintenance. The resulting B6 deficiency manifests as peripheral neuropathy (sensory loss, paraesthesiae). All children receiving INH should be co-prescribed pyridoxine at 1–2 mg/kg/day as prophylaxis. B12 deficiency from metformin (not INH) causes neuropathy; niacin and thiamine are not depleted by INH.