Page 25 of 33
PE13.4 | Calcium Magnesium Nutrition — SDL Guide
Learning Objectives
- State the ICMR/NIN 2020 recommended dietary allowances (RDA) for calcium and magnesium across age groups from infancy to adolescence.
- List the principal dietary sources of calcium and magnesium, including Indian food sources, and describe factors that affect their bioavailability.
- Explain the mechanisms of calcium homeostasis, including the roles of parathyroid hormone (PTH), 1,25-dihydroxyvitamin D, calcitonin, and the inverse calcium-phosphate relationship.
- Describe how magnesium deficiency impairs PTH secretion and end-organ responsiveness, producing refractory hypocalcaemia.
- Distinguish early-onset from late-onset neonatal hypocalcaemia by timing, aetiology, clinical features, and management.
- Identify the clinical features of hypocalcaemic tetany (Trousseau sign, Chvostek sign, laryngospasm, seizures) and describe emergency and maintenance management.
- Describe the aetiology, clinical features (including rachitic rosary, frontal bossing, X-ray changes), and management of nutritional rickets in Indian children.
- Recognise and manage hypomagnesaemia, including its role as a cause of refractory hypocalcaemia.
INSTRUCTIONS
Calcium and magnesium are the two most abundant macro-minerals in the human body and are indispensable for skeletal development, neuromuscular function, cardiac conduction, and hundreds of enzymatic reactions. In India, nutritional calcium deficiency contributing to rickets and hypocalcaemic tetany remains a clinical reality in paediatric outpatient departments. Final-year medical students must be able to counsel families on dietary sources, calculate needs against ICMR/NIN standards, recognise deficiency states ranging from a seizing neonate to a toddler with bowing legs, and understand the often-missed link between magnesium depletion and refractory hypocalcaemia. This SDL builds that competency using the PE-foundation arc: from clinical relevance through normal physiology, homeostatic mechanisms, to applied diagnosis and management.
References
- Ghai Essential Pediatrics, 9th edition, Ch 8 — Nutrition (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 67 — Calcium, Magnesium, and Phosphorus (textbook)
- ICMR-NIN Recommended Dietary Allowances and Estimated Average Requirements for Indians, 2020 (guideline)
- IAP Guidelines on Vitamin D and Calcium Deficiency in Children, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 18-month-old boy is brought to the paediatric OPD by his mother, who is alarmed because the child's legs have been bowing outward for the past two months and he appears listless. On examination, his wrists are widened, there is a palpable beading along the costochondral junctions, and his anterior fontanelle is still open. A week later in the neonatal unit, a 3-day-old preterm infant born at 34 weeks gestation suddenly develops jitteriness and a brief generalised seizure. Serum calcium comes back at 6.4 mg/dL. In both cases, the same mineral — calcium — is at the centre of the clinical problem, yet the mechanisms and contexts are entirely different. And in a third scenario, a 4-year-old girl with persistent diarrhoea and refractory hypocalcaemia despite calcium and vitamin D supplementation turns out to have serum magnesium of 1.1 mg/dL, and recovers only once magnesium is replaced. These cases illustrate why calcium and magnesium nutrition must be understood together, as a linked homeostatic system.
WHY THIS MATTERS
Calcium and magnesium deficiency states are among the most common and clinically significant nutritional problems in Indian paediatric practice. Nutritional rickets — caused by combined calcium and vitamin D deficiency — affects toddlers across India, with the highest burden in low-sunlight winter months in northern India, though dietary calcium inadequacy is a year-round driver in many regions. Neonatal hypocalcaemia is a leading cause of neonatal seizures in premature infants and term infants fed unmodified cow's milk. Hypomagnesaemia is frequently overlooked, yet it is the key to unlocking refractory hypocalcaemia in children with malabsorptive conditions. As a final-year medical student, you will be the first-line clinician who orders the serum calcium in a seizing neonate, counsels a mother on ragi and dairy intake for her toddler, and recognises that a child's calcium is not correcting because their magnesium has not been checked. The NMC CBME 2024 competency PE13.4 specifically asks you to describe RDA, dietary sources, and deficiency states for both minerals — making this a high-yield examination and clinical topic.
RECALL
Before proceeding, consolidate the following prerequisite knowledge from your Physiology (PY) and Biochemistry (BI) years:
- Calcium physiology (PY): Parathyroid hormone (PTH) is secreted by the chief cells of the parathyroid glands in response to a fall in ionised serum calcium. PTH acts on bone (osteoclast activation → Ca and phosphate release), kidney (enhanced tubular Ca reabsorption, phosphaturia, and activation of 25-OH-D → 1,25-OH2-D by 1α-hydroxylase), and indirectly on the intestine (via 1,25-OH2-D → increased Ca and phosphate absorption). Calcitonin, from thyroid C-cells, opposes PTH by inhibiting osteoclasts — though its role in day-to-day calcium homeostasis is minor in adults.
- Vitamin D activation (BI): Cholecalciferol (D3) from skin or diet is hydroxylated first in the liver to 25-OH-D (calcidiol) and then in the kidney to the active form 1,25-OH2-D (calcitriol). Deficiency of vitamin D therefore reduces intestinal calcium absorption, leading to secondary hyperparathyroidism and, ultimately, rickets or osteomalacia.
- Calcium–phosphate inverse relationship: In the extracellular fluid, calcium and phosphate concentrations are inversely related around a solubility product. High phosphate (as in cow's milk feeds in neonates) drives down ionised calcium.
- Magnesium as enzymatic cofactor (BI): Magnesium is required for the phosphate-transfer reactions of ATP; virtually all ATP-dependent reactions (kinase reactions, DNA/RNA synthesis, protein synthesis) require Mg2+ as a cofactor. Recall that Mg2+ is predominantly intracellular and that serum Mg reflects only about 2% of total body magnesium.
Why Calcium and Magnesium Matter in Paediatric Practice
Calcium is the most abundant mineral in the human body and magnesium the fourth most abundant; together they account for the structural integrity of the skeleton and the precision of neuromuscular transmission. In the paediatric context, their importance is amplified by the extraordinary demands of rapid skeletal growth: an infant's skeleton doubles its calcium content in the first year of life, and adolescents undergoing the pubertal growth spurt accumulate up to 300 mg of calcium per day in their skeleton — demands that can outstrip dietary supply if nutrition is inadequate or absorption is impaired. Magnesium's relevance in paediatrics is less immediately obvious but clinically critical: it is required for the function of parathyroid hormone itself, meaning that magnesium depletion can mimic hypoparathyroidism and produce a hypocalcaemia that will not respond to calcium or vitamin D supplementation until magnesium is replaced.
The key paediatric presentations of calcium–magnesium dysfunction are:
• Neonatal hypocalcaemia (early-onset within 72 h or late-onset after day 4) — a cause of neonatal seizures, jitteriness, and apnoea.
• Hypocalcaemic tetany — carpopedal spasm, laryngospasm, Trousseau and Chvostek signs, generalised seizures.
• Nutritional rickets — widening of epiphyses, rachitic rosary, frontal bossing, bowing of legs in toddlers.
• Refractory hypocalcaemia in children with diarrhoea or malabsorption — hypomagnesaemia as the underlying undiagnosed driver.
Understanding the clinical context for each of these presentations is the starting orientation for the rest of this SDL.
Calcium: Body Distribution, RDA, and Dietary Sources
The total body calcium in an adult is approximately 1,000 g; approximately 99% is stored in bone and teeth as hydroxyapatite crystals [Ca10(PO4)6(OH)2], which serve both a structural scaffold function and as a metabolic reservoir. The remaining 1% is distributed between the intracellular compartment (~0.9%) and the extracellular fluid (~0.1%). Within the extracellular fluid, serum calcium exists in three fractions: approximately 40% bound to albumin, 10% complexed to anions such as citrate and phosphate, and 50% as free ionised calcium — the biologically active fraction. The normal serum total calcium is 8.5–10.5 mg/dL (2.1–2.6 mmol/L), and normal ionised calcium is 4.6–5.3 mg/dL (1.15–1.33 mmol/L). An important clinical point is that albumin levels affect the measured total calcium but not the ionised fraction: for every 1 g/dL fall in serum albumin below 4 g/dL, the measured total calcium falls by ~0.8 mg/dL without a change in the physiologically active ionised calcium (corrected calcium formula).
Provided image
ICMR/NIN 2020 Recommended Dietary Allowances for Calcium:
| Age group | RDA (mg/day) | Note |
|---|---|---|
| 0–6 months | 200 (AI) | Adequate Intake from breast milk |
| 7–12 months | 260 (AI) | AI from breast milk + complementary foods |
| 1–3 years | 700 | Critical toddler window |
| 4–8 years | 1000 | School-age |
| 9–18 years | 1300 | Highest — pubertal skeletal accretion |
Adolescents have the highest calcium RDA (1300 mg/day) because the pubertal growth spurt demands rapid skeletal mineralisation. Meeting this requirement from Indian diets — which are predominantly plant-based — requires deliberate dietary planning.
Dietary sources of calcium in the Indian context:
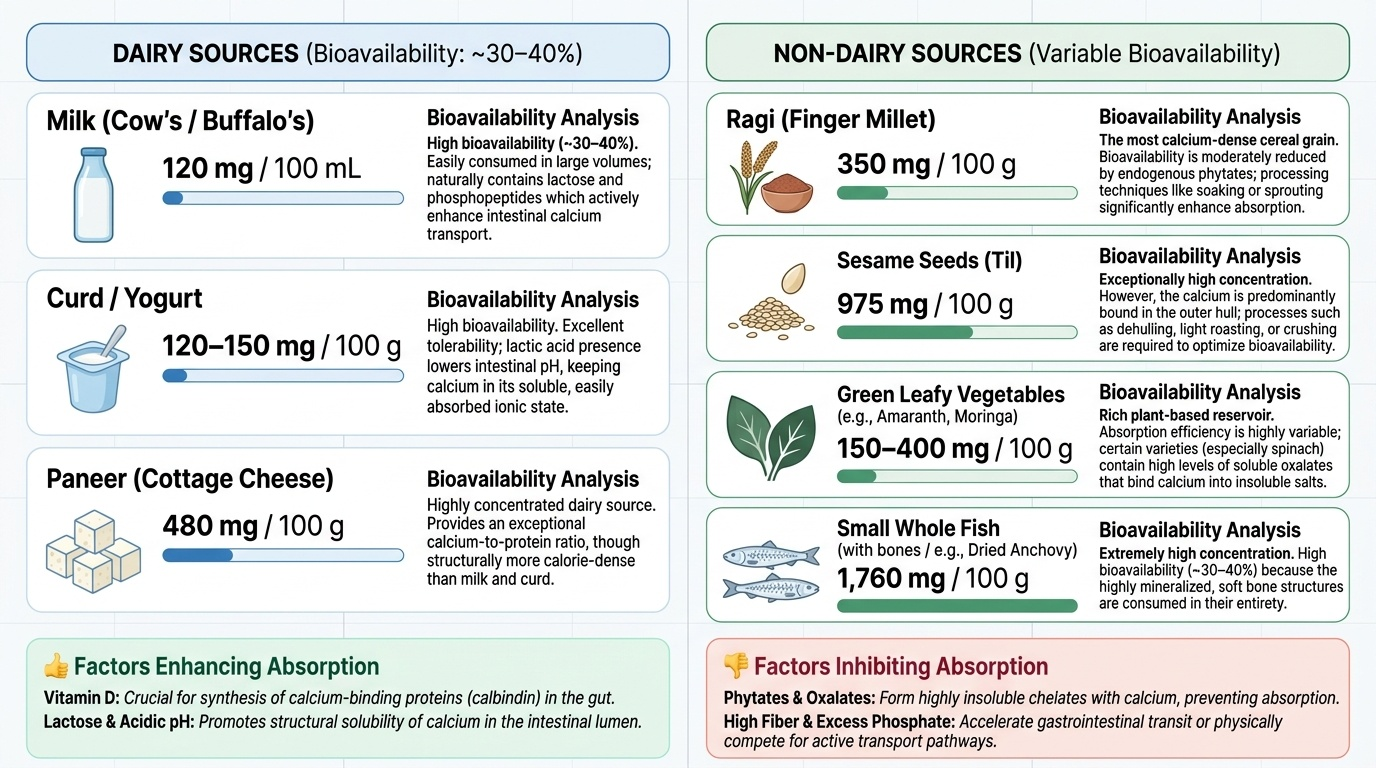
• Dairy: cow's/buffalo's milk (~120 mg/100 mL), curd/yoghurt (~120–150 mg/100 g), paneer (~480 mg/100 g) — high bioavailability (~30–40%)
• Non-dairy high-calcium foods: ragi (finger millet) (~350 mg/100 g — the most calcium-dense Indian grain), sesame seeds (~975 mg/100 g), dried beans/legumes (~100–130 mg/100 g), green leafy vegetables (amaranth, moringa), small whole fish with bones (e.g., dried anchovy ~1760 mg/100 g)
• Calcium bioavailability is reduced by: phytates (in whole grains and legumes), oxalates (in spinach, rhubarb), excessive dietary phosphate, vitamin D deficiency (the most clinically important factor), and high-fibre diets
• Calcium absorption is enhanced by: adequate vitamin D, lactose (in breast milk and cow's milk), protein
Ragi deserves special mention for Indian paediatric nutrition counselling — it is an affordable, culturally accepted, calcium-rich complementary food that can substantially improve calcium intake in toddlers who receive little or no dairy.
Magnesium: Body Distribution, RDA, and Dietary Sources
Magnesium is the fourth most abundant cation in the body and the second most abundant intracellular cation after potassium. Unlike calcium, the majority of body magnesium is intracellular: approximately 60% is in bone (as a surface mineral on hydroxyapatite crystals), 38% is intracellular (cytoplasm and mitochondria), and only about 2% is in the extracellular fluid and serum. This distribution has an important clinical implication: serum magnesium may be normal even when intracellular magnesium is significantly depleted, making biochemical assessment of total body magnesium status unreliable from serum alone. Nevertheless, the clinically used threshold is serum magnesium 1.7–2.2 mg/dL (0.7–1.0 mmol/L), and hypomagnesaemia is defined as serum Mg <1.7 mg/dL (<0.7 mmol/L).
ICMR/NIN 2020 Recommended Dietary Allowances for Magnesium:
| Age group | RDA (mg/day) | Note |
|---|---|---|
| 0–6 months | 30 (AI) | Adequate Intake from breast milk |
| 7–12 months | 75 (AI) | |
| 1–3 years | 80 | |
| 4–8 years | 130 | |
| 9–13 years | 240 | |
| 14–18 years (male) | 410 | Pubertal demand |
| 14–18 years (female) | 360 |
Dietary sources of magnesium:
Magnesium is the central atom of the chlorophyll molecule, so the richest dietary sources are invariably green leafy vegetables (spinach ~87 mg/100 g, moringa/drumstick leaves ~45 mg/100 g), nuts and seeds (pumpkin seeds ~534 mg/100 g, almonds ~270 mg/100 g), whole grains (wheat germ, brown rice ~143 mg/100 g), and legumes (black beans ~70 mg/100 g, lentils ~36 mg/100 g). Animal sources include fish (mackerel ~97 mg/100 g) and dark chocolate. Magnesium bioavailability from plant sources is approximately 30–50% and is reduced by phytates and excessive dietary calcium.
Magnesium deficiency as a pure dietary deficiency is uncommon in children on a balanced Indian diet. The clinical problem arises in settings of increased losses or impaired absorption: prolonged diarrhoea, malabsorption syndromes (e.g., Crohn's disease, coeliac disease), chronic diuretic use, and primary genetic disorders of renal magnesium reabsorption (e.g., TRPM6 gene mutations causing familial hypomagnesaemia with secondary hypocalcaemia).
SELF-CHECK
A 10-year-old boy consumes a vegetarian diet that is largely based on whole wheat chapati, dal, and vegetables. Which of the following foods, if added to his daily diet, would provide the greatest increase in calcium intake within the Indian dietary context?
A. An extra cup of green tea
B. Two tablespoons of ragi (finger millet) flour daily
C. An extra serving of white rice
D. A handful of roasted salted peanuts
Reveal Answer
Answer: B. Two tablespoons of ragi (finger millet) flour daily
Ragi (finger millet) is one of the most calcium-dense Indian grains, containing approximately 350 mg of calcium per 100 g, compared to negligible calcium in green tea, white rice, or peanuts. Ragi is an affordable, commonly available complementary food recommended by IAP for improving calcium intake in children on plant-based Indian diets. Adding 20 g of ragi flour daily provides approximately 70 mg of additional calcium — a meaningful contribution at a low cost.