Page 27 of 33
PE13.4 | Calcium Magnesium Nutrition — SDL Guide (Part 3)
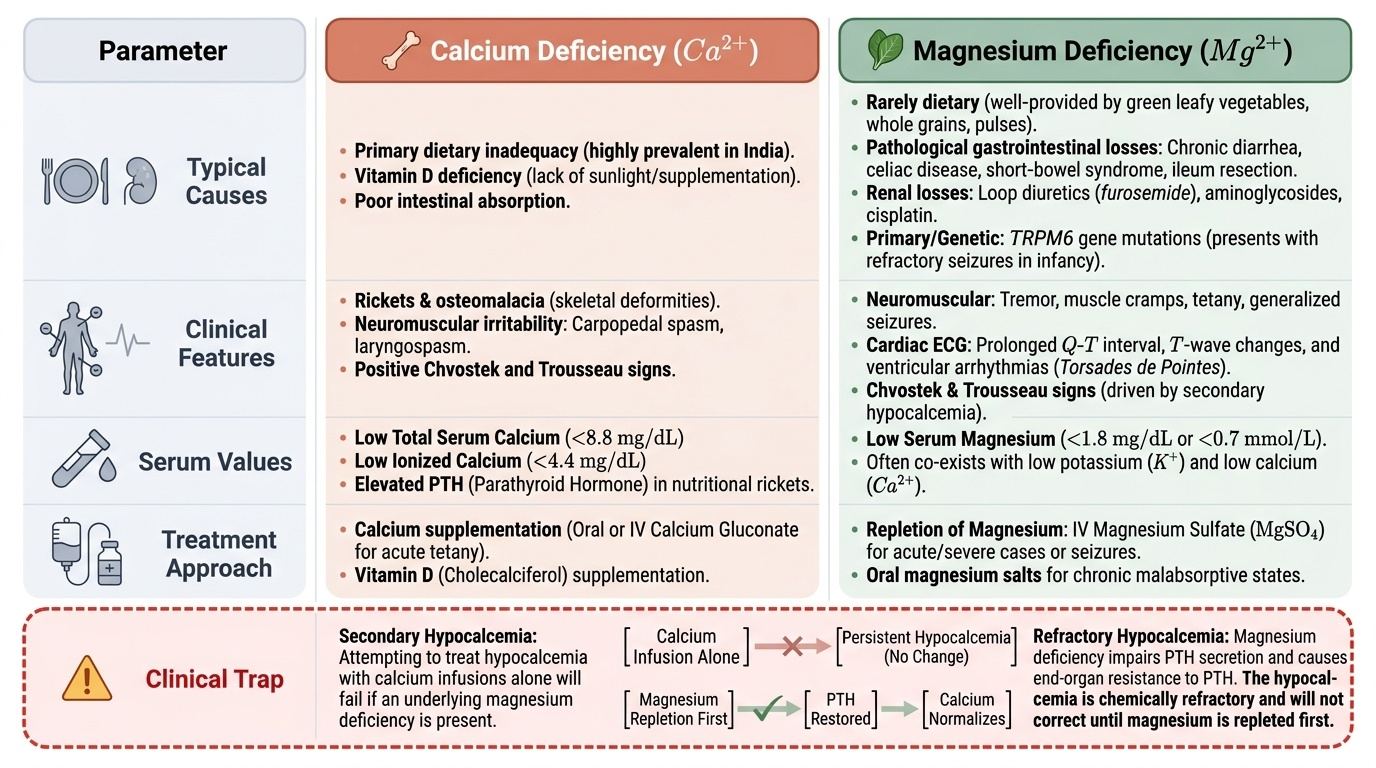
Magnesium Deficiency: Clinical Features and Management
Magnesium deficiency in children is almost always secondary to conditions that cause increased losses or impaired absorption, rather than pure dietary deficiency. Unlike calcium, whose dietary shortage in India is a well-recognised public health problem, magnesium deficiency rarely arises from inadequate dietary intake alone in a child eating a varied Indian diet — green leafy vegetables, whole grains, and pulses provide sufficient magnesium for most age groups. The clinical problem instead arises from pathological losses through the gut or kidney, or from genetic defects in magnesium transport. Recognising the clinical setting is therefore the key first step: a child with prolonged diarrhoea, short-bowel syndrome, or a cardiac patient on furosemide is at high risk of magnesium depletion and must have serum magnesium checked as a routine part of the biochemical workup, not an afterthought. The clinical consequences of magnesium depletion range from subtle neuromuscular irritability and cardiac rhythm disturbances to the cardinal and underappreciated presentation of refractory hypocalcaemia, which will not correct until magnesium is repleted. The most important causes of hypomagnesaemia in Indian paediatric practice are:
• Gastrointestinal losses: Acute and chronic diarrhoea (especially prolonged infectious gastroenteritis), malabsorption syndromes (e.g., coeliac disease, inflammatory bowel disease), short-bowel syndrome, and surgical resection of the ileum (the main site of magnesium absorption).
• Renal losses: Loop diuretics (furosemide — commonly used in paediatric cardiac and nephrotic patients), aminoglycoside antibiotics, cisplatin.
• Primary hypomagnesaemia: Rare autosomal recessive TRPM6 gene mutations (familial hypomagnesaemia with secondary hypocalcaemia) — presents in the first months of life with refractory seizures.
Provided image
The clinical features of hypomagnesaemia reflect magnesium's fundamental roles in neuromuscular transmission, cardiac rhythm, and enzymatic function:
• Neuromuscular: Tremor, muscle cramps, tetany, Trousseau and Chvostek signs (identical to hypocalcaemic tetany — because the presenting picture IS hypocalcaemic tetany driven by secondary hypomagnesaemia), generalised seizures.
• Cardiac: Prolonged QT interval and T-wave changes on ECG; ventricular arrhythmias (torsades de pointes in severe cases).
• Behavioural/psychiatric: Irritability, anxiety, depression (often under-recognised in older children and adolescents).
• Secondary metabolic: Hypokalaemia (magnesium deficiency impairs ROMK potassium channels, causing renal K+ wasting) and the cardinal presentation of refractory hypocalcaemia.
Management of hypomagnesaemia:
• Mild/asymptomatic: Oral magnesium replacement — magnesium oxide or magnesium glycinate 10–20 mg/kg/day of elemental magnesium in 2–3 divided doses. Gastrointestinal absorption limits oral dosing (diarrhoea is a dose-limiting side-effect).
• Symptomatic/severe (seizures, arrhythmia): IV magnesium sulphate 25–50 mg/kg over 30–60 minutes (maximum 2 g per dose = 4 mL of 50% MgSO4 solution or 20 mL of 10% solution); cardiac and respiratory monitoring mandatory; calcium gluconate available as antidote at the bedside.
• Ongoing prevention: Address the underlying cause (treat diarrhoea, adjust diuretic regimen, encourage magnesium-rich foods — green leafy vegetables, nuts, whole grains).
SELF-CHECK
A 5-year-old girl with short-bowel syndrome following neonatal resection has persistent hypocalcaemia (serum Ca 7.2 mg/dL) despite 48 hours of IV calcium gluconate infusion and vitamin D supplementation. Which investigation is most important to order next?
A. Serum 25-hydroxyvitamin D level
B. Intact parathyroid hormone (PTH) level
C. Serum magnesium level
D. Urine calcium:creatinine ratio
Reveal Answer
Answer: C. Serum magnesium level
In a child with short-bowel syndrome (a condition associated with magnesium malabsorption due to loss of the ileum), hypocalcaemia that is refractory to standard calcium and vitamin D replacement is the cardinal presentation of hypomagnesaemia. Hypomagnesaemia causes functional hypoparathyroidism (impaired PTH secretion and end-organ resistance) — hence the calcium will not correct until magnesium is repleted. Serum magnesium is the critical next investigation. PTH (option B) may also be low or inappropriately normal, which would confirm functional hypoparathyroidism, but knowing the magnesium level is the actionable test that directly guides management. Vitamin D (option A) and urine calcium (option D) are secondary considerations once the Mg-mediated mechanism is excluded.
Self-Assessment: Calcium and Magnesium Nutrition
Test your understanding of the calcium and magnesium nutrition content covered in this SDL with the following clinical vignettes. Review each scenario carefully before checking the explanatory notes.
Vignette 1 — The preterm neonate with jitteriness:
A 28-week preterm infant (birth weight 1100 g), now 18 hours old, is noted to have lip trembling, jitteriness, and a brief episode of apnoea. Serum calcium is reported at 5.9 mg/dL. The mother is a known diabetic on insulin.
Questions: (a) What type of neonatal hypocalcaemia is this and what are the two aetiological factors? (b) What is the immediate management? (c) What monitoring is mandatory during IV calcium infusion?
Key answers: (a) Early-onset neonatal hypocalcaemia (within 72 h). Aetiological factors: (1) prematurity — immature parathyroid response and transient hypoparathyroidism; (2) IDM (infant of diabetic mother) — maternal hyperglycaemia causes foetal hyperglycaemia and hyperinsulinism, which impairs foetal magnesium transport, leading to hypomagnesaemia that reduces PTH. (b) IV calcium gluconate 10%, 1–2 mL/kg over 5–10 minutes, followed by maintenance calcium infusion. (c) Continuous cardiac monitoring (ECG or pulse oximetry with HR display) — bradycardia, cardiac arrhythmia, and cardiac arrest can occur with rapid IV calcium.
Vignette 2 — The toddler with bowing legs:
An 18-month-old boy presents with bowing of the legs noted over 2 months. He is exclusively breastfed with no complementary food introduction. He lives in a flat with minimal sunlight exposure. On examination: frontal bossing, rachitic rosary, widened wrists. X-ray shows cupped and frayed metaphyses with widened growth plates at wrists. Serum calcium 8.2 mg/dL, phosphate 2.9 mg/dL, alkaline phosphatase 890 IU/L, PTH 280 pg/mL, 25-OH-D 8 ng/mL.
Questions: (a) What is the diagnosis and aetiology? (b) How does this differ from XLH rickets? (c) What is the IAP-recommended treatment?
Key answers: (a) Nutritional rickets — combined vitamin D deficiency (25-OH-D 8 ng/mL) and calcium deficiency (exclusively breastfed, no dairy or ragi in complementary foods; no sunlight). Secondary hyperparathyroidism confirmed (PTH 280 pg/mL). (b) In XLH rickets: serum phosphate very low (renal phosphate wasting via FGF23), serum calcium and 25-OH-D NORMAL; treatment requires oral phosphate + calcitriol, not vitamin D alone. In this case phosphate is low-normal due to PTH phosphaturia (not genetic), and 25-OH-D is grossly low. (c) Vitamin D 2000–4000 IU/day for 3 months + elemental calcium 500 mg/day + dietitian review for complementary feeding (ragi, dairy); recheck ALP and X-ray at 3 months.
Vignette 3 — Refractory hypocalcaemia with diarrhoea:
A 4-year-old girl with a 3-week history of watery diarrhoea (10–12 stools/day) is hospitalised with a generalised seizure. Serum calcium is 6.9 mg/dL. She has been receiving IV calcium gluconate for 36 hours with minimal improvement. Serum magnesium comes back at 1.0 mg/dL.
Questions: (a) Why has the calcium not corrected with IV calcium? (b) What is the treatment? (c) Name three other causes of hypomagnesaemia in children.
Key answers: (a) Hypomagnesaemia (Mg 1.0 mg/dL) causes functional hypoparathyroidism — both impaired PTH secretion (requires Mg2+ for exocytosis) AND reduced end-organ PTH responsiveness (Gs-protein GTPase requires Mg2+). Without adequate PTH activity, the renal and skeletal mechanisms to raise serum calcium cannot operate, so calcium replacement alone is ineffective. (b) IV magnesium sulphate 25–50 mg/kg over 30–60 min (max 2 g/dose), with cardiac monitoring; continue oral Mg after recovery; continue oral calcium supplementation; treat underlying diarrhoea. (c) Loop diuretics (furosemide), cisplatin chemotherapy, primary TRPM6 gene mutation (familial hypomagnesaemia with secondary hypocalcaemia).