Page 19 of 33
PE13.1-2 | Iron Nutrition — SDL Guide
Learning Objectives
- State the RDA for iron across paediatric age groups and compare haem and non-haem dietary sources with their absorption rates
- Explain the three stages of iron deficiency and the physiological mechanisms of iron absorption and regulation by hepcidin
- Describe the clinical features, diagnostic criteria (including WHO Hb cut-offs by age), and laboratory profile of iron deficiency anaemia
- State the therapeutic dose of elemental iron for IDA treatment in children
- Describe the National Iron Plus Initiative (NIPI) / Anaemia Mukt Bharat programme — target groups, IFA formulations, doses, and schedules for each age group
INSTRUCTIONS
Iron deficiency anaemia (IDA) is the single commonest nutritional deficiency disease in India and worldwide, affecting over two-thirds of children under 5 in some states. Its consequences extend far beyond pale conjunctivae — iron deficiency in infancy impairs cognitive development and motor function even before anaemia develops, with effects that may be irreversible. This module covers the full story: iron physiology and requirements, the dietary sources available in India, the progression from iron depletion to manifest IDA, the clinical and laboratory diagnosis, and the government's Anaemia Mukt Bharat programme, which you will be implementing in primary care.
References
- Ghai Essential Pediatrics, 9th ed, Ch 8 — Nutrition and Ch 16 — Blood Disorders (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 482 — Iron-Deficiency Anaemia (textbook)
- Anaemia Mukt Bharat Operational Guidelines, MoHFW, 2018 (guideline)
- WHO Haemoglobin Concentrations for the Diagnosis of Anaemia, 2011 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a rural sub-centre, an Anganwadi worker brings a 3-year-old girl for review because she has been 'weak' for several months. The child is irritable, tires easily, and her mother says she eats poorly — she craves clay and paper (pica). On examination, the child is pale, with pallor of the conjunctivae, tongue, and nail beds. Her spleen is just palpable. Her haemoglobin is 7.2 g/dL. The diet history reveals the family is vegetarian, subsisting on roti, dal, and rice; they rarely eat green leafy vegetables. The Anganwadi worker asks you which government programme provides iron supplementation to children like this, and what dose she should have been receiving. How do you answer — and what treatment do you start today?
WHY THIS MATTERS
Iron deficiency anaemia is the most prevalent nutritional disorder in India. NFHS-5 (2019–21) reported that approximately 67% of children aged 6–59 months in India are anaemic, with some states exceeding 80%. The consequences of IDA in children are not limited to pallor and fatigue — iron is essential for myelination, neurotransmitter synthesis (dopamine, serotonin), and mitochondrial function in the developing brain. Iron deficiency, even in its pre-anaemic stage, causes measurable cognitive impairment, reduced attention span, and poor school performance. Some of these effects on brain development during the critical window of the first two years of life may not be fully reversible even after iron repletion. As a doctor in any clinical setting — primary care, community health, or hospital — you will encounter IDA more frequently than almost any other paediatric condition. Knowing the diagnostic criteria, the correct therapeutic dose, and the government programme doses exactly is non-negotiable.
RECALL
Before you proceed, recall:
• Haemoglobin is the oxygen-carrying protein in red blood cells, containing four haem groups each with one Fe²⁺ ion; iron is essential for haem synthesis in erythroblasts.
• Ferritin is the primary intracellular iron storage protein; serum ferritin reflects total body iron stores (low ferritin = depleted stores).
• Non-haem iron absorption requires reduction of Fe³⁺ to Fe²⁺ by gastric acid and vitamin C, followed by transport across the enterocyte brush border by DMT1 (divalent metal transporter 1), and export into the portal circulation via ferroportin.
• Mean corpuscular volume (MCV): normal >80 fL; iron deficiency causes microcytic (MCV <80 fL), hypochromic (MCH <27 pg) anaemia.
• Pica (craving for non-food substances — clay, paper, ice) is a well-known symptom of iron deficiency whose mechanism is not fully understood but is clinically useful as a diagnostic clue.
Iron in Paediatric Health: Why It Matters
Iron deficiency anaemia (IDA) is the commonest nutritional anaemia worldwide and the leading cause of years lived with disability among all nutritional deficiencies globally. In India, it constitutes a major public health burden: NFHS-5 data (2019–21) showed that 67.1% of children aged 6–59 months were anaemic — a figure that represents millions of children at risk of impaired cognitive development, reduced immune function, and poor growth. The states of Uttar Pradesh, Bihar, Madhya Pradesh, and West Bengal carry disproportionately high burdens. The impact of iron deficiency in infancy and early childhood extends well beyond anaemia: iron is required for synthesis of myelin in the developing brain, for the production of dopaminergic neurotransmitters, and for oxidative phosphorylation in neurons. Studies consistently show that children with iron deficiency in early life have lower IQ scores, reduced attention, and poorer academic outcomes — some of which persist even after iron repletion if the deficiency occurred during the critical window of brain myelination (first 2 years). Understanding the magnitude and consequences of iron deficiency is the foundation for appreciating why India has invested significantly in programmatic iron supplementation through the National Iron Plus Initiative and Anaemia Mukt Bharat.
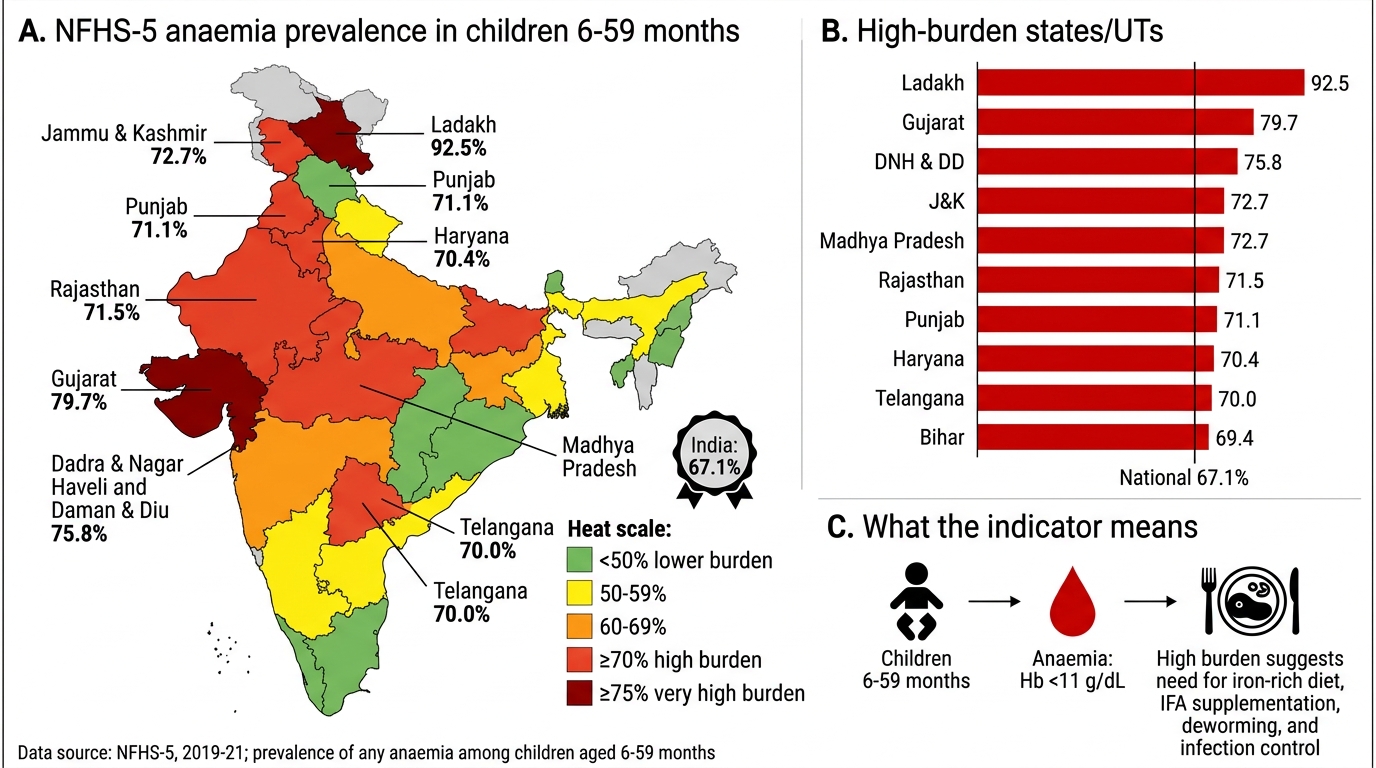
NFHS-5 Childhood Anaemia Burden Across India
Iron Physiology: RDA, Dietary Sources, and Absorption
The body contains approximately 3–5 g of iron in an adult, of which 60–70% is in haemoglobin, 10% in myoglobin and enzymes, and the remainder in storage forms (ferritin and haemosiderin). Daily losses are small (approximately 1 mg/day for children through intestinal epithelial shedding, sweat, and trace blood losses), but absorption must compensate for these losses while also supporting growth and increasing red-cell mass. The Indian RDA for iron (ICMR/NIN 2020) is 9 mg/day for children aged 1–3 years, 13 mg/day for 4–6 years, and 16 mg/day for 7–9 years; adolescent boys require 20 mg/day and adolescent girls 27 mg/day (higher demand due to menstrual losses).
Dietary iron exists in two forms with fundamentally different bioavailability:
Haem iron is found in animal-source foods — red meat, poultry, and fish. It is absorbed as an intact metalloporphyrin complex directly by haem carrier protein 1 (HCP-1) on enterocyte brush borders, with bioavailability of approximately 20–25%, and its absorption is not inhibited by dietary factors such as phytates, oxalates, or calcium. Haem iron is the most efficiently absorbed dietary iron form.
Non-haem iron is found in plant foods (legumes, cereals, green leafy vegetables) and fortified foods. It exists as Fe³⁺ and must be reduced to Fe²⁺ before absorption; this reduction is facilitated by gastric acid and dietary vitamin C (ascorbate), explaining why vitamin C dramatically enhances non-haem iron absorption. Fe²⁺ is transported across the enterocyte brush border by divalent metal transporter 1 (DMT1). Bioavailability is only 1–10% and is markedly inhibited by phytates (in cereals and legumes), tannins (tea, coffee), calcium (dairy), and oxalates (spinach). In contrast, vitamin C, animal protein, and fermented foods (which reduce phytate content) enhance absorption. Given that the majority of Indian children's diets are vegetarian and cereal-based, the bioavailability of their dietary iron is inherently low — making the gap between RDA and actual absorbed iron particularly large. Within the enterocyte, iron is either stored as ferritin or exported to the portal circulation via ferroportin, regulated by the liver-derived peptide hepcidin; in iron deficiency, hepcidin is suppressed, allowing maximum ferroportin expression and enhanced intestinal iron export.
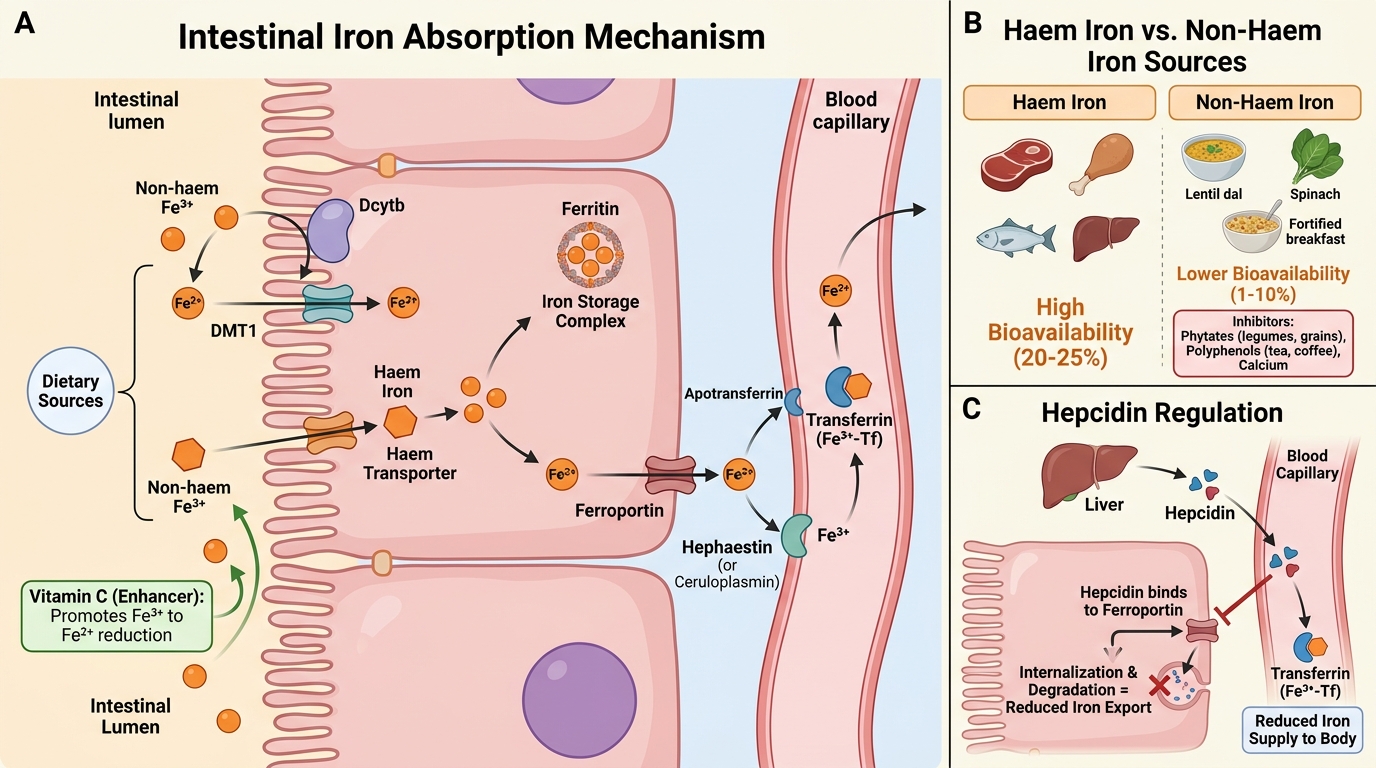
Iron Absorption in the Duodenal Enterocyte
| Source type | Examples | Bioavailability | Key factors |
|---|---|---|---|
| Haem iron | Meat, poultry, fish, liver | ~20–25% | Not inhibited by dietary factors |
| Non-haem iron | Dal, green leafy veg, fortified cereals | 1–10% | Enhanced by vitamin C; inhibited by phytate, tannin, calcium |
SELF-CHECK
A 2-year-old child is on a purely vegetarian diet with no animal-source foods. Which intervention would most effectively enhance absorption of dietary non-haem iron?
A. Adding calcium-fortified milk to the diet
B. Giving the iron-containing meal with a cup of tea
C. Including a guava or citrus fruit alongside the iron-containing meal
D. Soaking the lentils overnight and discarding the water before cooking
Reveal Answer
Answer: C. Including a guava or citrus fruit alongside the iron-containing meal
Vitamin C (ascorbic acid) is the most potent enhancer of non-haem iron absorption — 50 mg of vitamin C can increase non-haem iron absorption by 2–4 fold by reducing Fe³⁺ to Fe²⁺ in the gut lumen. Guava and citrus are among the most vitamin C-rich accessible foods. Calcium in milk INHIBITS non-haem iron absorption. Tea contains tannins that also INHIBIT absorption. Soaking lentils and discarding the water reduces phytate content and is a useful strategy but is less potent than vitamin C co-ingestion as an absorption enhancer.
Iron Deficiency: How It Develops and Progresses
Iron deficiency does not develop suddenly — it progresses through three sequential stages, each with a distinct biochemical and clinical profile. Understanding this progression explains why serum ferritin can be abnormal long before the child appears pale, and why the cognitive effects of iron deficiency may precede the development of anaemia that triggers clinical suspicion.
Stage 1 — Pre-latent (Iron Depletion): Iron stores are depleted but haemoglobin and serum iron remain normal. The only abnormality is a low serum ferritin (<12 mcg/L; or <30 mcg/L in the context of inflammation). There are no symptoms; this stage is detectable only on screening. The child may already be experiencing subclinical effects on brain iron-dependent enzymes.
Stage 2 — Latent Iron Deficiency: Stores are exhausted; iron supply to erythropoiesis is now insufficient. Serum iron falls, total iron-binding capacity (TIBC) rises (as the liver synthesises more transferrin), and transferrin saturation falls below 15%. Haemoglobin is still normal or at the lower limit; MCV may begin to fall. The child may show early fatigue and reduced attention.
Stage 3 — Manifest IDA: Iron supply for erythropoiesis is critically insufficient; haemoglobin falls below the WHO cut-off for age. Red cells become microcytic (MCV <80 fL) and hypochromic (pale centre exceeds one-third the diameter; MCH <27 pg). The child now presents with pallor, fatigue, irritability, pica, and, in severe cases, cardiac symptoms.
Risk groups for iron deficiency in children:
• Infants born preterm or with low birth weight (smaller iron stores at birth)
• Infants exclusively breastfed beyond 6 months without iron-containing complementary foods (breast milk iron, while bioavailable, is insufficient beyond 4–6 months)
• Infants on unmodified cow's milk as the primary beverage (poor iron content, may cause occult GI blood loss)
• Children on vegetarian/vegan diets with high phytate intake
• Children with chronic blood loss (hookworm, chronic gastritis, inflammatory bowel disease)
• Adolescent girls with onset of menstruation
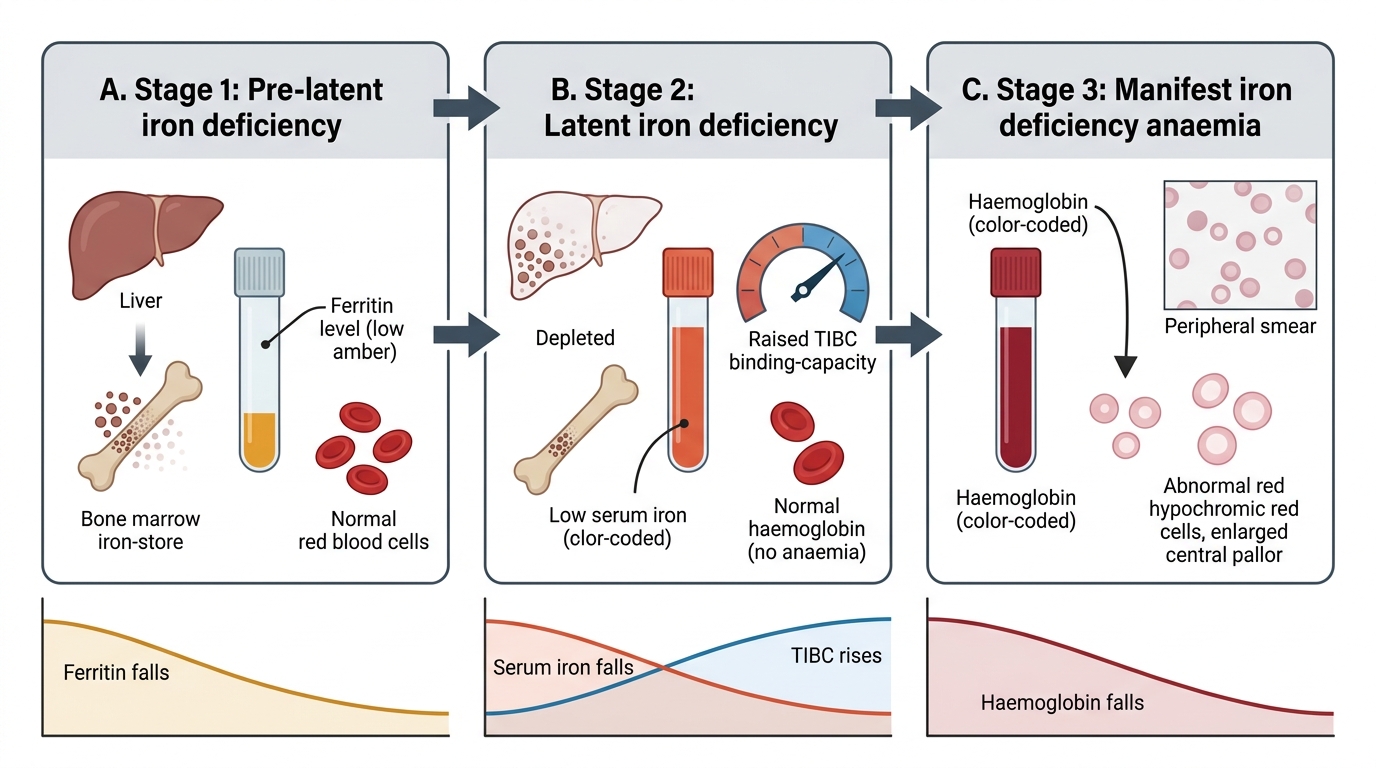
Stages of Iron Deficiency