Page 2 of 33
PE12.1-2 | Vitamin A — SDL Guide (Part 2)
Clinical Features and Classification of Vitamin A Deficiency
The clinical spectrum of Vitamin A deficiency is systematically classified by the WHO using the xerophthalmia classification, which grades ocular and systemic manifestations from mildest to most severe. This grading system is clinically important because stages X1A (Bitot's spots) through X3B (keratomalacia) are used to define Vitamin A deficiency as a significant public health problem in a community. The classification has both ocular and non-ocular components.
Provided image
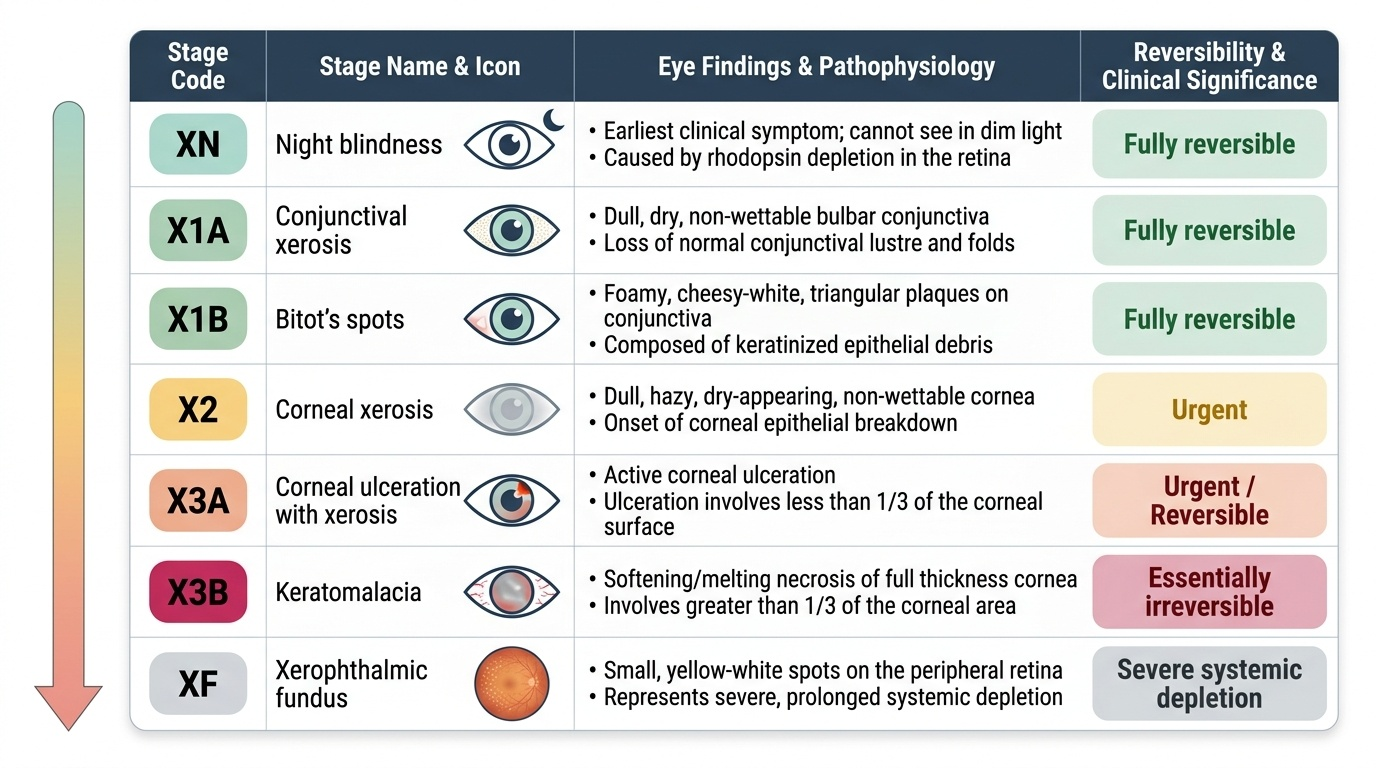
WHO Xerophthalmia Classification:
XN — Night blindness (nyctalopia): earliest symptom; child cannot see in dim light or at dusk; rhodopsin depletion; fully reversible. In young children this is often reported by parents as the child becoming 'hesitant' or 'clumsy' at dusk.
X1A — Conjunctival xerosis: dull, dry, non-wettable bulbar conjunctiva; the normal conjunctival lustre and folds are lost; the surface looks like dry sand.
X1B — Bitot's spots: foamy, cheesy-white, triangular plaques on the bulbar conjunctiva (typically bilateral, temporal > nasal); composed of keratinised epithelial debris and Corynebacterium xerosis; pathognomonic of Vitamin A deficiency in children; reversible with treatment.
X2 — Corneal xerosis: dull, hazy, dry-appearing cornea; non-wettable; epithelial breakdown beginning; prompt treatment prevents progression.
X3A — Corneal ulceration with xerosis: ulceration involving less than one-third of the corneal area; still potentially reversible with aggressive treatment.
X3B — Keratomalacia: colliquative (softening/melting) necrosis of the full thickness of the cornea; greater than one-third corneal involvement; essentially irreversible; leads to perforation, phthisis bulbi, and permanent blindness.
XF — Xerophthalmic fundus: yellow-white spots on the peripheral retina; represents severe systemic depletion; rare.
XN — Night blindness in older children and adults (sometimes listed separately as XN to distinguish from the childhood classification).
Systemic features of Vitamin A deficiency (beyond the eye):
• Skin: follicular hyperkeratosis (phrynoderma) — 'toad skin'; dry, rough, horny papules over the lateral upper arms, thighs, and shoulders
• Growth: poor linear growth and weight gain
• Immunity: increased frequency and severity of respiratory infections, diarrhoeal disease, measles
• Anaemia: Vitamin A deficiency impairs erythropoiesis and iron mobilisation, contributing to anaemia of nutritional deficiency
CLINICAL PEARL
Bitot's spots are pathognomonic of Vitamin A deficiency in children under 6 years, but NOT in older children and adults. In adults, Bitot's spots may be a residual inactive lesion from past deficiency and do not necessarily indicate active, current deficiency — they can persist even after repletion. Night blindness (XN) is the better indicator of active deficiency in this age group. Always ask parents of pre-school children about difficulty seeing at dusk — the history of nyctalopia often precedes visible Bitot's spots by weeks.
Diagnosis and Management of Vitamin A Deficiency
The diagnosis of Vitamin A deficiency is primarily clinical, based on the xerophthalmia classification and the history of dietary inadequacy in an at-risk child. In the community and clinical setting, the history of night blindness in a child from a nutritionally vulnerable household — combined with conjunctival findings such as Bitot's spots — provides sufficient grounds to initiate treatment without waiting for laboratory confirmation. Biochemical testing is rarely required for individual management decisions in the field, but it plays an important role in population surveys, where biochemical prevalence data guide national programme responses. When biochemical confirmation is needed, serum retinol is the most commonly used marker, with a value below 0.70 µmol/L (20 µg/dL) indicating deficiency at the population level per WHO criteria.
Biochemical markers:
• Serum retinol <0.70 µmol/L (20 µg/dL) = deficiency (WHO threshold for population-level significance); <0.35 µmol/L = severe deficiency
• Relative dose-response (RDR) test: measures the percentage rise in serum retinol 5 hours after a test dose (positive = liver stores depleted)
• Conjunctival impression cytology (CIC): demonstrates metaplastic cells on the conjunctiva before clinical signs appear
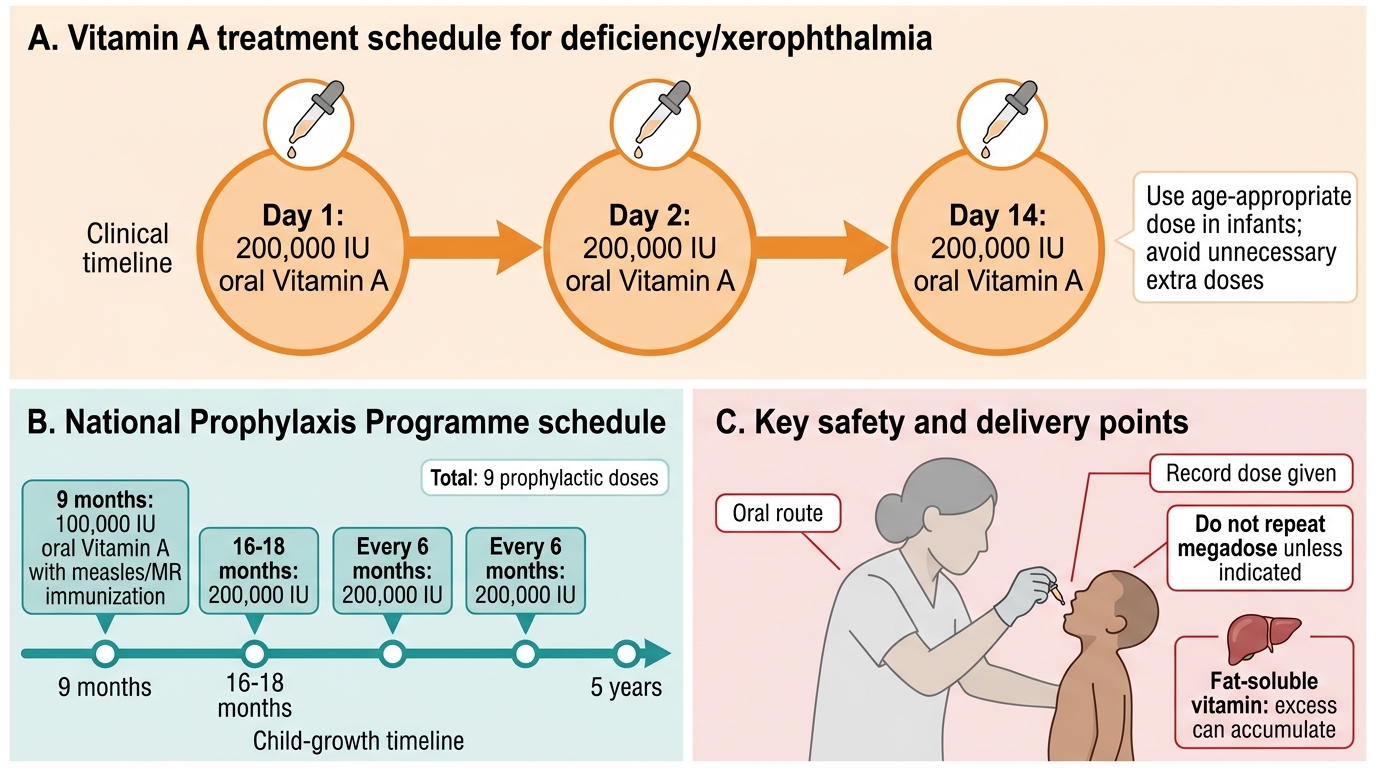
Treatment of established deficiency (WHO/IAP recommended schedule):
The cornerstone of treatment is oral megadose Vitamin A supplementation given on a three-dose schedule:
| Day | Dose (children ≥12 months) | Dose (infants 6–12 months) |
|---|---|---|
| Day 1 (immediately) | 200,000 IU (2 lakh IU) oral | 100,000 IU oral |
| Day 2 | 200,000 IU oral | 100,000 IU oral |
| Day 14 | 200,000 IU oral | 100,000 IU oral |
For infants <6 months: 50,000 IU on each of the three occasions. The rationale for the three-dose regimen is: Day 1 reverses acute deficiency and restores vision; Day 2 ensures saturation of hepatic stores; Day 14 consolidates repletion after early gastrointestinal losses.
National Vitamin A Supplementation (Prophylaxis) Programme — India:
India's programme delivers Vitamin A via the immunisation platform at the following schedule:
| Age / Contact point | Dose | Form |
|---|---|---|
| 9 months (with MR/Measles vaccine) | 1,00,000 IU (1 lakh IU) | Oral solution |
| 16 months (DPT/OPV booster-1) | 2,00,000 IU (2 lakh IU) | Oral solution |
| 2 years, 2.5 years, 3 years … up to 5 years (6-monthly) | 2,00,000 IU (2 lakh IU) | Oral solution |
Key programme point: the 9-month dose is 1 lakh IU (not 2 lakh), reflecting the smaller hepatic storage capacity of a younger infant; from 18 months onwards, the full 2 lakh IU every 6 months is used.
Dietary counselling: counsel caregivers to include dark-green leafy vegetables, orange-yellow fruits, and eggs in the child's diet daily; promote continued breastfeeding.
Vitamin A Treatment and Prophylaxis Schedule
Vitamin A Toxicity (Hypervitaminosis A)
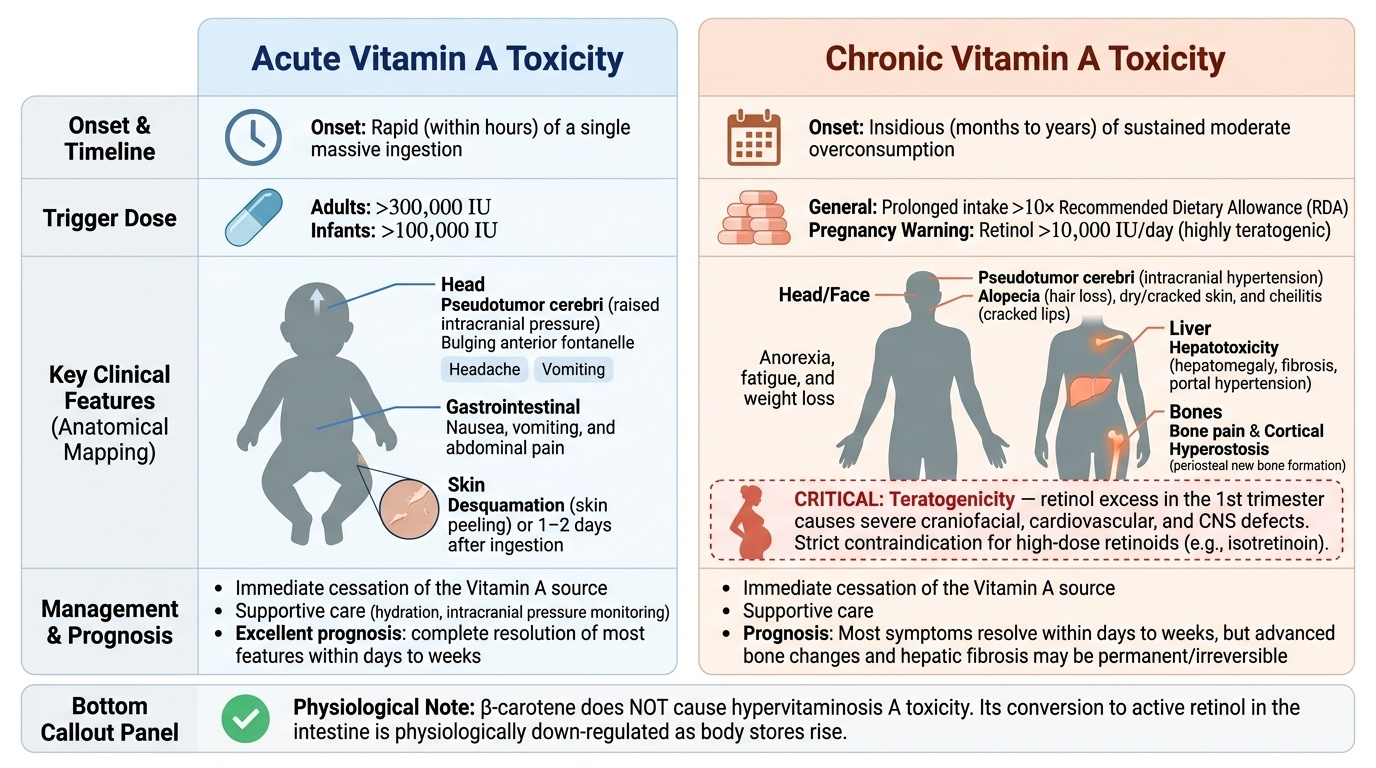
Vitamin A toxicity (hypervitaminosis A) results from excessive intake and is an important clinical consideration, particularly because megadose supplementation programmes are widely deployed and parents sometimes self-administer additional doses believing 'more is better.' Unlike water-soluble vitamins, which are readily excreted in urine, fat-soluble Vitamin A accumulates in hepatic stellate cells and adipose tissue, and the body has limited capacity to rapidly excrete an excess load. This accumulation means that toxicity can arise from both a single massively excessive dose (acute toxicity) and from prolonged moderate overconsumption over months or years (chronic toxicity). Understanding the clinical distinction between these two forms, and their management, is essential for safe delivery of Vitamin A programmes.
Provided image
Acute toxicity occurs within hours of a massively excessive single dose (typically >300,000 IU in adults or >100,000 IU in infants). Clinical features include:
• Raised intracranial pressure (pseudotumour cerebri): bulging fontanelle in infants (most characteristic in the paediatric context), headache, vomiting
• Nausea, vomiting, abdominal pain
• Skin peeling (desquamation) appearing 1–2 days after the acute episode
Chronic toxicity develops insidiously after months to years of excessive intake (>10 times the RDA). Features include:
• Anorexia, weight loss, fatigue
• Bone pain and cortical hyperostosis (periosteal new bone formation detectable on X-ray, particularly of the long bones and clavicles)
• Dry, rough, cracked skin; hair loss (alopecia); cheilitis
• Hepatotoxicity: hepatomegaly, fibrosis, portal hypertension in severe chronic excess
• Pseudotumour cerebri (intracranial hypertension)
• Teratogenicity — critically important: excess Vitamin A (retinol > 10,000 IU/day) in the first trimester is teratogenic, causing craniofacial, cardiovascular, and CNS defects. This is why high-dose retinoid drugs (isotretinoin for acne) carry a strict pregnancy contraindication. Note: β-carotene does NOT cause toxicity because conversion to retinol is down-regulated as body stores rise.
Management of toxicity:
• Immediate cessation of the Vitamin A source
• Supportive care; resolution of most features (except bone and hepatic changes) occurs within days to weeks of stopping supplementation
• For intracranial hypertension: acetazolamide to reduce CSF pressure if needed
Important distinction: the bulging fontanelle after a prophylaxis dose (from the dose given at 9 months) is an acute toxicity feature that resolves without specific treatment — parents should be counselled about this possibility when the dose is given.
SELF-CHECK
An 8-month-old infant is brought to the emergency department 6 hours after a health worker administered a Vitamin A capsule during an immunisation visit. The infant has a tense, bulging anterior fontanelle and is irritable but afebrile. There is no history of fever or head injury. What is the most likely cause, and what is the first-line management?
A. Acute Vitamin A toxicity causing raised intracranial pressure; stop source, reassure parents, observe (self-limiting)
B. Bacterial meningitis; urgent lumbar puncture and empirical antibiotics
C. Subdural haematoma from non-accidental injury; urgent CT scan
D. Hydrocephalus due to congenital aqueductal stenosis; neurosurgical referral
Reveal Answer
Answer: A. Acute Vitamin A toxicity causing raised intracranial pressure; stop source, reassure parents, observe (self-limiting)
A bulging fontanelle appearing hours after a high-dose Vitamin A administration is the characteristic presentation of acute Vitamin A toxicity (pseudotumour cerebri). The infant is afebrile, ruling against meningitis as the primary concern. The fontanelle change is due to raised intracranial pressure from excess retinol, which is self-limiting once the dose is metabolised. Management is primarily reassurance and observation. Meningitis, haematoma, and hydrocephalus require specific investigations but are not supported by the acute temporal link to Vitamin A dosing.
Self-Assessment and Case Application
Let us return to the case in the opening hook. The 2-year-old boy from Rajasthan has classic Bitot's spots (WHO stage X1A) and a history consistent with night blindness (XN) — bumping into objects at dusk. His immunisation record indicates he received the 9-month MR vaccine, at which point a dose of 1 lakh IU (100,000 IU) of Vitamin A should also have been administered. It was not — a missed opportunity at a critical immunisation contact.
Immediate management: Administer 200,000 IU of Vitamin A orally today (Day 1), repeat tomorrow (Day 2), and again at Day 14. Simultaneously address his dietary history with family counselling on locally available, affordable Vitamin A-rich foods (drumstick leaves, methi, eggs if affordable, papaya, ripe mango).
Prognosis: Bitot's spots and night blindness (stages XN, X1A, X1B) are fully reversible with prompt treatment. Corneal involvement (X2, X3A) may be partially reversible; keratomalacia (X3B) results in permanent blindness. This underscores the urgency of recognising pre-corneal stages.
Programmatic lesson: The health worker missed the opportunity to give Vitamin A at the 9-month visit. The programme now delivers:
• 1 lakh IU at 9 months (with MR/measles)
• 2 lakh IU every 6 months from 16–18 months to 5 years
Key recall points for examination:
• Night blindness is the earliest symptom of Vitamin A deficiency (XN)
• Bitot's spots (X1A) = pathognomonic in children <6 years, not in adults
• Treatment: 200,000 IU on Day 1, Day 2, Day 14
• Prophylaxis programme: 1 lakh IU at 9 months; 2 lakh IU 6-monthly from 18 months to 5 years
• β-carotene does NOT cause toxicity; excess preformed retinol does
• Acute toxicity: bulging fontanelle in infants; teratogenic in first trimester
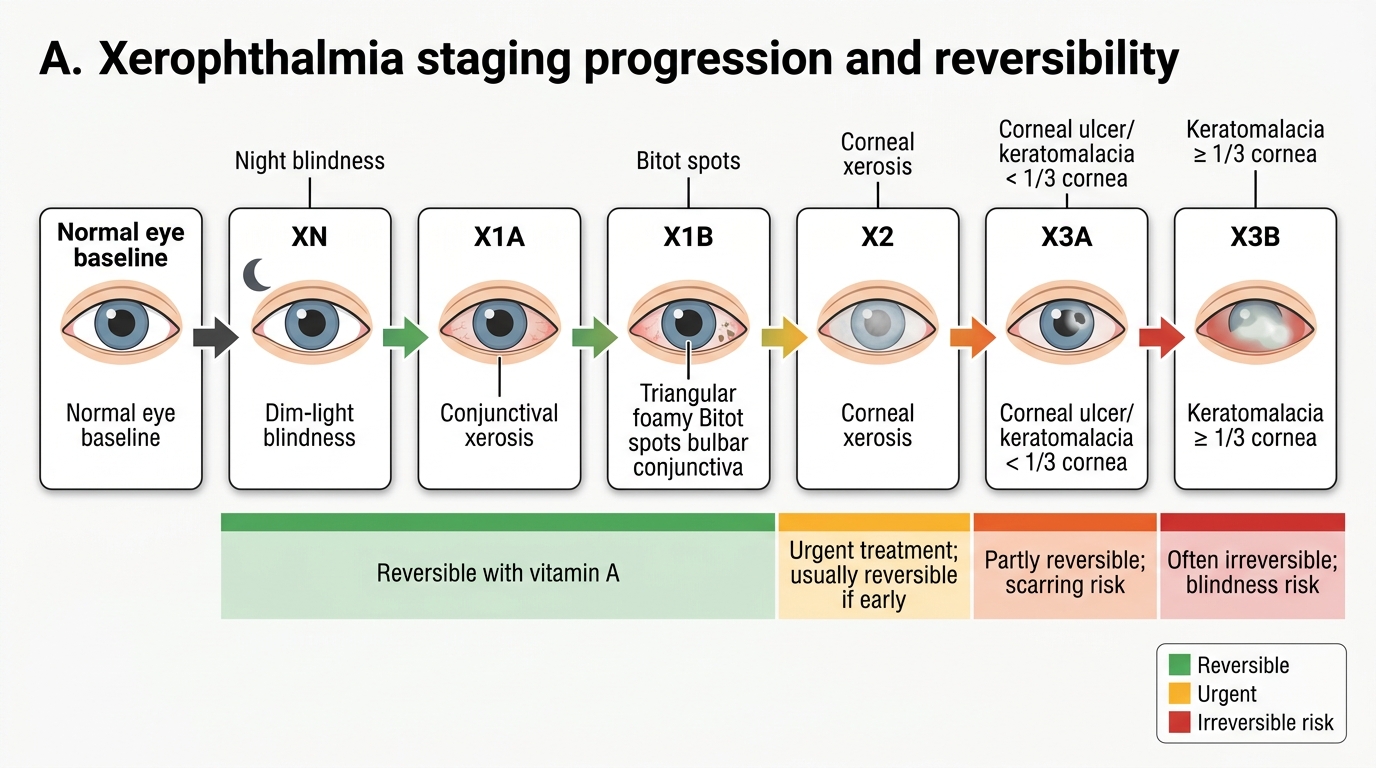
Xerophthalmia Staging and Reversibility