Page 11 of 33
PE12.5-6 | Vitamin K — SDL Guide (Part 2)
Vitamin K Deficiency Bleeding (VKDB): Classification and Clinical Features
VKDB — previously called Haemorrhagic Disease of the Newborn (HDN) — is classified into three clinical forms based on the timing of presentation, which reflects different causative mechanisms and identifies different at-risk infant populations. This classification is clinically important because the form dictates both the urgency and the preventive strategy. The shift in nomenclature from HDN to VKDB reflects a better mechanistic understanding — the condition is not restricted to the neonatal period (late VKDB occurs up to 6 months), and the term HDN was sometimes confused with other haemorrhagic disorders of neonates. Understanding the timing of each form allows the clinician to immediately generate the correct hypothesis when a bleeding infant presents: a birth-day bleed prompts a question about maternal drug exposure; a day-3 bleed raises the question of missed prophylaxis; and a bleed at 3 weeks of age in a breastfed infant without prophylaxis is late VKDB until proven otherwise — a medical emergency.
Provided image
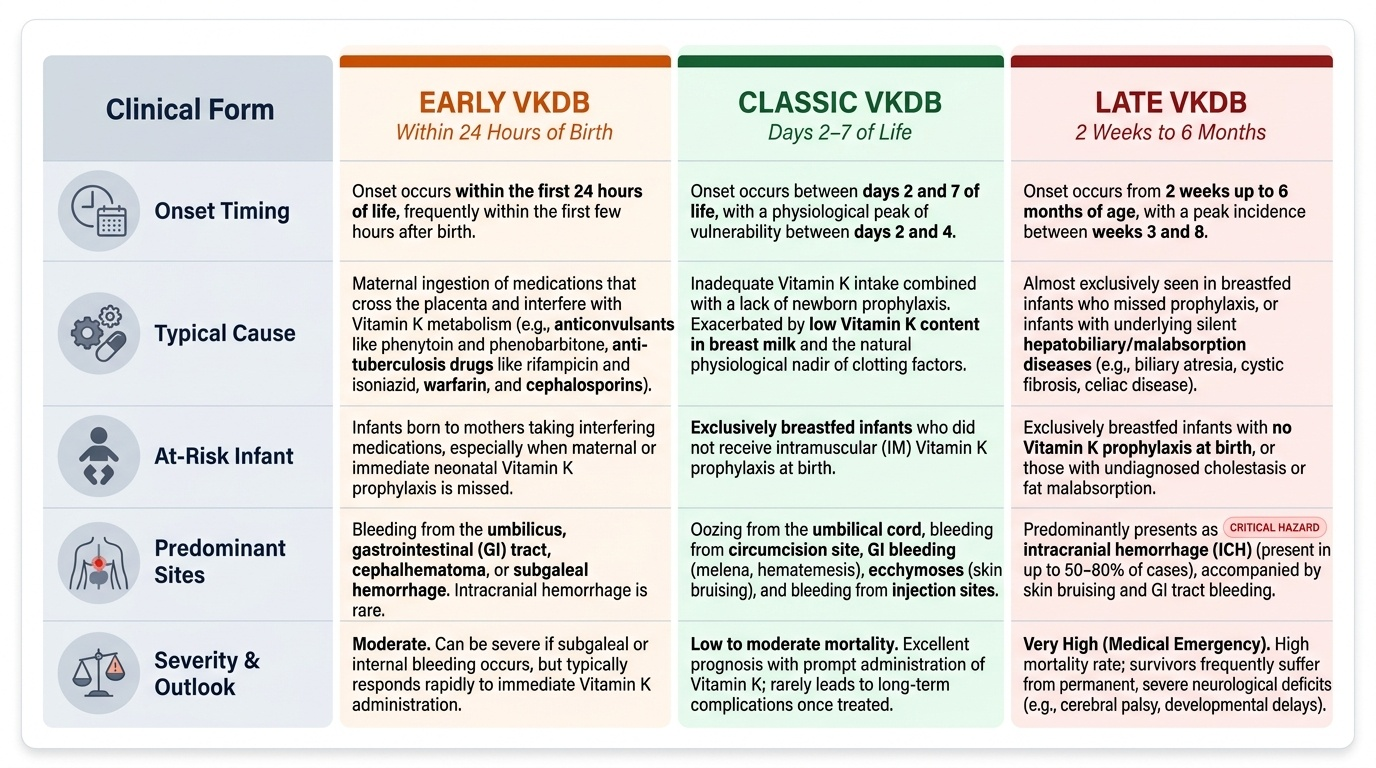
Classification of VKDB:
EARLY VKDB (within the first 24 hours of life):
• Timing: onset within 24 hours of birth
• Cause: maternal ingestion of drugs that cross the placenta and interfere with Vitamin K metabolism — anticonvulsants (phenobarbitone, phenytoin), anti-tuberculosis drugs (rifampicin, isoniazid), anticoagulants (warfarin), cephalosporins (broad-spectrum, inhibit K2 synthesis)
• Clinical features: bleeding from umbilicus, gastrointestinal tract, cephalhaematoma, subgaleal haemorrhage, intracranial haemorrhage (rare)
• Prevention: Vitamin K given to the mother during the last month of pregnancy AND to the neonate at birth
CLASSIC VKDB (day 2–7 of life):
• Timing: days 2–7 (peak days 2–4)
• Cause: inadequate Vitamin K intake (exclusively breastfed, low breast milk K content) combined with no prophylaxis at birth; normal physiological nadir of Vitamin K-dependent factors
• At-risk infant: exclusively breastfed, no IM Vitamin K at birth
• Clinical features: umbilical cord oozing, bleeding from circumcision site, gastrointestinal bleeding (malaena, haematemesis), ecchymoses, bleeding from injection sites
• Prevention: routine IM Vitamin K 1 mg at birth
LATE VKDB (2 weeks to 6 months of age):
• Timing: 2 weeks to 6 months (peak 3–8 weeks)
• Cause: exclusive breastfeeding without prophylaxis, OR fat malabsorption (cholestatic liver disease, cystic fibrosis, alpha-1-antitrypsin deficiency, biliary atresia)
• At-risk infant: exclusively breastfed without birth prophylaxis; infants with undiagnosed cholestasis
• Clinical features: most dangerous form — intracranial haemorrhage (ICH) in 30–50% of cases; subdural, subarachnoid, or intracerebral haemorrhage causing sudden deterioration, vomiting, tense fontanelle, seizures, apnoea; other bleeding sites (skin, gastrointestinal)
• Prognosis: 20% mortality; 30–50% permanent neurological sequelae (hemiplegia, developmental delay, visual impairment)
• Prevention: routine IM Vitamin K at birth is the only reliable prevention; cholestasis identified early requires ongoing fat-soluble vitamin supplementation
Diagnosis, Management and Prevention of VKDB
The diagnosis of VKDB combines the clinical context (breastfed newborn, no birth prophylaxis, relevant drug exposure, underlying malabsorption) with a characteristic coagulation profile. Prompt recognition and immediate treatment are essential to prevent catastrophic bleeding, particularly intracranial haemorrhage in late VKDB. The key diagnostic principle is that VKDB is a disorder of secondary haemostasis — coagulation factor deficiency — with entirely intact primary haemostasis (platelets and vessel-wall response). This distinction immediately separates VKDB from immune thrombocytopenia (ITP), neonatal alloimmune thrombocytopenia, and disseminated intravascular coagulation (DIC, which typically has both low platelets AND prolonged PT/aPTT). The combination of prolonged PT AND prolonged aPTT with normal platelet count and normal bleeding time is pathognomonic of a factor-deficiency coagulopathy, and in the appropriate clinical context is sufficient to initiate Vitamin K treatment without delay.
Diagnostic investigations:
• Prothrombin time (PT): markedly prolonged — this is the most sensitive test for VKDB because Factor VII (extrinsic pathway, shortest half-life) is depleted early
• Activated partial thromboplastin time (aPTT): also prolonged (Factors IX, X, II depleted)
• Platelet count: NORMAL — distinguishes from thrombocytopenia
• Bleeding time: NORMAL — primary haemostasis intact
• PIVKA-II (des-gamma-carboxyprothrombin): elevated — most specific marker of subclinical Vitamin K deficiency; not routinely available
• Response to Vitamin K (the 'Koller test' equivalent): normalisation of PT within 4–6 hours of Vitamin K administration confirms VKDB
Management:
| Situation | Vitamin K | FFP | Other |
|---|---|---|---|
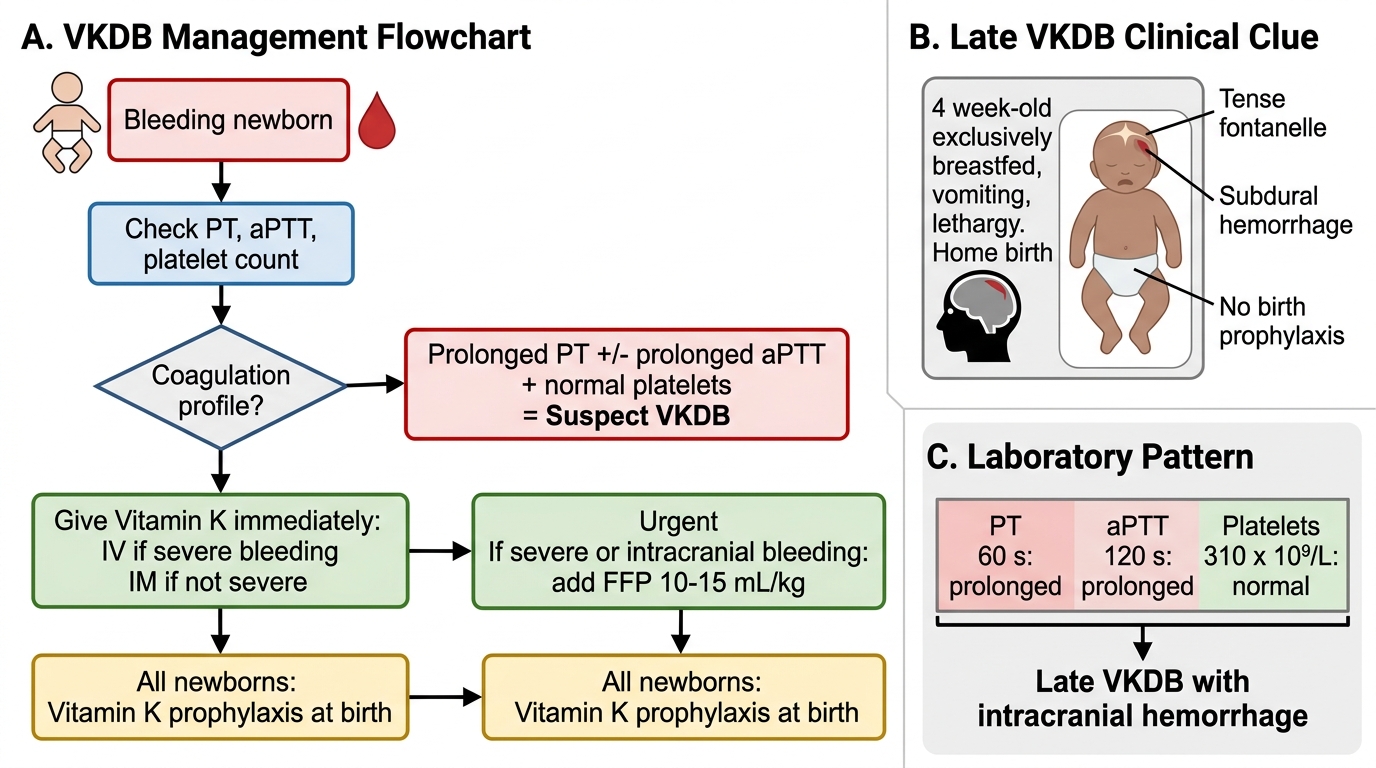
| Suspected VKDB (active bleeding) | 1 mg IV immediately (or IM if IV unavailable) | 10–15 mL/kg IV (provides immediate factor replacement) | Identify source of bleeding; neuroimaging if ICH suspected |
| Suspected VKDB (no active bleeding) | 1 mg IM | Not required | Monitor PT at 4–6 hours |
| VKDB secondary to malabsorption | 1 mg IM/IV + address underlying cause | As needed | Consider ongoing supplementation |
Key management point: Vitamin K takes 4–6 hours to correct PT (liver needs time to synthesise new carboxylated factors after Vitamin K is administered). For severe, life-threatening bleeding (intracranial haemorrhage), FFP provides immediate coagulation factors and should be given concurrently with Vitamin K.
Prevention — National Vitamin K Prophylaxis Protocol (IAP/NIS):
This is the most important programmatic intervention:
• All newborns (term and preterm) should receive Vitamin K prophylaxis at birth, regardless of mode of delivery or feeding intention
• Dose: 1 mg IM for newborns ≥2.5 kg (or ≥35 weeks gestation)
• Dose: 0.5 mg IM for newborns <2.5 kg (or <35 weeks gestation)
• Route: intramuscular is preferred over oral because IM provides reliable, single-dose long-term protection; oral regimens require multiple doses (3–4 doses over weeks) and have lower bioavailability
• Timing: within the first few hours after birth
Newborn VKDB: Diagnosis, Emergency Treatment, and Prevention
SELF-CHECK
A 4-week-old exclusively breastfed infant presents with a tense fontanelle, vomiting, and lethargy. He was born at home and received no medications at birth. CT scan shows a subdural haemorrhage. PT is 60 s, aPTT is 120 s, platelets are 310 × 10⁹/L. What is the diagnosis and what is the FIRST intervention?
A. Late VKDB with intracranial haemorrhage; give IV Vitamin K 1 mg immediately AND fresh frozen plasma 10–15 mL/kg
B. Classic VKDB; give IM Vitamin K only and wait for PT correction before imaging
C. Non-accidental injury; urgent child protection referral before any treatment
D. Bacterial meningitis with DIC; give broad-spectrum antibiotics and platelet transfusion
Reveal Answer
Answer: A. Late VKDB with intracranial haemorrhage; give IV Vitamin K 1 mg immediately AND fresh frozen plasma 10–15 mL/kg
A 4-week-old home-delivered exclusively breastfed infant with no birth prophylaxis presenting with intracranial haemorrhage and the coagulation profile of prolonged PT/aPTT + normal platelets = late VKDB. This is the most dangerous scenario — intracranial bleeding requires immediate dual-therapy: IV Vitamin K 1 mg (to trigger new factor synthesis over 4-6 hours) AND FFP 10-15 mL/kg (to provide immediate factor replacement while waiting for Vitamin K to work). Delaying treatment for child protection assessment or imaging would be inappropriate given the severity. Platelet transfusion is not indicated (platelets normal). This case is the direct consequence of missed birth prophylaxis.
Self-Assessment
Returning to the opening case: the 3-week-old exclusively breastfed infant born at home with no postnatal medications has late VKDB with intracranial haemorrhage. The coagulation profile (PT 45 s, aPTT 98 s, platelets 280 × 10⁹/L) is diagnostic — prolonged PT and aPTT with entirely normal platelet count and bleeding time points exclusively to Vitamin K-dependent factor deficiency. The precipitating factors are the complete picture: home birth, exclusive breastfeeding (low breast milk K1 content ~1-3 mcg/L), no prophylaxis at birth, age 3 weeks (the classic late-VKDB window of 2 weeks to 6 months). The single injection of 1 mg Vitamin K IM at birth — a five-second intervention costing almost nothing — would have completely prevented this intracranial haemorrhage and its lifelong neurological consequences.
Key examination recall points:
• VKDB early: within 24 hours; due to maternal drugs (phenytoin, rifampicin, warfarin)
• VKDB classic: day 2–7; breastfed, no prophylaxis
• VKDB late: 2 weeks to 6 months; breastfed/malabsorption; ICH in 30–50%
• Coagulation profile: prolonged PT AND aPTT, normal platelets and bleeding time
• PIVKAs: biologically inactive coagulation factors produced without Vitamin K
• Treatment: IV Vitamin K 1 mg + FFP 10–15 mL/kg for active/severe bleeding
• Prophylaxis: 1 mg IM at birth for ≥2.5 kg; 0.5 mg IM for <2.5 kg
• Breast milk Vitamin K: ~1–3 mcg/L (very low — cannot substitute for prophylaxis)
• Warfarin inhibits Vitamin K epoxide reductase (VKOR) — same pathway, applied pharmacology
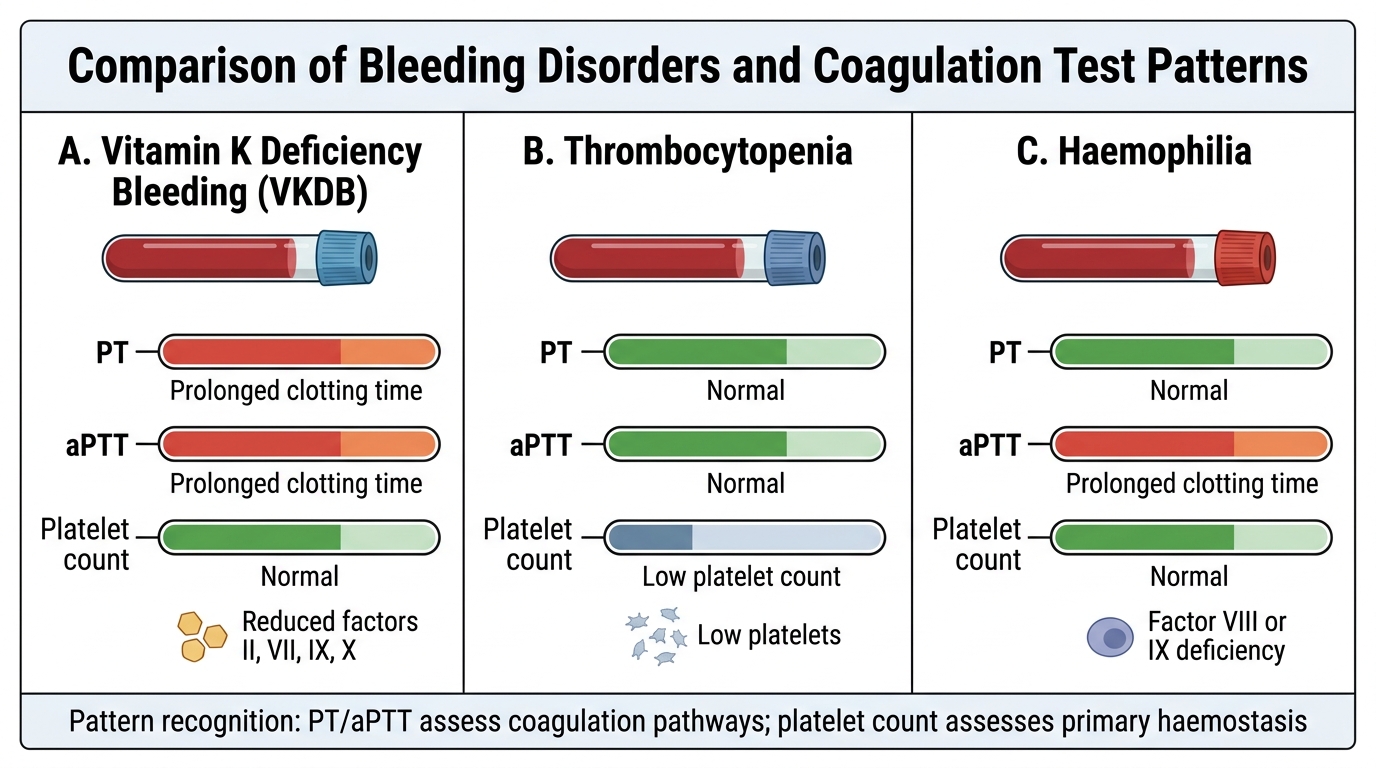
Coagulation Profiles: VKDB, Thrombocytopenia, and Haemophilia