Page 3 of 20
PE16.1 | IMNCI Framework — SDL Guide (Part 3)
IMNCI in India: HBNC, HBPNC and Field Implementation
India has extended the community arm of IMNCI through two programmatic elements: Home-Based Newborn Care (HBNC) and Home-Based Postnatal Care (HBPNC), both implemented by ASHAs with supervision from ANMs and medical officers.
HBNC is a package of home visits by the ASHA to assess, promote care for, and refer sick neonates in the first 28 days. The visit schedule under the MoHFW HBNC programme is: day 1 (within 24 hours of delivery at home or discharge from a facility after institutional delivery), day 3, day 7, day 14, and day 28. If a delivery is institutional, the day-1 visit occurs within 24 hours of discharge. At each visit, the ASHA assesses feeding (exclusive breastfeeding), thermal protection, cord care, danger signs (convulsions, fast breathing, inability to feed, hypothermia, jaundice), and birth asphyxia history. She records weight and uses the IMNCI danger-sign criteria to decide whether to manage at home (green), advise early facility visit (yellow), or refer urgently (pink).
HBPNC extends postnatal care to the mother as well — checking for puerperal sepsis, breast conditions, and mental wellbeing — recognising that maternal health directly impacts newborn feeding and care. ASHAs are incentivised under the JSSK and PMSMA programmes to complete these visits.
At the facility level, IMNCI case management is operationalised through a chart booklet kept at every PHC and sub-centre. ANMs, nurses, and MBBS officers are trained to use the chart during all sick-child consultations. Village Health, Sanitation and Nutrition Days (VHSNDs) are the convergence platform where IMNCI-trained AWWs and ASHAs deliver growth-monitoring, immunisation, and nutrition counselling to well children alongside sick-child referrals.
IMPORTANT: ASHA uses IMNCI-based danger-sign criteria during HBNC visits; she does NOT make treatment decisions independently — her role is to recognise danger signs and facilitate timely referral, or to counsel on home management for green cases.
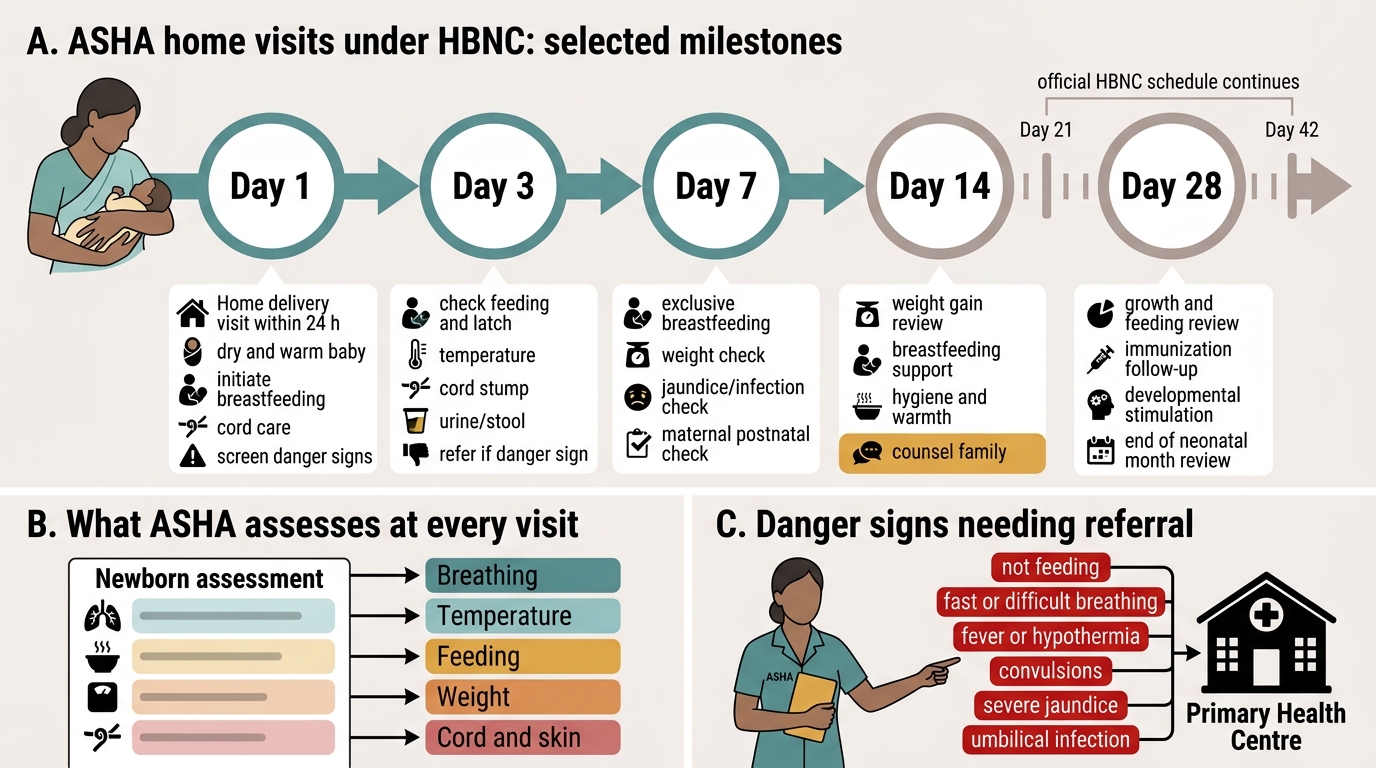
ASHA Home Visits Under HBNC
Evidence and Impact of IMNCI on Child Survival
The evidence base for IMNCI spans over two decades of field research across multiple countries and Indian states. The cornerstone evidence came from the WHO Multi-Country Evaluation of IMCI (MCE) study, which assessed IMCI implementation in Bangladesh, Brazil, Peru, Tanzania, and Uganda between 1997 and 2001. The study found that children in districts with full IMCI implementation (all three components) had a significantly lower risk of death (hazard ratio approximately 0.84 in some sites) compared to control districts, and that the quality of sick-child assessment improved substantially at IMCI-trained facilities. The key finding was that partial implementation — training alone without health-system strengthening and community-component delivery — produced smaller or negligible survival benefits.
In India, programme evaluations in states such as Rajasthan, Uttar Pradesh, and Jharkhand have shown that HBNC visit completion rates of ≥75% are associated with improved neonatal care practices and timely referral of sick neonates. The roll-out of IMNCI training to all levels of the public health system, combined with HBNC/HBPNC, has contributed to India's NMR decline from approximately 44 per 1,000 live births in 2000 to approximately 20 per 1,000 live births in 2020.
However, limitations and challenges persist:
• Training coverage gaps: a large proportion of PHC-level officers and ANMs in high-burden states have not completed formal IMNCI training.
• Drug supply disruptions: IMNCI management recommendations (zinc, oral amoxicillin, ORS) are often unavailable at the point of care.
• Referral barriers: distances, costs, and caregiver reluctance mean that even correctly identified pink-category children do not always reach the referral facility in time.
• Updating of protocols: the chart booklet has not been universally updated to reflect current antimicrobial recommendations (e.g., use of amoxicillin for non-severe pneumonia, which replaced co-trimoxazole in the Indian IMNCI update).
These limitations are recognised by MoHFW, and current NHM guidelines include IMNCI refresher training as a mandatory element of continuing medical education for PHC officers.
Self-Assessment
Self-assessment is the bridge between knowing the IMNCI framework intellectually and being able to apply it fluently at the bedside. The questions below are structured to test your ability to recall the three-component strategy, apply age-specific thresholds, execute the assess-classify-treat algorithm correctly, and understand the override rule that underpins patient safety. Work through each question independently before consulting the earlier sections. For questions that involve clinical vignettes, write out your classification and action before verifying against the IMNCI chart booklet — the goal is to build the automatic pattern recognition that a real clinical encounter demands, not just to confirm that you read the material. These self-check questions mirror the format used in NMC-aligned OSPE stations and short-answer examinations, so treating them seriously is a form of high-yield examination preparation.
- A health worker at a PHC is assessing a 14-month-old girl with fever for 4 days. Before classifying her fever, what step does the IMNCI algorithm mandate first, and why?
- List the three components of the IMNCI strategy and explain why all three must be functioning simultaneously for the programme to achieve a reduction in child mortality.
- A young-infant assessment reveals fast breathing (62/min) but no other abnormal findings. The mother says feeding is adequate. What is the IMNCI classification, and what action is taken?
- Explain the significance of the 'override rule' in the IMNCI colour-coded triage system with a clinical example.
- During an HBNC day-7 visit, the ASHA finds the neonate with an umbilical cord that is red and discharging pus. What action does IMNCI specify, and what pre-referral treatment should be given?
SELF-CHECK
Which of the following MOST accurately describes the three components of the IMNCI strategy?
A. Training health workers; providing vaccines; distributing ORS
B. Improving case-management skills; strengthening the health system; improving family and community practices
C. Diagnosing illness; prescribing medicines; following up patients
D. Preventing malnutrition; treating pneumonia; managing diarrhoea
Reveal Answer
Answer: B. Improving case-management skills; strengthening the health system; improving family and community practices
The three official WHO/IMNCI components are: (1) improvement in case-management skills of health workers (facility level training); (2) strengthening health system (drug supply, referral, supervision); (3) improving family and community practices (ASHA/AWW counselling, HBNC, demand-side behaviour change). Options A, C, and D describe elements within these components but do not represent the three strategic pillars.