Page 5 of 20
PE16.{2,5} | IMNCI Young Infant Assessment — SDL Guide
Learning Objectives
- Demonstrate the step-by-step IMNCI assessment procedure for the young infant (birth to <2 months)
- Identify clinical signs of Possible Serious Bacterial Infection (PSBI) in a young infant
- Distinguish PSBI from local bacterial infection and physiological conditions using IMNCI criteria
- Classify a young infant using the colour-coded IMNCI triage system (pink/yellow/green)
- Identify and stratify risk in a sick neonate using IMNCI guidelines
- Describe the pre-referral treatment for a pink-classified young infant and counsel the mother appropriately
INSTRUCTIONS
The young infant (birth to <2 months) is the most biologically vulnerable patient a clinician will ever encounter. Neonatal sepsis can progress from mild signs to cardiovascular collapse within hours. Physiological jaundice looks identical to haemolytic jaundice at the bedside. A baby who appears to be sleeping may be lethargic. The IMNCI young-infant algorithm was specifically designed to prevent these mistakes by forcing a systematic, eyes-first assessment before any history-biased pattern recognition can take over. Mastering this algorithm is a core practical competency for every MBBS graduate practising in primary-care India — and is tested in OSCE/OSPE-format NMC exit examinations.
References
- Ghai Essential Pediatrics, 9th edition, Ch 7 (Care of the Newborn) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 107 (Infections of the Neonatal Infant) (textbook)
- MoHFW India — IMNCI Training Module 1: Young Infant (guideline)
- WHO — Pocket Book of Hospital Care for Children, 2013 (guideline)
- Young Infants Clinical Signs Study (YICSS), Lancet 2008 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 12-day-old baby girl is brought to the sub-centre by her grandmother. The mother is still in bed after a home delivery five days ago. The grandmother says the baby has not been feeding well for the last 24 hours, seems sleepy, and the navel area looks a bit red. You observe the baby before you even touch her. She is lying still — not crying, not moving spontaneously. Her breathing is fast. You count 68 breaths per minute. The umbilicus is red, with redness extending 2 cm onto the abdominal skin. Her axillary temperature is 38.1°C. There are no skin pustules. You are looking at a 12-day-old with fast breathing, fever, umbilical infection with skin spread, and lethargy. What is your IMNCI classification? What do you do in the next 10 minutes?
WHY THIS MATTERS
Neonates account for approximately 45% of all under-5 deaths globally, and the majority of those deaths occur in the first week of life — the period of maximum biological vulnerability. Neonatal sepsis, which may present with only a few non-specific signs (poor feeding, temperature instability, fast breathing), carries a case fatality rate of 30–50% when treatment is delayed beyond six hours of sign recognition. The IMNCI young-infant algorithm exists because no heuristic or gestalt clinical approach reliably detects serious illness in young infants without a structured checklist — field studies demonstrated that health workers using unstructured assessment missed PSBI in a significant proportion of cases. For you as an MBBS graduate posted to a PHC, sub-centre, or district hospital, the ability to assess a young infant correctly using IMNCI is a life-saving clinical skill — not a protocol formality.
RECALL
Activate the following prior knowledge before engaging with the assessment procedure:
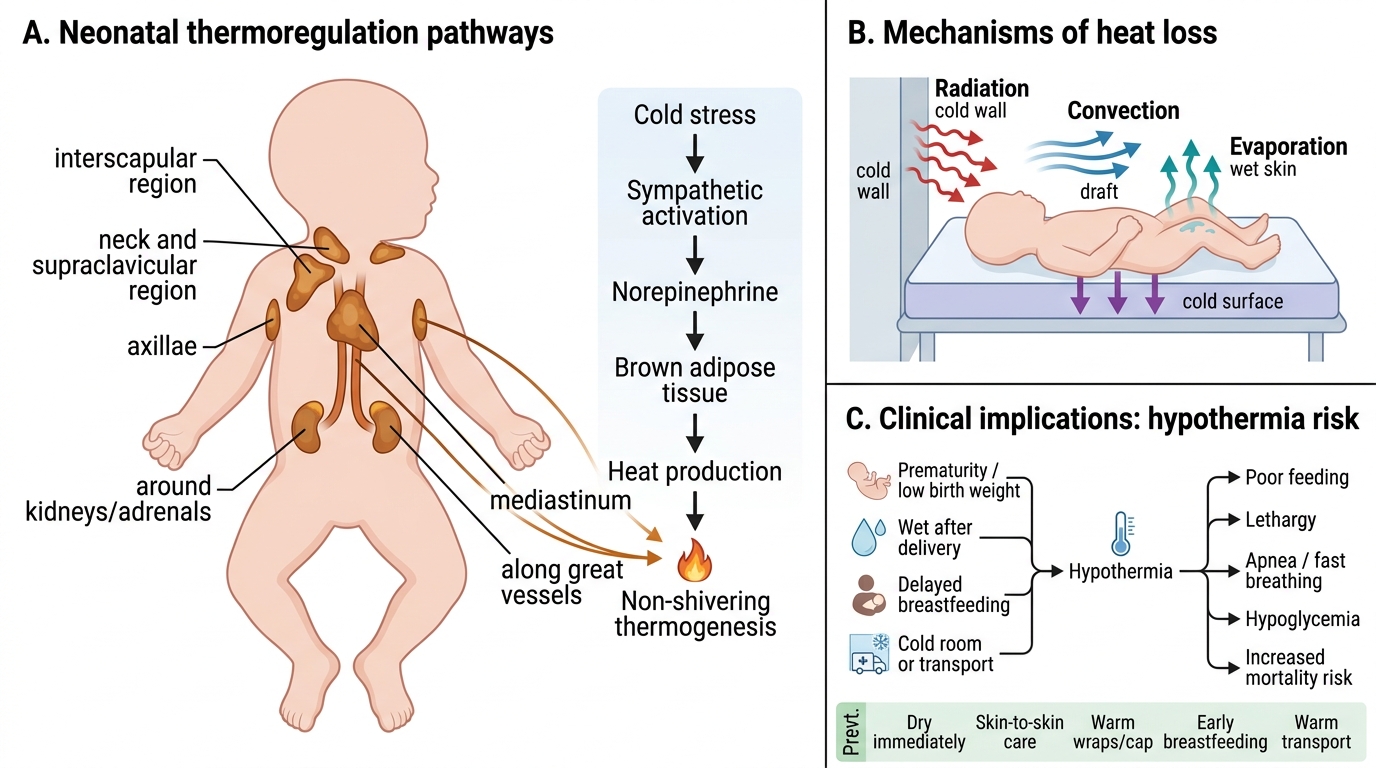
- Neonatal physiology (PY): young infants cannot shiver — they rely on brown adipose tissue (BAT) non-shivering thermogenesis for heat; they have a high surface-area-to-mass ratio predisposing to rapid heat loss. Thermoregulation failure leads to cold stress → metabolic acidosis → sepsis risk.
- Jaundice physiology: physiological jaundice appears day 2–3, peaks day 4–5, resolves by day 14 (term); jaundice appearing within 24 hours is always pathological (haemolytic until proved otherwise); jaundice extending to palms and soles is severe regardless of age.
- APGAR score (from PY/OG): used at 1 and 5 minutes after birth to assess transition — NOT a disease-severity tool after the delivery room. Do NOT use APGAR when assessing a 12-day-old sick baby.
- Neonatal immune immaturity: maternal IgG transfers transplacentally after 32 weeks — preterm infants have less passive immunity. Immature neutrophil reserves mean bacterial infection rapidly overwhelms defences.
- Breastfeeding mechanics: a neonate unable to latch or suck effectively may present to you as 'not feeding well' — assess latch and suck as part of the feeding assessment in the IMNCI algorithm.
Clinical Indication: Why the Young Infant Requires a Separate Algorithm
The IMNCI programme uses two distinct age-band algorithms — one for young infants (birth to <2 months) and one for children aged 2 months to 5 years — because the clinical presentation, danger-sign spectrum, diagnostic thresholds, and management principles differ so fundamentally between these groups that a single algorithm would produce dangerous classification errors.
Six biological and clinical reasons justify the separate approach. First, signs of serious illness in young infants are non-specific and overlap with normal variation: a well neonate may have irregular breathing with brief pauses; an early septic neonate may breathe regularly but at a higher-than-normal rate. This overlap means only threshold-based, counted respiratory rates (not clinical impression) can reliably detect fast breathing. Second, clinical deterioration is rapid: a young infant with PSBI who is yellow-category (local infection, treatable at PHC) at 9 am may be in septic shock by noon if a second sign — say, reduced feeding — was not elicited on the initial assessment. Third, fever thresholds differ: fever in a child 12 months old has a high prior probability of viral illness; fever ≥37.5°C axillary in a neonate has a high prior probability of serious bacterial infection. Fourth, normal physiological findings in older children are abnormal in neonates: jaundice is physiological in a 4-day-old but pathological if it extends to palms/soles or appears at day 1. Fifth, feeding inability is pathological in neonates: an older child who is not eating may be feeding less due to sore throat; a neonate who cannot breastfeed or take 3/4 of a normal feed is showing a danger sign. Sixth, immunisation status matters acutely: a neonate who did not receive BCG, OPV-0, and Hepatitis B at birth is at additional risk for vaccine-preventable complications.
The clinical indication for applying the IMNCI young-infant assessment is ANY sick young infant presenting to or visited at home by an ASHA, ANM, or medical officer — or any newborn on a HBNC visit who the ASHA identifies as feeding poorly, not breathing normally, having a temperature abnormality, or appearing unwell.
Governing Principles: Anatomy, Physiology and IMNCI Design Logic
The IMNCI young-infant algorithm is structured by three governing physiological principles that any practitioner must understand to apply it correctly, rather than as a rote checklist.
Principle 1 — Thermoregulation is critical and fragile. Young infants have a high surface-area-to-body-mass ratio, minimal subcutaneous fat for insulation, and cannot shiver. Their primary heat-generating mechanism is non-shivering thermogenesis via brown adipose tissue (BAT) — BAT is concentrated in the interscapular region, around the kidneys, and in the mediastinum, and generates heat by uncoupled mitochondrial respiration. Cold stress rapidly depletes BAT and glucose reserves, leading to metabolic acidosis and impaired immune function. This is why IMNCI defines hypothermia as <35.5°C axillary (more conservative than the adult threshold) and mandates that temperature be measured using a correctly positioned thermometer, not estimated by touch. Conversely, fever ≥37.5°C in a young infant is not benign — the threshold for bacterial infection investigation is lower than in any other age group.
Principle 2 — Immune deficiency is structural. The young infant's immune system has three critical gaps: (a) immature neutrophil production with limited bone-marrow reserve; (b) absent or low secretory IgA at mucosal surfaces; (c) limited transplacental IgG in preterm infants (transfer peaks after 32 weeks). Maternal fever, chorioamnionitis, Group B Streptococcus colonisation, or prolonged rupture of membranes represent risk factors that compound this structural gap and make early-onset sepsis more likely. IMNCI assesses these perinatal risk factors through its history-taking component.
Principle 3 — The eyes-first, count-first discipline. IMNCI mandates observing the infant before touching it — because examination-related disturbance raises respiratory rate and can mask or provoke signs that would otherwise be evident. The respiratory rate must be counted for a full 60 seconds using a watch, NOT estimated by observation alone. Studies have repeatedly shown that clinical estimation of respiratory rate in neonates is unreliable — the only accurate method is a timed count with the infant undisturbed and the chest or abdomen visible. This procedural discipline is built into the algorithm as a non-negotiable first step.
Neonatal Thermoregulation and Hypothermia Risk
Step-by-Step Assessment of the Young Infant
The IMNCI young-infant assessment follows a fixed, ordered sequence designed to maximise yield while minimising examiner interference with the infant. Each step must be completed before moving to the next — skipping steps based on the chief complaint is the most common source of missed diagnoses in neonatal primary care.
Step 1 — Ask history (without disturbing the infant): chief complaint and duration; feeding ability (is the baby breastfeeding? how many times in the last 24 hours? does the baby latch and suck effectively?); convulsions (parents often do not volunteer convulsions unless asked directly — ask specifically about 'fits', 'jerking of arms/legs', 'staring'); movements (is the baby moving less than usual?).
Step 2 — Observe (before touching): Does the infant move spontaneously? Is breathing visible (count — see Step 3)? Is there chest indrawing? Is there jaundice visible (look at face, chest, abdomen, palms, soles)? Observe umbilical area — redness, discharge?
Step 3 — Count respiratory rate for 60 seconds: Using a watch (with second hand or a stopwatch). Count chest or abdominal excursions for a full 60 seconds. Fast breathing threshold in young infants = ≥60 breaths/minute. If fast breathing is detected, count a second time to confirm before classifying. An anxious infant being disturbed may show transiently elevated rates — two counts reduce misclassification.
Step 4 — Check for severe chest indrawing: defined as inward movement of the lower chest wall (bony thorax) on inspiration — NOT just subcostal soft-tissue retraction (which is normal in young infants due to chest-wall compliance). Severe chest indrawing is a PSBI sign regardless of respiratory rate.
Step 5 — Measure temperature: axillary temperature using a thermometer for 3 minutes. Fever ≥37.5°C or hypothermia <35.5°C = PSBI sign.
Step 6 — Look at umbilicus: Is there redness, swelling, or pus discharge? If redness is present, does it extend onto the abdominal skin? Mark extent with a pen if available (to monitor progress or referral notes).
Step 7 — Count skin pustules: inspect the entire skin surface including scalp folds, axillae, groin. Count total pustules. ≥10 pustules or any bulla (fluid-filled vesicle >5 mm) = PSBI sign. <10 pustules without other PSBI signs = local bacterial infection (yellow).
Step 8 — Check for jaundice: inspect in good natural light. Start at face/sclera, progress to chest, abdomen. If jaundice is visible: blanch the skin with a finger to reveal the underlying skin colour. If palms/soles are yellow = severe jaundice (pink). Determine timing: did jaundice appear within the first 24 hours of life?
Step 9 — Assess feeding: offer the breast or watch the mother feed. Assess attachment (chin touching breast, most of areola in mouth, lower lip turned outward). Count sucking — is the suck effective? A baby who is not feeding OR taking less than 3/4 of the usual amount = feeding problem.
Step 10 — Assess weight: weigh using infant scale. Low birth weight (<2500 g) and very low birth weight (<1500 g) affect management. If current weight is unavailable, use birthweight record.
Step 11 — Check immunisation status: Has BCG, OPV-0, and Hepatitis B-1 been given at birth? If not given, is there a contraindication (jaundice — delay BCG; sepsis — delay all vaccines until recovered)?
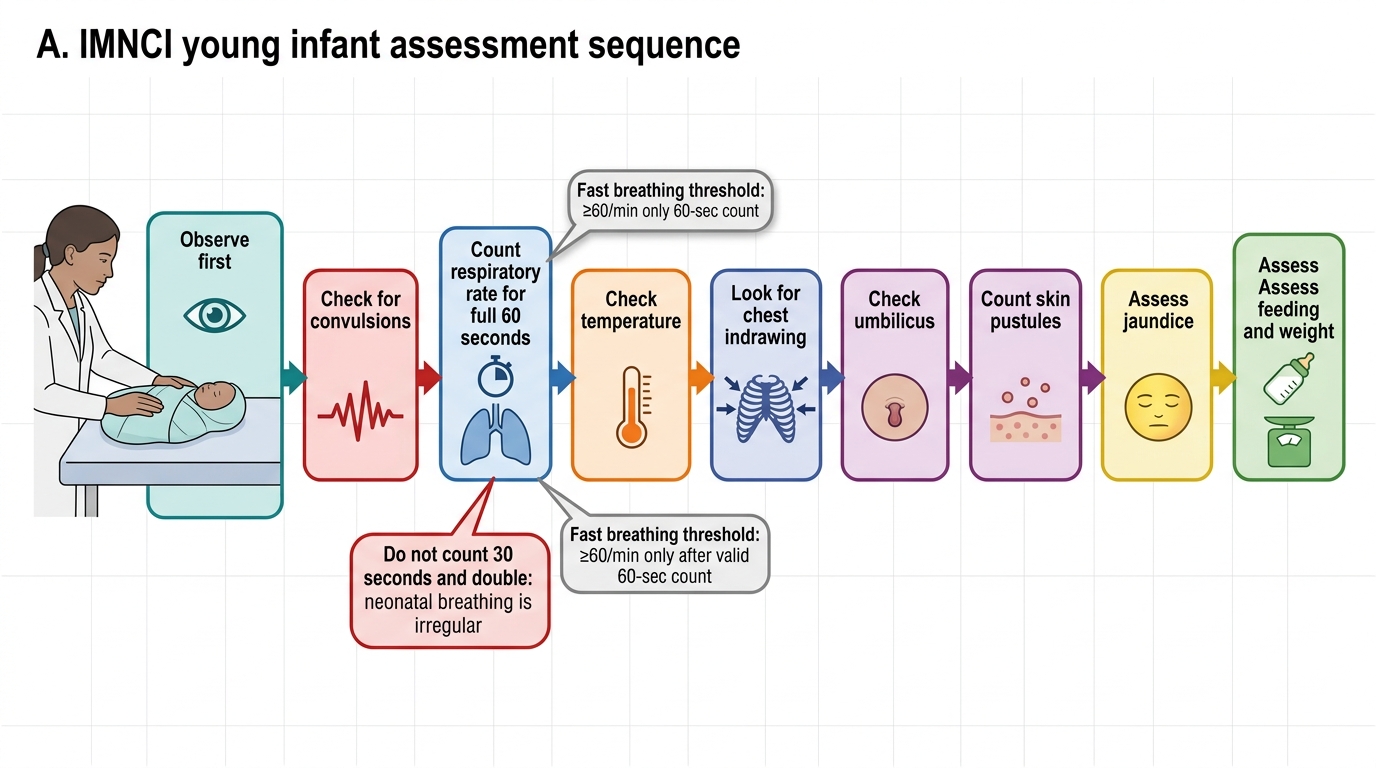
IMNCI Young Infant Step-by-Step Assessment Sequence
SELF-CHECK
You are counting the respiratory rate in a 3-week-old infant. After counting for 30 seconds you get 28 breaths — you double it to estimate 56/min. Is this an acceptable technique and what is your classification?
A. Acceptable — 56/min is below the threshold of 60/min so no fast breathing, continue assessment
B. Not acceptable — IMNCI mandates counting for a full 60 seconds; repeat the count before classifying
C. Acceptable — 56/min is borderline, classify as fast breathing and refer
D. Not acceptable — you should estimate respiratory rate visually without counting
Reveal Answer
Answer: B. Not acceptable — IMNCI mandates counting for a full 60 seconds; repeat the count before classifying
IMNCI mandates a full 60-second count for respiratory rate in young infants — this is non-negotiable. A 30-second count doubled introduces error because neonatal breathing is irregular (periodic breathing with brief pauses is normal in neonates). Doubling a 30-second count can yield falsely elevated rates. The correct approach is to recount for a full 60 seconds. Until you have a valid 60-second count, you cannot classify breathing as fast or normal.